Giant Haematometrocolpos due to Postvaginoplasty Stenosis
Pabbisetty Sushma1, Jaya Selin Praveena Joseph2, Mohan Shobana Aparna3, Senthil Kumar Aiyappan4
1 Junior Resident, Department of Radiodiagnosis, SRM Medical College Hospital and Research Centre, Kattankulathur, SRMIST, Chengalpattu, Tamil Nadu, India.
2 Junior Resident, Department of Radiodiagnosis, SRM Medical College Hospital and Research Centre, Kattankulathur, SRMIST, Chengalpattu, Tamil Nadu, India.
3 Junior Resident, Department of Radiodiagnosis, SRM Medical College Hospital and Research Centre, Kattankulathur, SRMIST, Chengalpattu, Tamil Nadu, India.
4 Professor and Head, Department of Radiodiagnosis, SRM Medical College Hospital and Research Centre, Kattankulathur, SRMIST, Chengalpattu, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Senthil Kumar Aiyappan, Department of Radiodiagnosis, SRM Medical College Hospital and Research Centre, Kattankulathur, Chengalpattu-603203, Tamil Nadu, India.
E-mail: asenthilkumarpgi@gmail.com
Magnetic resonance imaging, Nulliparous, Vaginal reconstruction
A 24-year-old nulliparous unmarried woman presented to the Gynaecological Department with complaints of abdominal pain for two years that has worsened over the past two days. The pain was dull aching with no aggravating or relieving factors. It was continuous in nature and was associated with a few episodes of vomiting. There was no history of fever or other constitutional symptoms. Vital signs were normal. The patient had primary amenorrhoea and cyclical abdominal pain, for which she was examined and diagnosed with vaginal atresia. Following this, she underwent neovaginoplasty 10 years ago, using the McIndoe vaginoplasty technique. However, the patient failed to undergo periodic vaginal dilatation.
On examination, the abdomen was distended and tense with the presence of a large abdominopelvic mass lesion extending from the pelvis to the epigastrium. On per speculum examination, the urethra was not clearly visualised and the vaginal orifice appeared narrowed. On pervaginal examination, the cervix was not delineated and a hard, tense bulging mass was noted, occupying the vagina. Laboratory investigations revealed a low haemoglobin value of 7 g/dL. The rest of the routine investigations were normal.
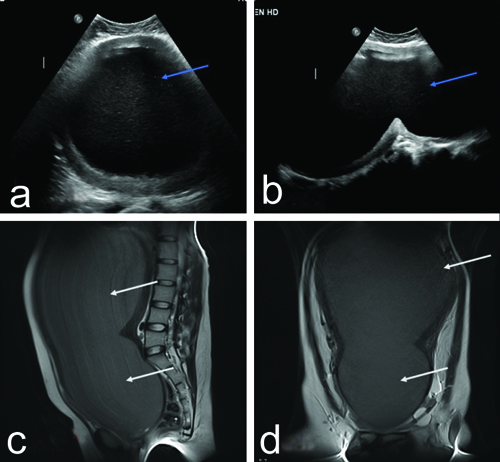
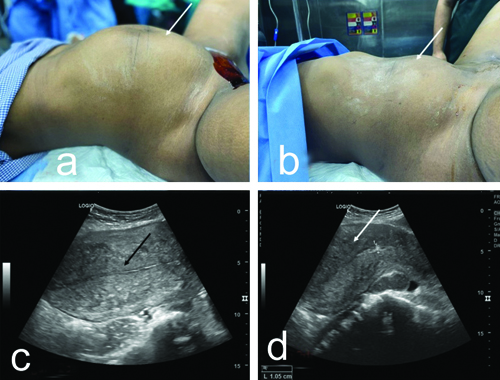
Clinically, a diagnosis of haematometrocolpos was made and the patient underwent ultrasound of the abdomen followed by Magnetic Resonance Imaging (MRI). The ultrasonography revealed a large abdominopelvic cystic mass representing a grossly distended uterine cavity and vagina, which showed echogenic contents [Table/Fig-1a,b]. There was narrowing at the level of the vagina, which was confirmed on MRI, with the endometrial and vaginal cavities showing T2 iso to mildly hyperintense contents suggestive of blood products/proteinaceous contents. The size of the distended uterus and vagina measured approximately 35×18 cm [Table/Fig-1c,d]. Postoperative changes were noted in the vagina with the loss of normal vaginal contour. There was associated mild left hydroureteronephrosis due to obstruction of the left ureter by haematometrocolpos. The patient underwent ultrasound-guided haematometrocolpos drainage with cystoscopy. The patient was placed in a lithotomy position and the surgical site was painted and draped. Under general anaesthesia and aseptic conditions, an incision was made below the urethra and the plane was dissected with ultrasound guidance, following which 4.5 litres of altered tarry chocolate-coloured blood was drained. Postsurgery, a per rectal examination was done to ensure the patency of the rectal mucosa. Foley’s catheter (22G) was inserted through the septum for continuous drainage. The patient received packed red blood cell transfusion preoperatively and postoperatively to improve the haemoglobin level. The abdominal distension and pain significantly reduced after drainage [Table/Fig-2a,b]. Post-drainage ultrasound images showed an empty endometrial cavity and a bulky uterus with heterogeneous echotexture [Table/Fig-2c,d]. Furthermore, the patient was referred to the plastic surgery department for vaginal reconstruction.
