Tibial plateau fractures account for 1% of all fractures and exhibit a bimodal distribution, with a peak occurrence in young patients due to motor vehicle crashes or bumper strike injuries resulting in proximal tibial intra-articular fractures. These fractures can also be seen in elderly patients with osteoporotic bones who experience less severe trauma [1,2].
One of the most typical intra-articular fractures is the proximal tibial plateau fracture, which can result from either direct trauma in an axial compressive pattern or indirect trauma in a coronal fracture pattern [3]. These fracture patterns are very complex and may impact either the medial or lateral tibial plateaus, or even both. Understanding the type of injury, such as ligament injuries, meniscal tears, and high or low-energy trauma, can facilitate the course of therapy for these fractures [3].
The clinical management of complicated tibial plateau fractures still remains a challenge. These fractures are commonly referred to as C-type injuries when using the Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification [4] or as type V and VI when using the Schatzker classification [5]. High-energy fractures of the type V and VI Schatzker types are frequently associated with additional local and systemic damage. High-energy tibial plateau fractures can be treated with a variety of techniques, such as intramedullary nailing [6], dual plating [7], and definitive external fixation [8], although the most effective course of care is still up for debate. Multiple surgical techniques and fracture fixation methods have been devised to treat these fractures. The open reduction and internal fixation procedures for each tibial plateau help in preserving anatomic articular congruity, restoring mechanical alignment, and enabling early knee joint mobilisation. These open reduction and internal fixation procedures, particularly when carried out through damaged soft-tissues, have occasionally been linked to serious wound complications [9].
Every fracture is unique in its shape and requires individualised care. Tibial plateau fractures are often treated using two-dimensional classification methods. Several authors have suggested that treating tibial plateau fractures requires considering the fracture in three dimensions using Computed Tomography (CT) [10,11]. The standard recommendation for the definitive fixation of this type of fracture is bi-columnar dual plating [12-15]. However, there are situations in which, in addition to fractures of the tibial condyles, a thin-profile distal fibular plate was employed for repairing the tibial tuberosity avulsion fractures [16].
The present study used a thin, contoured fibular plate for the tibial tuberosity to minimise hardware prominence. The optimal placement is directly anterior over the tibial tuberosity. Soft-tissue is dissected medially to visualise the patellar tendon and distally to its insertion at the tibial tuberosity through anteromedial or anterolateral incisions for bicondylar fracture fixation. The present study aimed to evaluate the clinical outcomes as well as the radiological results of bi-columnar plating combined with additional thin distal fibular plating for the tibial tuberosity in complex proximal tibia Schatzker type 5 and 6 fractures with additional tibial tuberosity fractures.
Materials and Methods
The prospective study was conducted at the Orthopaedics Department of Saveetha Institute of Medical and Technical Sciences (SIMATS), Chennai, Tamil Nadu, India, from January 2017 to January 2022 on 18 patients after obtaining approval from the Ethics Committee (117/06/2022/IEC/SMCH). The informed consent was obtained from the patients.
Inclusion and Exclusion criteria: Patients of either gender aged from 18 to 80 years, with Schatzker classification type V or VI with tibial tuberosity avulsion fractures diagnosed by X-ray and Computed Tomography (CT) scan of the knee joint, closed or Gustilo I/II/IIIA/IIIB open fractures, and patients willing to come for follow-up, fractures less than two-week-old were included. Patients aged less than 18 or more than 80 years, fractures more than two-week-old, patients with pathological fractures, open growth plates, individuals suffering from serious head injuries with a Glasgow Coma Scale (GCS) <8, mental retardation, drug addiction, or other neurological problems that might impede rehabilitation, severe systemic diseases, such as uncontrolled diabetes mellitus, chemotherapy, aggressive malignancy, or renal failure, Gustilo grade IIIC fractures, patients with fractures in any ipsilateral or contralateral limbs, and those who were not willing to participate or come for follow-up, were excluded.
