Gastrointestinal Tract (GIT) is a hollow organ from the oral cavity up to the anus. The small intestine and colon make up the majority of the GIT and are sites for a wide variety of pathologies, including congenital anomalies, infections, inflammatory, and neoplastic conditions, which may clinically present as intestinal obstruction or perforation [1,2]. Intestinal obstruction is an impairment or complete arrest of the passage of contents through the intestine [3]. Approximately 80% occur in the small intestine due to its narrow lumen, and the most common site for colon obstruction is the sigmoid colon [4].
The causes of obstruction show demographic variation. Tubercular aetiology is the commonest cause of small intestinal obstruction in developing countries, followed by postoperative adhesions, volvulus, and intussusception in developed countries [5,6]. The commonest causes of LBO are tumours (particularly adenocarcinoma involving the left-side), followed by diverticulitis (usually in the sigmoid), volvulus (in the sigmoid or caecum), or fecal impaction [7]. Less common causes include Hirschsprung disease, inflammatory bowel disease, foreign bodies including gallstones, and extra-abdominal cancers metastasising to the abdomen [8]. In Small Bowel Obstruction (SBO), symptoms occur shortly after onset and present with intermittent and colicky abdominal pain around the umbilicus or epigastrium, which improves with bilious vomiting. Compared to this, LBO develops gradually with mild continuous pain, infrequent, intermittent, and feculent vomiting [9]. The diagnosis of obstruction can be made by the clinical evaluation of initial signs and symptoms and erect abdominal plain X-ray [10,11]. However, these findings are non specific, and histopathology is required for the definitive diagnosis of the aetiology [12]. Histochemical and immunostains are routinely used to evaluate medical liver biopsy specimens. The use of these special stains allows the identification of more clinically important information than is available on hematoxylin and eosin stains alone. These special stains are important for evaluating active and chronic injury and for establishing a specific diagnosis. The skillful use of these stains greatly improves patient care. Information on the use of special stains can be scattered in different sources, making the information hard to access. No systematic morphological study has been done in our country to explore the actual prevalence of these conditions in resected intestines. Thus, the present study was conducted to find out the profiles of various histological lesions of the small intestine. The present study was aimed to investigate the histomorphology of all small intestinal lesions in adults and to determine the pattern of small intestinal lesions with respect to age, sex, anatomical site, and relative frequency.
Materials and Methods
The cross-sectional study, conducted from January 2020 to September 2021, included a total of 77 cases of intestinal obstruction due to mechanical causes received in the Department of Pathology, Government Medical College, Haldwani, Nainital, Uttarakhand, India. These cases were included in the study under IEC No. 49/Pat/2019.
Inclusion criteria: All resected small and large intestinal segments with obstruction due to mechanical causes.
Exclusion criteria: Causes of obstruction other than mechanical, such as drug-induced obstruction, obstruction due to paralytic ileus and hypokalemia, and obstruction due to inefficient relaxation of pelvic floor muscles as seen in conditions like multiple sclerosis and spinal cord injury.
Study Procedure
A detailed gross and microscopic examination was performed, including routine stains and special stains wherever necessary. Demographic details, clinical information, and other investigation details were obtained from the requisition form, the treating surgeon, and the patient’s file. The data were presented in numbers and percentages.
Results
A total of 77 cases of intestinal obstruction due to mechanical causes were included in present study. The highest representation was from the age group 31-40 years (25.9%), followed by 21-30 years (15.6%), and the fewest cases belonged to the age group 81-90 years (1.3%). There was a male preponderance 46 (59.8%) with a male to female ratio of 1.5:1 [Table/Fig-1].
Age-wise distribution of patients.
| Age group (year) | Number | Percentage |
|---|
| 1-10 | 6 | 7.9% |
| 11-20 | 8 | 10.4% |
| 21-30 | 12 | 15.6% |
| 31-40 | 20 | 25.9% |
| 41-50 | 10 | 12.9% |
| 51-60 | 9 | 11.7% |
| 61-70 | 7 | 9.2% |
| 71-80 | 4 | 5.1% |
| 81-90 | 7 | 1.3% |
| Total | 77 | 100% |
The most common presentation was constipation (98.70%), followed by abdominal pain (93.51%) and vomiting (57.1%). Tenderness was the most common sign (71.4%) [Table/Fig-2]. The small intestine was more commonly involved (45.5%) than the large intestine (36.4%), and 2.6% of cases showed extraintestinal involvement. One case was of suppurative appendicitis and another of a retroperitoneal mass adhered to the large bowel wall.
