Periodontitis is a disease of tooth supporting tissues which often results in exposure of the root surface to the oral environment. The exposed root cementum with plaque and calculus undergoes a variety of changes like hyper or demineralised surface, loss of collagen cross-banding and contamination with endotoxins [1]. Although mechanical techniques were frequently used for root decontamination, they leave a surface smear layer made up of organic and inorganic particles acting as a barrier for periodontal wound healing. It has been proposed that root bio-modifiers are the demineralising acids that when applied on the root surface exposes the collagen fibers within the root matrix and removes the endotoxin. This aids in the attachment of connective tissue cells to the root surface which is critical for re-establishment of periodontal apparatus [2,3].
According to Bhushan K et al., the root surface biomodification agents are broadly classified into [4]. Root conditioners like CA, tetracycline, Hcl, EDTA, fibronectin, laminin, doxycycline, minocycline, polyacrylic acid, phosphoric acid, formalin, chlorhexidine, hydrogen peroxide, cetyl pyridium chloride and Sodium-n-Lauryl sarcosine, Cohn’s factor, Bile salts and plasma fractions, enamel matrix proteins, platelet rich plasma, recombinant human growth factors, hyaluronic acid, lasers.
Among the above-mentioned agents, CA is the gold standard and is being used routinely for periodontal therapy [5,6].
Lan WC et al., in his study on the effect of CA on gingival fibroblast culture, observed that 47.6 mmol/L CA at a pH of 3.8 resulted in gingival cell death. Clinically, irrational use of the root conditioner or insufficient flushing of the same may also result in such an outcome on the surgical flap. So, they concluded that a conditioning agent with the least cytotoxicity would be a better choice than CA in regenerative periodontal therapy [11].
ACV, an organic nutraceutical with numerous health advantages, is produced by the alcoholic fermentation of apples. It is a rich source of flavonoids, vitamins, minerals, polyphenolic chemicals, and organic acids. Lactic acid, CA, malic acid, succinic acid, acetic acid, and formic acid are some of the organic acids found in ACV. The ACV products have pH values that vary from 2.83 to 3.21. It is listed on the Generally Recognised As Safe (GRAS) list [12]. Natural food-borne acetic acid (ACV), which has been shown to have several medical benefits, including antibacterial, anti-inflammatory, and antioxidant activity, is being used as an intracanal irrigant due to its effectiveness in disinfecting canals and removing smear layers [13]. Among varying concentrations of ACV (100, 75, 50, and 25%) the presence of acetic acid in 75% ACV demineralised the smear layer better around the dentinal tubules [14]. ACV also demonstrated a promising antibacterial action against oral pathogens that cause endodontic infections, such as Enterococcus faecalis, Streptococcus, and Staphylococcus [15,16].
To the beset of our knowledge, no research has been done on the impact of ACV as a root biomodification agent on teeth with periodontal disease. Therefore, this pilot study was to assess the smear layer removal and fibrin clot adhesion of ACV in comparison to CA by Scanning Electron Microscopy (SEM) on periodontally affected teeth.
Materials and Methods
This pilot study was conducted at Sri Venkateswara Dental College and Hospital, Chennai, India, for three months, starting in January 2024 and ending in March 2024. The study commenced after receiving approval from the institutional ethical committee (IEC/SVDCH/2412). The study involves only 16 samples in total, with eight teeth in each group. The aim of the research was to determine the smear layer removal and fibrin clot adhesion of ACV compared to CA on periodontally infected teeth.
Preparation of the sample: A total of eight teeth extracted due to advanced periodontitis were procured for sample preparation. The teeth were scaled using ultrasonic scaler under copious saline irrigation. Further i root planning was done to remove the infected cementum using Gracey curettes (Hu-Friedy) #1-2, 3-4 [Table/Fig-1].
Scaling and root planing of extracted tooth using Gracey curette.
Using a diamond disc with saline irrigation, the root was first sectioned transversely at the Cemento-Enamel Junction (CEJ) [Table/Fig-2] and at the intersection of the middle and apical one-third. The apical thirds of the roots and the anatomic crown were eliminated. Dentin blocks were formed by longitudinally slicing the central portion of the root stumps to buccal and lingual halves. Each dentin block was prepared to a dimension of 4 mm by 6 mm [Table/Fig-3]. A total of 16 dentin block samples were obtained, of which eight underwent CA testing (Control group) and eight underwent ACV testing (Test group) [Table/Fig-4]. Within each group, four samples were assessed for smear layer removal, and the remaining four samples were evaluated for fibrin clot adherence.
Transverse slicing of the tooth at the level of CEJ.

Labial and the lingual surface of the sample after slicing.