Sample size calculation: Out of the total 20 patients initially included in the study, two were lost to follow-up. Therefore, the final sample included eighteen patients with tibial plateau fractures (Schatzker type V or VI) associated with tibial tuberosity avulsion fractures. Tibial tuberosity plating with a thin profile distal fibular plate was performed, and all patients received bi-columnar plating.
Study Procedure
A plaster slab or knee immobiliser was used to splint the injured limb. Following their medical condition, the state of the skin around the fracture, and the degree of swelling, the patients underwent surgery as early as possible. When there was significant soft-tissue swelling, the patient was placed in a knee-spanning external fixator or distal tibial skeletal traction was applied until the soft-tissue condition improved. The wrinkling of the skin around the proximal tibia, healing of fracture blisters, and decreased oedema were the clinical signs of soft-tissue recovery. Every procedure was performed under the guidance of an image intensifier on a C-arm.
All the patients underwent surgery under either general or regional spinal anaesthesia. Cefuroxime 1.5 mg intravenously was initiated half an hour before the administration of anaesthesia. During the surgery, an inflated tourniquet was used in each patient. Patients were positioned supine on a radiolucent table with a sandbag placed under the ipsilateral gluteal region. If a posteromedial approach was planned, the sandbag was placed on the contralateral hip side.
The medial column is often fixed first. Initially, the lateral column was reconstructed when the medial condyle was severely comminuted. In cases where the fragment was posterior, an open posteromedial approach was employed. By adequately retracting the gastrocnemius and pes anserinus, the posteromedial fragment was made visible. The anatomical reduction was achieved by adequately visualising the fragment. Fracture reduction was confirmed under fluoroscopic guidance. Then, a 3.5-mm medial proximal tibial Locking Compression Plate (LCP) or T buttress plate was used to hold the reduced fracture in place. For the anterolateral technique, a lazy ‘S’ incision was made parallel to the tibial shin, just lateral to the tibial tuberosity. Anatomical lateral locking plates, ‘L’ shaped buttressing plates, or lateral tibial raft plates were fixed to the lateral surface after achieving satisfactory reduction under the C-arm. Tibial tuberosity avulsions were fixed with thin-profile distal fibular plates in buttressing mode for all patients [Table/Fig-1a-c]. A contralateral thin-profile distal fibular plate was utilised to provide a buttressing effect. This plate was preferred as it could sit flush over the tibial tuberosity, offering a broad buttressing effect on the tuberosity fragment. Other precontoured plates did not sit flush over the tuberosity fragment. The intraoperative images showing plating has been depicated in [Table/Fig-2]. CT knee images with Schatzker type V fracture and tibial tuberosity avulsion fracture has been depicted in [Table/Fig-3].
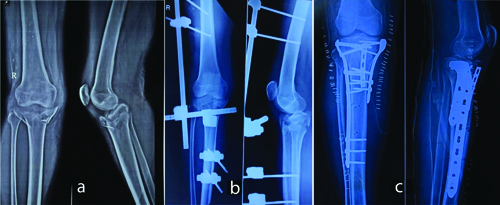
X-rays of right knee joint (a) Preoperative (b) Postoperative spanning external fixator and (c) Post operative after bicoumnar planting along with thin distal fibular planting.
Intraoperative images following plating.

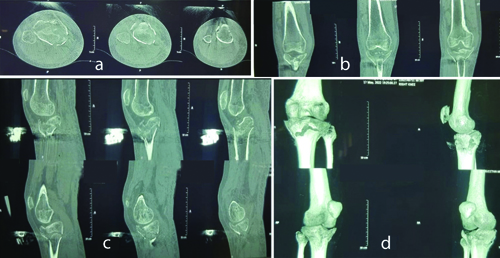
CT knee images with Schatzker type V fracture and tibial tuberosity avulsion fracture (a) Axial section, (b,c) Coronal section and (d) 3D reconstruction image.
Patients were monitored postoperatively to track recovery and detect any issues. Radiographs were used to assess the effectiveness of articular reduction, metaphyseo-diaphyseal reduction, and alignment. In cases of remaining instability postsurgery, a hinged knee brace was recommended. Static quadriceps strengthening activities and non weight-bearing walking were initiated on the first postoperative day. Non weight-bearing mobilisation was performed using a walking frame or axillary crutches. Active assisted knee bending and quadriceps exercises began on the second postoperative day.