Distribution of signs and symptoms (N=77).
| Signs and symptoms | n (%) |
|---|
| Constipation | 76 (98.7%) |
| Abdominal pain | 72 (93.5%) |
| Tenderness | 55 (71.4%) |
| Vomiting | 44 (57.1%) |
| Guarding and rigidity | 27 (35.1%) |
| Distention | 20 (25.9%) |
| Blood in stools | 15 (19.4%) |
| Fever | 14 (18.1%) |
Among the small intestine, the ileum was the most commonly involved site (53.2%), followed by the jejunum (3.9%) and Meckel’s diverticulum (2.5%). In the large intestine, obstruction in the caecum was the most common (14.2%), followed by the rectum in 7.8% and the rectosigmoid junction in 5.19% of cases.
Perforation was the most common gross finding (32.9%), followed by strictures (27.8%) and adhesions (14.4%) [Table/Fig-3]. Non specific inflammatory pathology was the most common cause of obstruction (23.5%), followed by adenocarcinoma (20.8%). Tubercular pathology was the third most common (11.9%), followed by intussusception (10.4%) and ischaemic bowel disease (6.4%) [Table/Fig-4].
Distribution based on lesional characteristics (N=77).
| Lesional characteristics | n (%) |
|---|
| Small intestine | 35 (45.5%) |
| Large intestine | 28 (36.4%) |
| Both | 12 (15.6%) |
| Extraintestinal | 2 (2.6%) |
| Gross finding |
| Perforation | 25 (32.5%) |
| Stricture | 21 (27.3%) |
| Adhesion | 12 (15.6%) |
| Gangrene | 9 (11.7%) |
| Polyp | 6 (7.7%) |
| Ulcer | 3 (3.8%) |
| Tubercle | 1 (1.4%) |
Distribution on basis of aetiology (N=77).
| Aetiology | n (%) |
|---|
| Non specific inflammatory pathology | 18 (23.5%) |
| Adenocarcinoma | 16 (20.8%) |
| Tubercular pathology | 9 (11.9%) |
| Intussusception | 8 (10.4%) |
| Ischaemic bowel disease | 5 (6.4%) |
| Obstructed hernia | 3 (3.8%) |
| Diverticulitis | 3 (3.8%) |
| Crohn’s disease | 2 (2.6%) |
| Non-Hodgkin’s Lymphoma (NHL) | 2 (2.6%) |
| Tubulovillous adenoma | 2 (2.6%) |
| Squamous Cell Carcinoma (SCC) | 2 (2.6%) |
| Volvulus | 1 (1.3%) |
| Acute suppurative appendicitis | 1 (1.3%) |
| Hamartomatous polyp | 1 (1.3%) |
| Gastrointestinal Stromal Tumour (GIST) | 1 (1.3%) |
| WNET (Carcinoid) | 1 (1.3%) |
| Metastatic deposits of adenocarcinoma | 1 (1.3%) |
| High grade soft-tissue sarcoma | 1 (1.3%) |
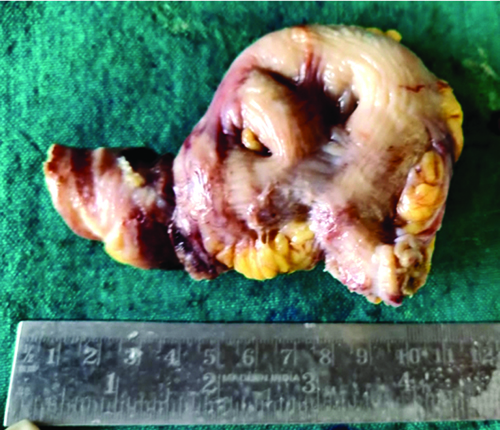
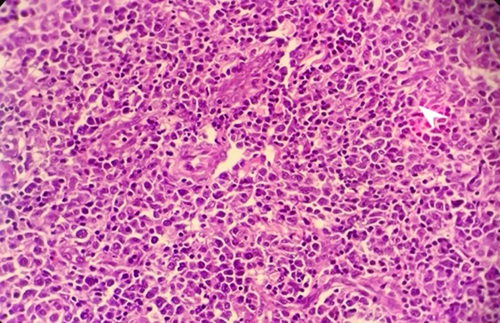
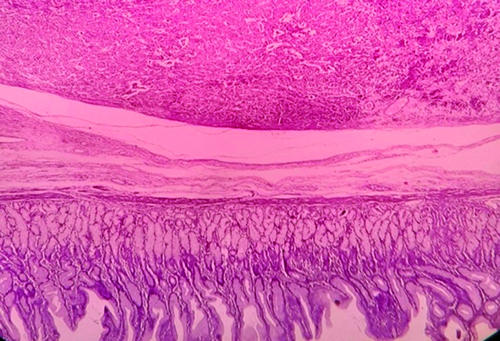
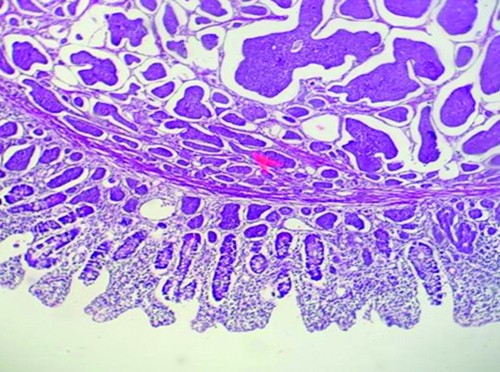
In the first decade of life, intussusception (66.6% of total cases presented in this age group) was the most common aetiology. In the second decade, tubercular aetiology (50.0% of all cases in this age group); Non specific inflammatory pathology (33.3%) followed by tuberculosis (25.0%) in the third decade. In the fourth and sixth decades, adenocarcinoma was the most common pathology. [Table/Fig-5,6,7,8 and 9] shows the gross morphology and histopathological {Haematoxylin and Eosin (H&E)} features of various intestinal obstruction cases reported in present study. The histopathology varies in presentation in all these cases based on the aetiology. For example, Non-Hodgkin’s Lymphoma (NHL) shows poorly differentiated cells, whereas the carcinoid tumour shows benign mucosal glands along with an organoid pattern composed of nests of tumour cells.
