The introduction of Laryngeal Mask Airways (LMAs), along with constant innovation in their design, has provided airway managers with an alternative to endotracheal intubation. However, the performance of supraglottic airway devices, including their sealing function, can be affected by head and neck movements. A neck position in flexion reduces the anteroposterior diameter of the pharynx by eliminating the longitudinal tension in the pharyngeal muscles anteriorly. In contrast, a neck position in extension increases the anteroposterior diameter of the pharynx by elevating the laryngeal inlet [1-4]. Most of these supraglottic devices aim for non-traumatic placement in the oropharynx to form an adequate seal, which allows for predictable ventilation.
Assessment of this seal pressure, or leak pressure, is a manouver that has commonly been used to confirm the function of the device and for research purposes concerning these LMAs. Anecdotal evidence suggests that the newly introduced LMA Protector provides better oropharyngeal seal pressure when used for controlled ventilation [Table/Fig-1] [5-8]. However, there is a lack of conclusive literature to prove this in different head and neck positions.
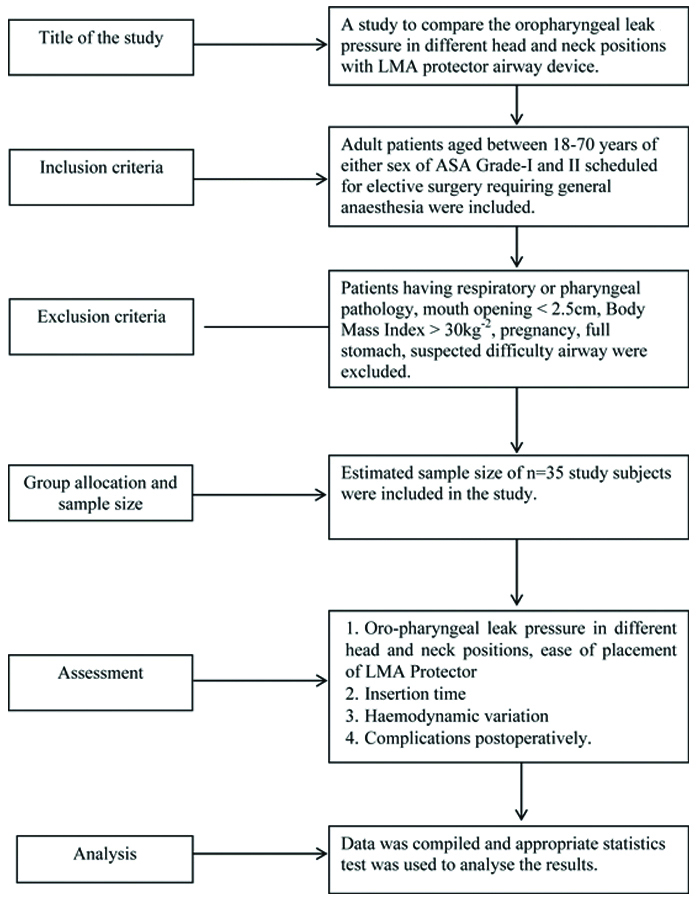
Thus, the authors conducted a study with the primary objective of comparing the difference in OLP with changes in head and neck positions using the LMA Protector airway device. The secondary objectives include studying the ease of insertion of the device, the number of attempts required for insertion, hemodynamic variations, fiber-optic scoring, and any postoperative complications that may occur.
Materials and Methods
The present prospective crossover study was conducted in the Department of Anaesthesiology and Critical Care at Pt. BD Sharma, PGIMS, Rohtak, Haryana, India, from April 2021 to May 2022 after approval was obtained from the Institutional Ethics Committee. The trial was registered on the Clinical Trial Registry-India (no. CTRI/2022/10/046439). Thirty-five patients were enrolled in this study.
Sample size estimation: Our estimated sample size of 35 patients is based on the primary outcome variable, OLP, from a previous study where the mean OLP was found to be 22 cm H2O in the neutral position and 26 cm H2O in the flexed position. The authors defined the standard deviation of OLP at the neutral position as seven and at the flexed position as nine, with reference to the previous study [2]. The authors calculated the sample size with a 95% confidence interval, 80% power, and an alpha level of 0.05. Written informed consent was obtained from each patient.
In all 35 patients, the position of the patient’s head and neck was changed randomly from neutral to flexion, extension, right lateral rotation, and left lateral rotation. The flow diagram is shown in [Table/Fig-2].