CA crystals were procured and dissolved in water to prepare a solution with pH of 1. Commercially available ACV (Bragg) with 5% concentration was obtained and pH tested. The pH of both the preparations was assessed by litmus test. The final pH of CA and ACV were one and three, respectively.
The agents were applied according to the protocol adopted by Chahal GS et al., The agents were applied with little pressure, which allowed them to moisten the surface without overly burnishing on the samples for three minutes with a cotton pellet. The pellet was changed every 30 seconds. Following treatment, samples were rinsed thoroughly with distilled water [17]. For the evaluation of fibrin clot adhesion eight of the samples alone received a drop of fresh human whole blood from a healthy volunteer, and allowed to rest for 20 minutes in a humidified chamber followed by five minutes rinsing in saline water [18].
Preparation of sample for SEM study: The SEM analysis was done to assess the efficiency of smear layer removal and fibrin clot adhesion. The specimens were fixed with 2.5% glutaraldehyde (pH 7.2) at room temperature for 30 minutes followed by airdrying and dessication with a glass vacuum dessicator. The specimens were mounted in SEM stubs then visualised in Stereoscan- 440 operated at an accelerated voltage of 15-20 KV and sputter coated with a thin layer of a conductive material, gold palladium using a sputter coater (Polaron SC 500 sputter coater).
Analysis of photomicrographs: SEM analysis:
The surface was randomly chosen from each dentin block, and the sample section that best reflected the overall surface topography was chosen and photographed.
The photomicrographs were assessed by two experts from the field of microbiology to determine the degree of smear layer removal using Root Surface Modification Index by Sampaio’s index – 2005 [19] and BEAI- FRM Leite 2005 [20]. The BEAI tested the adherence of the blood component, as well as, the configuration of the fibrin strands.
Root surface modification index [19]:
Score 1: Root surface without smear layer, with dentinal tubules completely opened; no evidence of smear layer in the dentinal tubule gaps.
Score 2: Root surface without smear layer, with dentinal tubules completely opened; evidence of smear layer in the dentinal tubule gaps.
Score 3: Root surface without smear layer, with the dentinal tubules partially opened.
Score 4: Root surface covered with smear layer, with uniform aspect; evidence of dentinal tubule gaps.
Score 5: Root surface covered with smear layer, with uniform aspect; no evidence of dentinal tubule gaps.
Score 6: Root surface covered with smear layer, with irregular aspect and presence of grooves and/or scattered debris.
Blood element adhesion index by FRM Leite in 2005 [20]:
The following scores were used to gauge how closely the fibrin network was linked to the conditioned root surface:
Score 0: Absence of fibrin network linkage to dentin surface
Score 1: Scarce fibrin network linkage to dentin surface
Score 2: Moderate fibrin network linkage to dentin surface
Score 3: Dense fibrin network linkage to dentin surface
The frequency of the number of samples that matched the index scores was tabulated.
Results
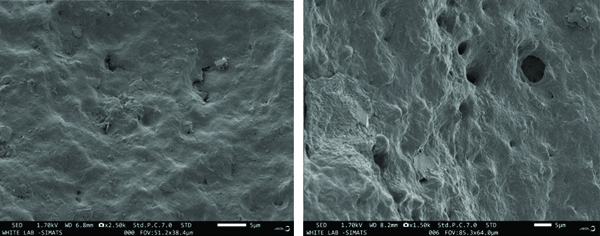
At x1500 magnification, 50% of the ACV group had maximum smear layer removal of RSMI (score-2), and the remaining ACV samples showed RSMI (score-4), indicating root surface covered with smear layer with uniform aspect, evidence of dentinal tubule gaps. In contrast, 50% of the samples in the CA group had evidence of smear layer removal but only partial dentinal tubular opening with RSMI (score-3), and the remaining CA samples showed the presence of smear layer with no evidence of dentinal tubule opening RSMI (score-5) [Table/Fig-5,6,7].
Frequency distribution according to smear layer removal using Sampaio’s index (n=8) [19].
| Root surface modification index- 2005 [19] | Score 1 | Score 2 | Score 3 | Score 4 | Score 5 | Score 6 |
|---|
| Citric Acid (CA) (n=4) | 0 | 0 | 2 (50%) | 0 | 2 (50%) | 0 |
| Apple Cider Vinegar (ACV) - (n=4) | 0 | 2 (50%) | 0 | 2 (50%) | 0 | 0 |
Data presented as N (%)
At x1500 magnification SEM image of sample treated with ACV and CA showing smear layer removal on the root surface with partial dentinal tubules opening.