Gross specimen of small intestine showing adhesions between intestinal loops.
Gross specimen of large intestine showing ulcer proliferative growth of adenocarcinoma.

Photomicrograph of Non-Hodgkin’s Lymphoma (NHL); Section shows sheets of small to medium size monomorphic atypical lymphoid cells showing high N:C ratio, irregular non cleaved nuclei, coarse clumped chromatin, indistinct nucleoli and moderate amount of eosinophillic cytoplasm (H&E stain, 400 X).
Photomicrograph of epithelioid GIST; Section shows a well circumscribed tumour in the wall (H&E stain, 40 X).
Photomicrograph of small intestine WNET (Carcinoid tumour); Mucosa shows benign mucosal glands. Submucosa shows circumscribed tumour mass with organoid pattern composed of nests of tumour cells (H&E, 40 X).
Discussion
Intestinal obstruction is one of the most serious and frequently encountered emergencies presenting as an acute abdomen, requiring intestinal resection. In this study, out of 77 cases, the majority belonged to the age group of 31-40 years 20 (25.9%), representing the economically viable segment of the population. This indicates that bowel obstruction is a common cause of the loss of productive life. A similar observation was made [13-15]. The small intestine was the most common site of alimentary tract obstruction in present study, probably due to its narrower lumen. This finding may not be surprising, considering that the large bowel is to a great extent a retroperitoneal structure and less likely to be involved in the leading causes of obstructions like adhesions and hernias than small bowels. The maximum number of cases were in the age group of 51-60 years and in the older population, i.e., beyond 50 years [16,17]. This can be explained by differences in geographical regions and demographic variations in the aetiology of intestinal obstruction [18]. The incidence in the older age group is higher in Western countries due to various factors, which include an increased aged population and an increased incidence of malignant aetiology due to the consumption of high animal fat and a lack of fiber in the diet.
The present study included 46 males (59.8%) and 31 females (40.2%), with a male-to-female ratio of 1.5:1. Studies from other regions worldwide have also shown a similar trend, with males outnumbering females, where the ratio was 1.5:1, 1.4:1, and 1.8:1 [19-21]. There is an equal preponderance of intestinal obstruction in both males and females (1:1), but males are twice as affected in the study (2.1:1) [22]. This gender disparity can be attributed to a large number of our patients belonging to hilly areas. Women in rural India are mostly housewives, which limits their exposure to various infections (like tuberculosis and typhoid) in contrast to males. Additionally, socio-cultural barriers in many communities prevent females from seeking medical care at the right time.