a,b) Ultrasound pelvis images showing grossly distended uterus and vagina with echogenic contents suggestive of blood products (blue arrows). c,d) T2 weighted sagittal and coronal MRI images showing grossly distended uterus and vagina extending upto epigastrium showing mildly T2 hyperintense contents (white arrows) suggestive of haematometrocolpos.
a,b) Clinical image showing abdominal distension before drainage with resolution after drainage (white arrows); c,d) Postdrainage ultrasound images showing empty endometrial cavity (black arrow) with heterogenous myometrial echotexture (white arrow).
Haematometrocolpos is the distension of the uterine cavity and vagina with blood due to anatomical mechanical obstruction to the evacuation of menstrual blood [1,2]. The common causes include imperforate hymen, transverse vaginal septum, vaginal atresia, vaginal hypoplasia and vaginal stenosis [2-4]. In the present case, it was due to the failure of neovaginoplasty as the patient did not undergo periodic dilatation. The causes for patient non compliance with dilatation are that they are not comfortable, unpleasant and they often act as a constant reminder of the abnormality, as in the present case. Since the vaginoplasty technique used here was McIndoe and the patient does not engage in sexual intercourse, periodic vaginal dilatation is required for the rest of their life as it uses skin as a graft [1]. Various other vaginoplasty techniques are available now which use peritoneal or intestinal grafts. Periodic vaginal dilatation is not required with these techniques [5]. Ultrasound-guided drainage can be effective in patients with acute pain due to haematometrocolpos, as in the present case [3]. Urinary retention and obstructive uropathy are also complications of haematometrocolpos [6]. In the present case, there was mild left hydronephrosis due to ureteric obstruction by haematometrocolpos, which resolved after drainage. The present case highlights the importance of periodic vaginal dilatation in unmarried females undergoing McIndoe vaginoplasty.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Apr 13, 2024
Manual Googling: Jun 09, 2024
iThenticate Software: Jun 11, 2024
[1]. Abrar S, Mohsin R, Zia-Ul-Islam Vaginal reconstruction in patients with vaginal agenesis: options and outcome: A single-center experiencePak J Med Sci 2023 39(1):219-22. [Google Scholar]
[2]. Saleh R, Katzenbach III G, Espinosa J, Hematometrocolpos disguised as abdominal painJ Emerg Med 2017 53(5):e97-99.Epub 2017 Oct 510.1016/j.jemermed.2017.06.043 [Google Scholar] [CrossRef]
[3]. Long JR, Gomez-Lobo V, Sharma K, Treatment of hematometrocolpos associated with vaginal agenesis using ultrasound-guided active drainageJ Vasc Interv Radiol 2022 33(12):1624-26. [Google Scholar]
[4]. Brito LGO, Suto HS, Hematometrocolpos in a teenagerN Engl J Med 2018 378(8):e12 [Google Scholar]
[5]. Dias MTPM, Bilhar APM, Rios LC, Costa BA, Duete ÚR, Lima Júnior EM, Neovaginoplasty for radiation-induced vaginal stenosis using Nile Tilapia Fish Skin as a biological graftJ Surg Case Rep 2019 2019(11):rjz311 [Google Scholar]
[6]. Kumar Y, Yadav P, Agarwal A, Abdominal swelling and obstructive uropathy due to hematometrocolpos secondary to imperforate hymen: A case reportPan Afr Med J 2022 41:18 [Google Scholar]