Fracture healing progress and knee joint Range of Motion (ROM) were monitored. The functional outcome of the patients was assessed over a one-year period using the Knee Society knee scoring system [Table/Fig-4] [15].
Clinical images showing knee range of movements in a 30-year-old male patient at 12-month postsurgery.

Statistical Analysis
Descriptive statistics were used to compute means, standard deviations, and ranges. The Statistical Package for Social Sciences (SPSS) version 11.0 was used to analyse the data. Student’s t-tests and ANOVA were used to compare two means. Correlations were analysed using the Pearson’s correlation coefficient. A p-value of 0.05 was considered statistically significant.
Results
The average age of the study population was 39.4±5.6 years. Road Traffic Accident (RTA) was the most frequent mode of injury in 14 (77%) individuals. Within the study group, no perioperative problems were recorded. The surgery took 114±10.4 minutes on average, and 146±40 mL was the average blood loss recorded throughout the procedure [Table/Fig-5].
Mode of injury, average duration of surgery and average blood loss in surgery.
| Mode of injury | Average duration of surgery (Min) | Average blood loss in surgery (mL) | Average bone union time (weeks) | Average time to full weight bearing (weeks) |
|---|
| Road traffic accident | 14 (77%) | 114±10.4 | 146±40 | 12.7 | 15.8 |
| Slip and fall | 2 (11.1%) |
| Fall from height | 2 (11.1%) |
After an average duration of 12.4 weeks (range: 11-15 weeks), radiographic bone union was seen in 16 individuals, with union occurring between 10 and 14 weeks [Table/Fig-5]. Every patient exhibited outstanding healing. The average time to begin full weight-bearing was 15.8 weeks (range: 12-24 weeks) [Table/Fig-5]. Two patients showed signs of union in further follow-ups after 14 weeks. There were no complaints of anterior knee pain. The Knee Society score at 12 months postoperatively was excellent at 93.6 (range 92 to 98). The affected knees exhibited an average Range of Motion (ROM) between 90.3 and 120.1 degrees. One patient developed a wound-related complication in the form of a superficial skin infection, which was treated with antibiotics and eventually subsided. One patient developed postoperative screw loosening for which screw exit was done. Another case had a 2° varus deformity and had a good functional score at the end of the follow-up.
Many radiographic abnormalities were observed, such as varus collapse, expansion and depression of the articular surfaces, preservation of fracture reduction, union in cortex or trabeculae across the fracture site, and evidence of subsequent osteoarthritis.
The union of bone was defined as “The union of at least three cortices in the Anteroposterior (AP) and lateral views, on follow-up radiographs”. There was no mortality reported during the study period. Knee society scoring at 12 months postoperatively was 88%, which falls in the excellent criteria, and 12% of patients were in the good category.
Discussion
The present study explores a new surgical technique for treating complex tibial plateau fractures. Current methods prioritise stable fixation of the fracture but can limit knee mobility. The most common cause of complex tibial plateau fractures is high-energy trauma. The comminution that follows makes it challenging to analyse fracture patterns. The fractures are categorised by the Schatzker and AO/OTA classifications based on how they appear on anteroposterior radiographs [3,5]. In present study, the use of additional thin-profile plates alongside traditional medial and lateral plates for the tibia was examined. A fibular plate, which is thin in profile and can be contoured to accommodate the tibial tuberosity, was also considered. Another advantage of using a thin fibular plate is that it reduces hardware prominence. The goal was to achieve both stable fixation and early knee movement, potentially leading to improved patient outcomes. The best site for the fibular plate, according to the study, is directly anterior to the tibial tuberosity. Through the anteromedial or anterolateral incisions made for bicondylar fracture fixation, soft-tissue dissection can be done medially until the patellar tendon is visualised, and fine dissection can be done distally to its insertion at the tibial tuberosity.