Abdominal pain was the most common presentation, followed by constipation [23]. This may be because most other studies include cases of acute intestinal obstruction, which present with severe abdominal pain. However, present study includes acute, subacute, as well as chronic cases. Most of the chronic and subacute cases are due to neoplastic causes and present as constipation.
In present study, the small intestine was more commonly involved (45.5%) in obstruction than the large intestine (36.4%), since, inflammatory and infectious pathology is the most common cause of obstruction, and the most common part involved in both is the ileum. Authors observation was consistent with their study, which reported the large intestine to be the more common site since, the majority of the cases were of neoplastic aetiology [24].
Perforation was the most common gross finding (32.9%) in present study, followed by strictures (27.8%) and adhesions (14.34%). Perforation was the commonest gross finding, with reported polyps followed by perforation. Non specific inflammatory pathology, which is the commonest aetiology in present case, can be due to various causes, including typhoid enteritis. These mainly presented with perforation and adhesions grossly, which was also noted. Additionally, there were many cases of ischaemic bowel disease where perforation was a common finding [25].
The present study showed non specific inflammatory pathology as the most common histopathology in obstruction (23.5%). Most cases of adhesions on histopathology show non specific inflammatory pathology. Adenocarcinoma (20.8%) was the second most common aetiology followed by tuberculosis (11.9%) in present study. Developed countries have also reported carcinoma to be the second most common cause after adhesions with an incidence of approximately 20%. Thus, literature supports authors observation. Adenocarcinoma (23.24%) was the most common etiological factor followed by non specific inflammation (18.59%) and chronic granulomatous pathology (16.27%) [26]. Tubercular pathology was the most common followed by adenocarcinoma and non specific inflammatory pathology. Differences in aetiologies can be explained on the basis of differences in geographical regions and socioeconomic factors. Infectious aetiology is more common in developing countries such as ours, which mainly present as non specific inflammatory pathology. Malignancy is more common in the West due to high consumption of animal fat and lack of fiber in the diet [27].
In present study, there were 50 cases with non neoplastic aetiology (64.9%). Non specific inflammatory pathology was the most common at 36.0%, followed by tubercular pathology at 18.0% and intussusception at 16.0%. Neoplastic aetiology comprised 27 cases (35%), with 11.1% being benign and the rest malignant. Adenocarcinoma was the most common malignant cause at 59.3%. Other malignancies included squamous cell carcinoma of the anal canal (7.4%), NHL (7.4%), GIST (3.7%), WNET (3.7%), metastatic deposits of adenocarcinoma (3.7%), and high-grade soft-tissue sarcoma (3.7%). Only a few studies on intestinal obstruction have described the histopathological findings in their results, classifying causes as neoplastic and non neoplastic without detail. Similar to present findings, a study with N=86 observed non specific inflammatory pathology as the most common benign cause and adenocarcinoma as the most common malignant cause [28]. Adenocarcinoma was found to be the most common cause of intestinal obstruction (27%) among neoplastic and non neoplastic causes, with lymphoma as the second most common neoplastic cause (7%), followed by metastatic deposits of adenocarcinoma (4.3%). In another study with N=34, lymphoma was the most common neoplasm causing obstruction (26.5%), followed by stromal tumours (23.5%), WNETs (20.5%), adenocarcinoma (20.5%), and metastasis (8.8%). Variations in findings are due to the demographic distribution of cancer as well as differences in the number of cases across various age groups [29].
Limitation(s)
The paediatric age group was not included in present study. This group can also present with the same signs and symptoms, and similar lesions can be found. Periampullary lesions studied can arise from the bile duct and pancreatic ducts. Not many studies are available on the study of lesions of the small intestine.
Conclusion(s)
Intestinal obstruction is a life-threatening condition worldwide. The present study highlights the important pathologies in obstruction. The majority of present cases belonged to the economically viable segment of the population, indicating it as a common cause of loss of productive life. Early intervention or preventive measures can control atleast some of the infectious diseases and prevent the development of such emergency situations. Neoplasms are the leading cause of LBO in present study. Early diagnosis and treatment are beneficial for better management and are imperative in providing a better quality of life to the patient.