Anaesthesia technique: All patients were pre-oxygenated with 100% oxygen for three minutes, and anaesthesia was induced with intravenous Fentanyl (2 μg/kg) and intravenous Propofol (2.5 mg/kg). After confirming adequate mask ventilation, vecuronium (0.1 mg/kg) was administered for neuromuscular blockade. Manual ventilation was performed with 4-6% sevoflurane in oxygen. A deflated and lubricated LMA Protector airway #4 was inserted into the oropharynx. The airway cuff was inflated to achieve an intra-cuff pressure of 60 cm H2O with the head and neck in a neutral position. During the insertion of the supraglottic device (SGD) in both groups, airway manipulations such as jaw thrust and insertion depth adjustment were performed at the discretion of the attending anaesthesiologist. Successful placement of the LMA was confirmed by proper chest expansion, adequate exhaled tidal volume, absence of audible leaks, and an appropriate end-tidal CO2 (EtCO2) level.
After confirming the correct placement of the device, the effect of various head and neck positions on the device was evaluated. The neutral position was maintained with the external ear canal level with the top of the shoulder and the ear-eye line (from the external ear canal to the superior orbital margin) vertical [9]. The patient was then repositioned into the following positions: extension, flexion, rotation to the left, and rotation to the right. Each position change started from the neutral position, and the cuff pressure was maintained at less than 60 cm H2O. Anaesthesia was maintained with 50% nitrous oxide in oxygen with sevoflurane. Mechanical ventilation was performed with an expiratory tidal volume of 10 mL/kg and a respiratory rate of 12 breaths per minute.
Insertion time of LMA protector: This is defined as the time from when the device is picked up until the appearance of the first waveform of the end-tidal CO2. If more than one attempt is made, the total time is the sum of both insertion attempts, excluding the time interval between the attempts.
Number of insertion attempts of LMA protector: A maximum of three attempts will be allowed. If insertion is not achieved within three attempts, it was regarded as a failure, and the patient was excluded from the study.
Ease of insertion of LMA protector: The degree of difficulty associated with inserting the Supraglottic Device (SGD) was assessed based on the manouvers needed for insertion. The categories are: easy (no manouvers required), fair (one type of manouver), and difficult (multiple types of manouvers) [10].
Oropharyngeal Leak Pressure (OLP): This was measured by closing the expiratory valve of the breathing circuit at a fixed gas flow of 3 L/min with ventilatory support turned off. The airway pressure at which the dial on the manometer reaches equilibrium or when a leak sound is heard with a stethoscope over the patient’s neck was recorded in the following head and neck positions: flexion, extension, right lateral rotation, and left lateral position.
Intra-Cuff Pressure (ICP): This was adjusted to 60 cm of H2O using a cuff pressure manometer with the head and neck in a neutral position before each measurement.
Peak Inspiratory Pressure (PIP): Thirty seconds after placing the patient’s head and neck in different positions, PIP was recorded.
Ventilatory score: This was scored from 0 to 3 based on three criteria, with each item scoring 0 or 1 point [11]:
- No air leakage with an airway pressure of 15 cm H2O;
- Bilateral chest expansion;
- Square wave capnography.
Fiberoptic grading: This was assessed according to the Brimacombe and Berry scoring system [12,13]:
- 1: Vocal cords not seen;
- 2: Vocal cords plus anterior epiglottis seen;
- 3: Vocal cords plus posterior epiglottis seen;
- 4: Only vocal cords visible.
Haemodynamic parameters: Heart Rate (HR), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), and Oxygen Saturation (SpO2) were monitored before the placement of the LMA Protector Airway in a neutral position (T1), and during flexion (T2), extension (T3), right lateral rotation (T4), and left lateral rotation (T5). At the end of surgery, anaesthesia was reversed using injection glycopyrrolate (10 μg/kg) and injection neostigmine (50 μg/kg), after which the airway device was removed.
Post-removal observations: After the removal of the LMA protector airway device, any gross blood staining was noted. Patients were asked about complaints of sore throat, dysphagia, and hoarseness of voice during the immediate postoperative period, as well as at half an hour and one hour after the removal of the device.