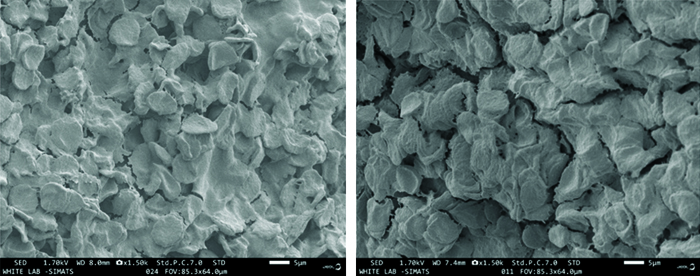
At x1500 magnification, fibrin clot adhesion was similar in both the test and control groups; 25% of samples from both groups had a BEA (score-1), indicating scarce fibrin network linkage to dentin and 50% of samples from both groups had a BEA (score-2), indicating moderate fibrin network formation. Both the ACV and CA groups reported similar levels of satisfaction with the fibrin network. The residual samples exhibited a thick fibrin network with BEA (score-3) [Table/Fig-8,9,10].
Frequency distribution according fibrin clot network using BEAI [20].
| Blood Element Adhesion Index (BEAI) [20] | Score 1 | Score 2 | Score 3 |
|---|
| Citric Acid (CA) (n=4) | 1 (25%) | 2 (50%) | 1 (25%) |
| Apple Cider Vinegar (ACV)- (n=4) | 1 (25%) | 2 (50%) | 1 (25%) |
Data presented as N (%)
At x1500 magnification SEM image showing fibrin clot adhesion on root surface treated with ACV and CA.
Discussion
Hypermineralisation in periodontitis-affected teeth makes the root surface unsuitable for fibroblast attachment and proliferation, which are necessary for the healing of periodontal wounds. When these surfaces are instrumented, a smear layer of subgingival plaque and bacterial endotoxins is inevitably left on them. Mechanical methods alone cannot totally disinfect periodontitis-affected root surfaces. In order to produce an environment that is more conducive to periodontal healing, the procedure of root biomodification employing different agents removes toxins and exposes dentin collagen fibers [4].
CA, one of the commonly used acids to demineralise, was observed to enhance cementogenesis and new attachment by its ability to promote fibrin clot adhesion. But on the contrary, this was declined by a monkey model study by Nyman et al., who did not observe regeneration of periodontal tissues. Few studies have also noted the cytotoxic effect of CA on wound healing, which has an adverse effect on the tissues exposed to high acidity following CA application. Because of its low pH, it has been shown to have adverse healing reactions when it comes into direct contact with periodontal cells [21-26].
So, the present study was conducted to evaluate the smear layer removal and fibrin clot adhesion of ACV in comparison to CA by SEM on periodontally affected teeth. In the SEM analysis, the test group exhibited satisfactory smear layer removal with a Sampaio index score of 2, which seems to be better than the control group. In the fibrin clot adhesion index, the BEA score was similar in both samples, illustrating that the novel ACV has a wound healing effect that is comparable to CA.
In the literature, ACV has been studied for its effect on smear layer removal in endodontics.
A study done by Zandim DL et al., assessed the effects of different types of vinegar on smear layer removal and dentinal tubule opening to investigate the association of vinegar consumption and dental hypersensitivity. It was observed that vinegar from apples and alcohol showed the highest dentinal tubule opening compared to rice and balsamic vinegar. In smear layer removal, 60% of the ACV group showed maximum smear layer removal [27], which is comparable to our study results.
Another study was conducted to test the efficiency of apple vinegar and sodium hypochlorite (NaOCl) with Ethylenediaminetetraacetic Acid (EDTA) as an intracanal irrigant on smear layer removal. The study noted that apple vinegar as an irrigant showed excellent smear layer removal compared to conventional NaOCl. The authors concluded that apple vinegar should be considered as a potential organic alternative to NaOCl [28]. Similarly, in the present study, ACV scored better than CA in smear layer removal.
Yet another study compared the smear layer removal effect of apple vinegar with 17% EDTA. The study results revealed that apple vinegar had a similar effect as EDTA at all root canal levels when used as a final irrigant solution after biomechanical preparation of the root canals [29].
A recent study conducted by Ballal NV et al., studied the root conditioning effects of Maleic Acid (MA), CA, and EDTA on extracted teeth. The SEM analysis noted that MA exhibited better smear layer removal than the other agents. This observation was because MA has a more demineralising effect than CA and EDTA [30]. In present study, ACV, which was primarily composed of acetic acid, also had maleic acid as the second major acid constituent. The results of the present study could also be attributed to the demineralising effect of MA.
