Behaviour management is a cornerstone of Paediatric Dentistry, particularly when it comes to alleviating the anxiety that children often feel during dental treatments. One innovative approach that has shown promise is the use of coloured restorations [1]. By allowing children to choose from a palette of colours for their dental fillings or sealants, dentists can transform a routine procedure into a more interactive and enjoyable experience [2]. This choice not only serves as a distraction but also gives children a sense of control over their treatment, which can be incredibly empowering. Studies have indicated that when children are involved in the decision-making process, their cooperation improves, and their anxiety levels decrease significantly [3].
The psychological impact of colour cannot be underestimated in the context of behaviour management. Colours are known to influence mood and perception, and this is particularly true for children, who are often more sensitive to visual stimuli. By incorporating colourful dental materials, dentists can create a more welcoming and less intimidating environment [4]. For instance, a child who might associate white fillings with pain or fear could perceive a blue or pink filling as something fun and exciting [5]. This positive association can make subsequent visits to the dentist less stressful for the child and easier for the dental care provider. Moreover, the preference for certain colours, such as pink or blue, has been observed to be higher among children, suggesting that offering a range of popular colours could be beneficial in managing behaviour during dental procedures [6].
In addition to the emotional benefits, coloured restorations can also have practical advantages. They can make it easier for both the dentist and the child to identify the treated areas, ensuring that oral hygiene is maintained effectively post-treatment [7]. Furthermore, the use of coloured materials can serve as a learning opportunity for the child, allowing the dentist to educate them about dental health in a fun and engaging way [8]. This educational aspect is crucial, as it helps to build the child’s understanding and awareness of dental care, laying the foundation for healthy habits that can last a lifetime [9]. Ultimately, the use of coloured restorations is more than just a novel approach to dental treatment; it is a comprehensive strategy that addresses the psychological, emotional, and educational needs of children undergoing dental care [10].
To date, no study has used the Modified Frankel Behaviour Rating Scale alongside a questionnaire to compare the behaviour of children after receiving coloured compomer and tooth coloured composite material. Therefore, the present study was planned to evaluate the behaviour of children and their acceptance of coloured versus conventional composite materials.
Materials and Methods
The study was a split-mouth, single-blinded, randomised clinical study conducted on 25 patients in the Department of Paediatric and Preventive Dentistry at GDCH, Nagpur, Maharashtra, India, from August 2023 to January 2024. The study commenced after obtaining ethical approval (IEC/04/60) from the Institutional Ethical Committee of GDCH, Nagpur, Maharashtra, India. It was also registered under the Clinical Trials Registry India (CTRI/2023/06/054346). Signed informed consent was obtained from all patients involved in the study.
Inclusion and Exclusion criteria: Children aged between 5 and 10 years, with bilateral mandibular first or second primary molars affected by Class I occlusal caries (according to GV Black classification) and Type 3 caries as classified by the International Caries Detection and Assessment System (ICDAS), were included in present study following a proper examination. Participants with American Soceity of Anaesthesiologists (ASA) physical status ≥III, any systemic illnesses, or highly uncooperative behaviour during dental procedures were not considered for the study, and participants whose primary mandibular molars were indicated for extraction were also excluded.
Sample size calcualtion: The sample size was calculated using the Epi Info online version sample size calculator, based on data obtained from the study conducted by Zighair RK and Jafa ZJ [11]. The minimum sample size needed for Group 1 was 25, and for Group 2, it was also 25. Therefore, the minimum total sample size required was 50. The total sample size was estimated to be 50 teeth, which corresponds to 25 participants.
Study Procedure
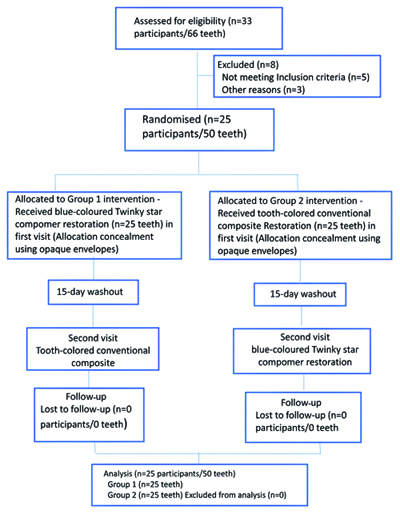
Twenty-five participants with bilateral Class I caries in primary mandibular second molars were selected from the Outpatient Department (OPD) based on the inclusion and exclusion criteria. Consequently, 50 teeth were selected and randomly divided into two groups using computer-based randomisation. Group 1 received a blue coloured Twinky Star compomer, while Group 2 received a tooth coloured conventional composite restorative material. Allocation concealment for selecting the side of the oral cavity was achieved using sequentially numbered opaque sealed envelopes. According to the randomisation, the restoration type allotted to each group was performed during the first visit, and the second visit was scheduled after a 15-day washout period, during which the restoration for the other group was completed.