In present study, the average union time was 12.7 weeks. In other Zhang Y et al., studies, an average of 14.1 weeks was reported for the bi-columnar cohort [17]. Fracture union was observed to occur between 8 and 22 weeks, with an average of 14 weeks, according to Prasad GT et al., [18]. The treatment of tibial tuberosity avulsion fractures with additional thin-profile distal fibular plates and the stiff fixation of the proximal tibia utilising medial and lateral plates allowed for early knee mobilisation [18].
Knee society scoring was conducted, revealing 88% excellent and 12% good outcomes after a 1-year follow-up in 16 patients who underwent thin distal fibular plating for tibial tuberosity avulsion fractures. This outcome was comparable to the study conducted by Rohra N et al., where patients with Schatzker type V and type VI fractures received bi-columnar plating, resulting in almost 70% of patients with excellent and 23% with good knee scores. The bi-columnar tibial plates used on the medial and lateral aspects have been in use for a considerable period. Notably, the avulsion injuries anteriorly were not addressed [Table/Fig-6] [19].
Comparison of Knee Society Scores at 1-year follow-up with the study conducted by Rohra N et al., [19].
| Grade | Rohra N et al., [19] (%) | Present study |
|---|
| Excellent (80-100) | 24 (70%) | 16 (88%) |
| Good (70-79) | 8 (23%) | 2 (12%) |
| Fair (60-69) | 1 (2.9%) | 0 |
| Poor (<60) | 1 (2.9%) | 0 |
| Total | 34 | 18 |
Early knee mobilisation was facilitated by the use of medial and lateral plates for stiff fixation of the proximal tibia and additional thin-profile distal fibular plates for treating tibial tuberosity avulsion fractures. Weight-bearing is typically postponed until X-rays show signs of union (usually between 12 and 16 weeks). Acute arthritic changes, metaphyseo-diaphyseal alignment, and articular congruity were assessed using AP and lateral plane radiographs of the knee joint and leg.
Severe comminution can cause malalignment and wound dehiscence in high-intensity intra-articular tibial plateau fractures. A delay in healing may lead to implant failure, varus collapse, and arthritis in the knee joint [20,21]. Various techniques have been proposed for repairing fractures, including bi-columnar plating using Minimally Invasive Percutaneous Plate Osteosynthesis (MIPPO) procedures, external fixation, hybrid fixators, plating through a single midline incision, plating using Mercedes Benz incisions, and plating through two incisions. To regain good Range of Motion (ROM) and to avoid progressive osteoarthritis, secure internal fixation with restoring articular congruity and ligament restoration are crucial. Open reduction of the fracture and fixation with plates should be done as soon as possible after the accident, ideally within four hours, or preferably one week later when the oedema and related inflammatory reactions have subsided. Patients underwent surgery after an average waiting period of 3.5 days.
However, present study addresses proximal tibial avulsion fractures using the buttress technique. The avulsed fragments are usually difficult to manage and control. Thin profile distal fibular plates were used for addressing these types of fractures. These thin profile plates also had excellent results concerning skin healing due to their less prominence over the bony aspects of the anterior tibia.
The present study investigated the treatment of complex tibial plateau fractures with a focus on achieving good knee function. The study found that using a combination of medial and lateral plates for the tibia and additional plates for tibial tuberosity avulsion fractures allowed for early knee movement after surgery.
Limitation(s)
The insufficient follow-up period might not capture long-term effects or outcomes. The sample size was small, which was not calculated. This might influence the results. A longer duration study with a wider patient population and an appropriate control group will be better to validate the outcome of present study.
Conclusion(s)
A unique thin-profile distal fibular plating technique for tibial tuberosities may be an effective treatment for difficult proximal tibia Schatzker type V and VI fractures with tibial tuberosity avulsion fractures. Columnar plates combined with open reduction and internal fixation through two incisions with thin distal fibular plates produce excellent/good functional results. This innovative and safe technique helps provide sound fixation and stability for faster and early mobilisation without any anterior knee pain and promotes quicker fracture healing. Appropriate timing of the operation, excellent extraperiosteal dissection, and avoiding dissection of comminuted bone fragments can all help minimise postoperative problems.