For the periodontal tissue to regenerate, a fibrin clot must be formed between the gingival tissue and the periodontally damaged root surface. Blood components that are produced on the root surface during surgery and at wound closure must provide a connection. This connection must stay stable throughout the initial stages of wound healing. Connective tissue, clot adhesion, and root surface must interact for a successful outcome [31]. In the present study, fibrin clot adhesion was also assessed, and the majority showed a moderate amount of clot adhesion in both sample groups. Since this study was done on a smaller scale to determine the feasibility of using ACV as a root conditioner for a full-scale study on periodontal regeneration, a smaller sample was subjected to SEM analysis. This in-vitro analysis helped us understand the chemical and biological effects of ACV compared to conventional CA. Blood clot stability is pivotal for periodontal wound healing as it prevents epithelial migration and paves the way for periodontal cell repopulation. The clot also provides the necessary growth factors to upregulate the molecular signaling pathway. Further, larger-scale research can be undertaken to study more in detail the effects of various concentrations and exposure times. Method of application and its interaction in fibroblast cell line studies.
Since this is the first kind of study to assess ACV fibrin clot adhesion to our knowledge, the present study results for ACV could not be compared. The present study could only be partially related to the available literature. In the study by Ballal NV et al., a cell culture study was done to assess the fibroblast attachment to the conditioned root surface. The authors summarised that the tested root conditioners CA, EDTA, and MA all exhibited cell attachment on the dentinal surface, which could provide better periodontal regeneration [30]. The present study observation of fibrin clot adhesion between ACV and CA is similar to the above study.
A study done by Subramanian S et al., compared the fibrin clot adhesion among the root conditioners like CA, EDTA, and saline. The results showed CA with a mean BEA score of 2.8±0.4 and EDTA 2.2±0.6 [32]. Though the scores were statistically significant, the intergroup comparison was not statistically significant. In the present study, half of the CA samples exhibited moderate fibrin clot adhesion (Score 2), which was not similar to the aforementioned study. This could be due to a smaller sample size.
The present test results were a little varied when compared to a study done by Minocha T and Rahul A on the blood clot adhesion index between CA, EDTA, and CA with EDTA. Within the groups, dense clot adhesion was reported in 60% of CA samples, and 40% of CA samples showed moderate fibrin adhesion, similar to the present study results [33].
ACV has been reported to have several biologic properties; a few to mention are antimicrobial, anti-inflammatory, and anti-oxidant activity. The presence of bioactive components like acetic acid and phenols makes it a potent antibacterial agent by crossing the microbial membrane, decreasing the intracellular pH, and eventually causing leakage of intracellular contents that results in bacterial cell death. The studies have reported their antibacterial effect against an array of organisms like Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus pyogenes, Enterococcus faecalis, Streptococcus pneumoniae, Pseudomonas aeruginosa, Pseudomonas fluorescens, Escherichia coli, Salmonella typhi, Enterobacter aerogenes, Klebsiella pneumoniae, Proteus mirabilis, Proteus vulgaris, and Acinetobacter [34]. In oral infections of endodontic origin, ACV was tested effective and comparable to 3% sodium hypochlorite against Staphylococcus aureus, Enterococcus faecalis, and Candida albicans [29].
In chronic inflammation like periodontitis, oxidative damage resulting in free radical formation initiates and exaggerates inflammation. ACV had exhibited appreciable antioxidant activity due to its presence of phloretin and quercetin. It increases the activity of critical enzymes that defend against oxidative stress, like glutathione peroxidase, catalase, and superoxide dismutase [35]. According to a study done by Asaad N and Laflouf M ACV exhibited an antiplaque effect due to its nature of dissolving dental plaque through its chemo-mechanical properties. And this effect was comparable to manual brushing without toothpaste [36]. The presence of phenols and flavonoids in ACV also aided in the inhibition of inflammation by downregulating prostaglandins and cytokines like TNF and IL-6 [35].
Limitation(s)
The limitations of the present study were that, since it was a pilot study, only a small number of samples were evaluated. And different concentrations of ACV were not tested. With the use of the current findings, large-scale research can be planned, employing various ACV concentrations under different magnifications.
Conclusion(s)
In this in-vitro investigation, it was discovered that both the ACV and CA groups eliminated a significant amount of smear layer; however, ACV resulted in greater dentinal tubular opening than CA. This demonstrates that the ACV was marginally better than the CA. The fibrin clot network adhered moderately in both groups. This fibrin-clot adhesion will allow for uninterrupted periodontal wound healing. The ACV evaluated in the current study showed good outcomes as a root conditioner. It might thus be regarded as an alternative to chemically manufactured root conditioners. However, because this is pilot research, more large-scale investigations are required to extend the findings therapeutically. Additional research and clinical trials are needed to establish ACV’s effectiveness in periodontal treatment.
Data presented as N (%)
Data presented as N (%)