A total of 33 patients were reviewed for inclusion in the study. After excluding eight patients who did not meet the inclusion criteria, the final sample comprised 25 children, as illustrated in [Table/Fig-1].
Consodilated Standards of Reporting Trails (CONSORT) flowchart.
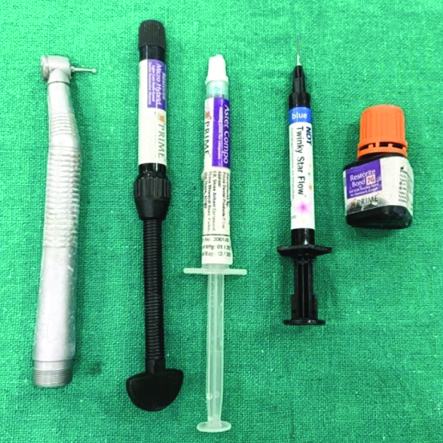
During the restorative procedure, the armamentarium used is shown in [Table/Fig-2a,b]. Isolation was initially achieved using a rubber dam to ensure optimal working conditions. The carious lesion was then removed using a rotary high-speed handpiece, followed by careful cavity preparation. Etching was performed using 37% phosphoric acid for 15 seconds, after which the cavity was thoroughly rinsed and dried. Subsequently, a bonding agent was applied and cured for 15 seconds [Table/Fig-3a,b]. Composite material was then placed incrementally, with each layer being light-cured for 20 seconds. Articulating paper was utilised to verify occlusal irregularities.
Armamentarium. a) Bilateral occlusal caries with 75,85. b) 75 with bule coloured composite, 85 with tooth coloured composite.
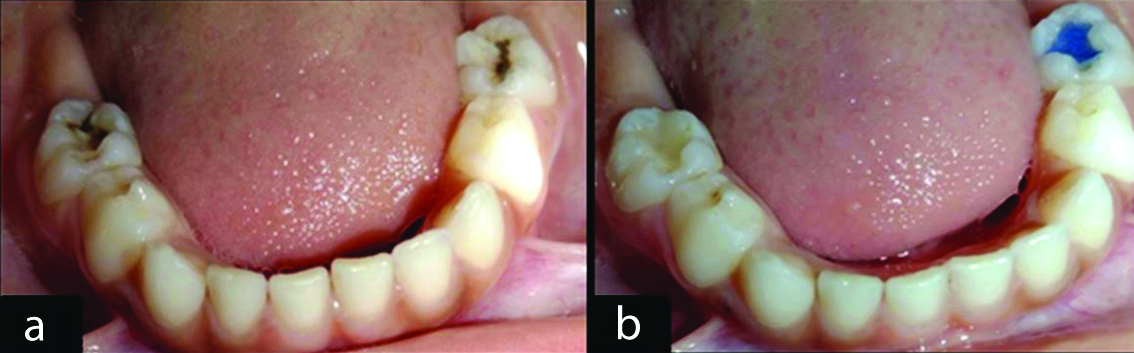
Blue coloured and conventional composite restoration.
The behaviour of the patients was assessed before the start of the dental restoration procedure and after the completion of the restoration placement. The behaviour was evaluated using the Modified Frankel Behaviour Rating Scale [Table/Fig-4] [12].
Modified Frankl behaviour rating scale.
| Rating | Behaviour |
|---|
| Rating 1: Definitely negative (--): | Refusal of treatment, crying forcefully, fearful, or any other overt evidence of extreme negativism. |
| Rating 2: Negative (-): | Reluctant to accept treatment, uncooperative, some evidence of negative attitude but not pronounced, i.e., sullen, withdrawn. |
| Rating 3: Negative positive (-+): | Fluctuation between uncooperativeness and some evidence of unpronounced negative attitude, and cautious acceptance to treatment with reservation shifting throughout the visit. |
| Rating 4: Positive (+) | Acceptance of treatment; at times cautious, willingness to comply with the dentist, at times with reservation but patient follows the dentist’s directions cooperatively. |
| Rating 5: Definitely positive (++): | Good rapport with the dentist, interested in the dental procedures, laughing and enjoying the situation. |
The acceptance of the children and their parents was assessed after the completion of the dental restoration procedure using a questionnaire. The questionnaire was designed by the author to collect the experiences of the children and parents regarding the dental treatment/restoration provided [Table/Fig-5,6]. A total of four questions were asked to the children and another set of four questions was posed to the parents.
Details of questionnaire for children.
| Questions | Category | Responses (%) |
|---|
| How was your experience of dental treatment? | Excellent | 6 (24) |
| Good | 14 (56) |
| Average | 5 (20) |
| Poor | 0 |
| Very poor | 0 |
| Which your favourite colour? | Pink | 2 (8) |
| Blue | 18 (72) |
| Green | 0 |
| White | 5 (20) |
| Did you like the colour of restoration? | Yes | 21 (84) |
| No | 4 (16) |
| Do you think colour of restoration is attractive? | Yes | 21 (84) |
| No | 4 (16) |
Details of questionnaire for parents.
| Questions | Category | Response n (%) |
|---|
| How was your experience for whole treatment procedure of your child? | Excellent | 6 (24) |
| Good | 16 (64) |
| Average | 3 (12) |
| Poor | 0 |
| Very poor | 0 |
| Did you like the colour of the restoration? | Yes | 13 (52) |
| No | 12 (48) |
| How would you describe the acceptability of your child for colourful restoration? | Excellent | 13 (52) |
| Good | 7 (28) |
| Average | 3 (12) |
| Poor | 2 (8) |
| Very poor | 0 |
| How would you describe the attitude towards coloured restoration throughout the procedure? | Excellent | 5 (20) |
| Good | 16 (64) |
| Average | 4 (20) |
| Poor | 0 |
| Very poor | 0 |
The newly developed questionnaire underwent a comprehensive validation process to ensure its reliability and internal consistency. The Content Validation Index (CVI) for various aspects of the questionnaire was calculated, resulting in scores of 0.90 for relevance, 0.88 for simplicity, 0.95 for clarity, and 0.87 for ambiguity. To evaluate test-retest reliability, Cohen’s κ statistics were employed, yielding values of 0.95 for Point X and 0.92 for Point Y. Internal consistency was assessed using Cronbach’s α, which demonstrated strong internal consistency with α values of 0.89 for Point X and 0.91 for Point Y. These validation metrics confirm that the questionnaire is both reliable and consistent across different dimensions.
Statistical Analysis
The children’s behaviour change and acceptability towards the blue coloured Twinky Star compomer and the tooth coloured conventional composite material were presented using frequency distribution. Statistical analysis was performed using SPSS version 16.0. The Wilcoxon signed-rank test was used to compare changes in behaviour within each group, and a comparison of behaviour between the two groups was conducted.
Results
A total of 25 children (14 males and 11 females) participated in the study, with a mean age of 8.47 (±1.59) years. Behaviour was assessed before and after treatment in both groups.
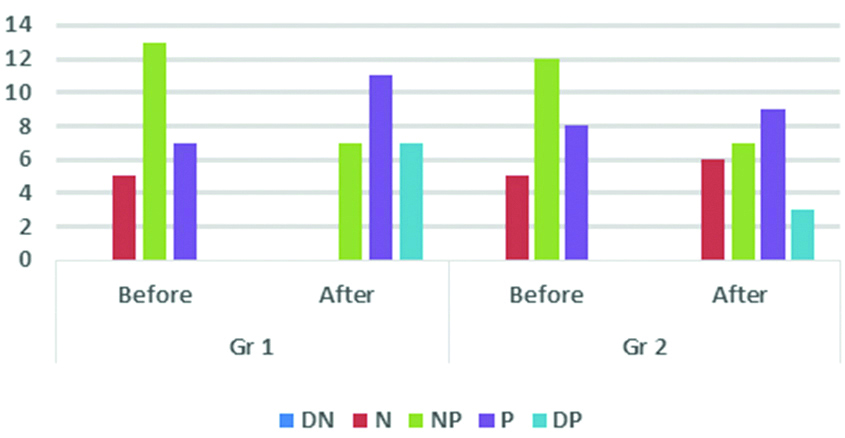
As shown in [Table/Fig-7,8], in Group 1, 13 children (52%) with the blue coloured composite restoration exhibited negative-positive behaviour, while 7 children (28%) showed positive behaviour before treatment. After treatment, this behaviour improved to positive in 11 children (44%) and definitely positive in 7 children (28%). In Group 2, which consisted of children who received conventional composite restorations, behaviour was evaluated before treatment, with 12 children (48%) displaying negative-positive behaviour and 8 children (32%) displaying positive behaviour. After treatment, changes in behaviour were noted: 6 children (24%) exhibited negative behaviour, 9 children (36%) exhibited positive behaviour, and 7 children (28%) continued to display negative-positive behaviour. A statistically significant improvement in behaviour was noted in the blue coloured composite restoration group (p-value <0.001), whereas no statistically significant difference (p-value=0.157) was observed in the conventional tooth coloured composite restoration group.
Comparison of change in behaviour within each group.
| Groups | Interval | DN | N | NP | P | DP | p-value |
|---|
| Group 1 | Before | 0 | 5 (20) | 13 (52) | 7 (28) | 0 | <0.001* |
| After | 0 | 0 | 7 (28) | 11 (44) | 7 (28) |
| Group 2 | Before | 0 | 5 (20) | 12 (48) | 8 (32) | 0 | 0.157 |
| After | 0 | 6 (24) | 7 (28) | 9 (36) | 3 (12) |
(Wilcoxon sign rank test; *indicates significant difference at p≤0.05 in Group-1, there was significant improvement in behaviour of children after treatment whereas change in behaviour in Group-2 was non significant
Comparison of change in behaviour within each groups.
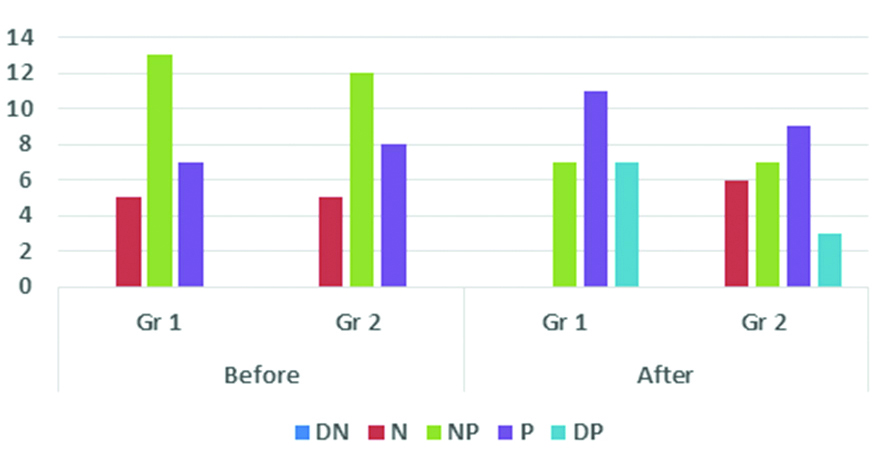
There was no significant difference in behaviour noted before treatment between the groups (p-value=0.832), while a significant difference (p-value=0.024) in behaviour was seen after treatment, with Group 1 showing greater improvement in behaviour, as depicted in [Table/Fig-9,10].
Comparison of behaviour between two groups.
| Interval | Groups | DN | N | NP | P | DP | p-value |
|---|
| Before | Gr 1 | 0 | 5 (20) | 13 (52) | 7 (28) | 0 | 0.832 |
| Gr 2 | 0 | 5 (20) | 12 (48) | 8 (32) | 0 |
| After | Gr 1 | 0 | 0 | 7 (28) | 11 (44) | 7 (28) | 0.024* |
| Gr 2 | 0 | 6 (24) | 7 (28) | 9 (36) | 3 (12) |
(Wilcoxon sign rank test; *indicates significant difference at p≤0.05, there was no difference in behaviour among both the groups before treatment; whereas significant difference was seen in behaviour after the treatment between both the groups with Group-1 showing improvement in behaviour)
Comparison of change in behaviour between two group.
The acceptance of the blue coloured composite and tooth coloured composite material by children and parents was evaluated using questionnaires provided to them. A total of 14 (56%) chidren reported a positive experience during dental treatment, 18 (72%) children liked the blue colour restoration, and 21 (84%) children found the colour of the restoration attractive. 13 (52%) parents liked the colour of the restoration, and 13 (52%) parents noted excellent acceptability of the blue coloured restoration, as shown in [Table/Fig-5,6].
Discussion
The present study evaluated the behaviour of children after the placement of blue coloured and conventional composite materials, as well as its acceptance among children and parents. It showed that both children and parents liked the blue coloured restoration. The results highlight that blue coloured restorations significantly improved children’s behaviour compared to traditional ones. Children in the blue coloured restoration group (Group 1) demonstrated a noticeable shift towards more positive and definitely positive behaviour post-treatment. In contrast, children in the traditional composite group (Group 2) showed mixed results, with some regressing to negative behaviour and fewer exhibiting positive change.
The current research indicates that overall acceptance and adherence rates among both children and parents were notably higher when they were exposed to materials restored with blue coloured composite. This suggests that the incorporation of blue hues has a positive impact on children’s attitudes towards treatment, making them more likely to embrace and co-operate with the procedures involved [13]. One possible explanation for this phenomenon could be the psychological associations linked to the colour [14]. Blue is often associated with feelings of calmness, tranquility, and trustworthiness [15]. Therefore, when children encounter treatment materials enhanced with blue colour restoration, it may evoke a sense of comfort and security, easing any apprehensions they may have about the procedures.
A study by Zighair RK and Jafa ZJ evaluated the effect of multicoloured restorative materials on children’s dental anxiety levels [11]. A highly significant decrease in Abeer Children’s Dental Anxiety Scale (ACDAS) scores after the dental procedure was observed between the control and experimental groups. Similarly, a study by Mascarenhas AN et al., found that children who chose coloured compomers (specifically blue and pink) showed reduced anxiety levels and better behaviour compared to those who opted for traditional composites [16].
A study by Hugar SM et al., evaluated and compared the clinical success of conventional composites and coloured compomer materials in the first permanent molars of children with mixed dentition [17]. Both conventional composites and coloured compomers demonstrated similar retention rates regarding anatomical form, marginal integrity, secondary caries, and marginal discoloration. Similarly, a study by Ertugrul F et al., compared the 12-month clinical performance of conventional (Compoglass F) and coloured (Twinky Star) compomer restorative materials in Class II restorations of primary teeth [10]. No significant differences were found among the groups at all recalls concerning marginal integrity, marginal discoloration, anatomical form, secondary caries, and surface texture. Coloured compomers could also serve as a viable alternative to tooth coloured compomers in the restoration of primary molars.
In the current study, the acceptance of blue coloured restoration among children and parents was evaluated subjectively by distributing a questionnaire to both groups. By collecting subjective responses through these questionnaires, researchers could gain insights into participants’ attitudes, preferences, and experiences regarding the blue coloured restoration. This qualitative approach enabled the researchers to capture the various complexities and perspectives of both children and parents, providing valuable information about the effectiveness of blue coloured composite in enhancing acceptance and adherence to treatment.
There was excellent acceptability of the coloured restoration among 13 (52%) children, while 7 (28%) children showed good acceptability. Among parents, it was noted that 16 (64%) had a good experience during treatment, and 6 (24%) reported an excellent experience. There is evidence suggesting that the incorporation of coloured composite restorations can positively influence children’s attitudes towards dental treatments. A study evaluating parental knowledge and acceptance of various dental treatments found that colourful and visually appealing restorations were generally well-received by both children and their parents. This acceptance was linked to improved cooperation and reduced anxiety during dental procedures [18].
Limitation(s)
The present study has focused solely on one colour for restoration. To expand understanding, authors can further evaluate acceptance by incorporating restorations in different colours.
Conclusion(s)
The blue coloured Twinky Star compomer was associated with a significant improvement in children’s behaviour post-treatment compared to the tooth coloured conventional composite material. High acceptance rates for the coloured composite were observed among both children and parents. Children’s natural affinity for colours often translates into positive behaviour and satisfaction following the placement of these materials, as noted by both parents and children.
(Wilcoxon sign rank test; *indicates significant difference at p≤0.05 in Group-1, there was significant improvement in behaviour of children after treatment whereas change in behaviour in Group-2 was non significant
(Wilcoxon sign rank test; *indicates significant difference at p≤0.05, there was no difference in behaviour among both the groups before treatment; whereas significant difference was seen in behaviour after the treatment between both the groups with Group-1 showing improvement in behaviour)