Statistical Analysis
The collected data were coded and entered into a Microsoft excel spreadsheet. Analysis was conducted using Statistical Package for Social Sciences (SPSS) version 20.0 (IBM SPSS Statistics Inc., Chicago, Illinois, USA) for Windows. Descriptive statistics included the computation of percentages, means, and standard deviations. The unpaired t-test was applied to compare two independent observations for quantitative data. The level of significance was set at p≤0.05. All data were analysed with SPSS version 20.0 and are presented as means with standard deviations or as numbers and percentages.
Results
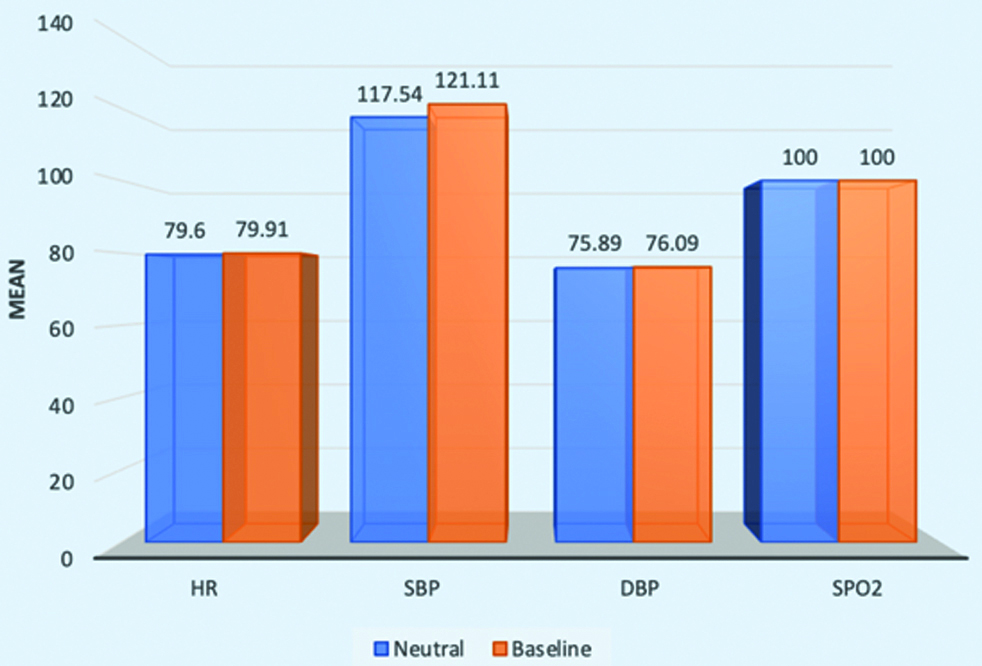
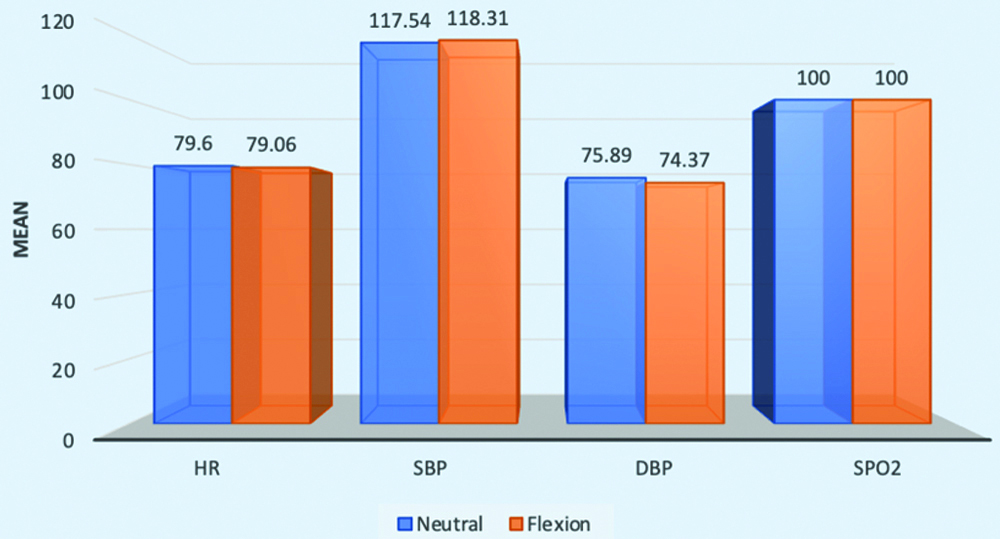
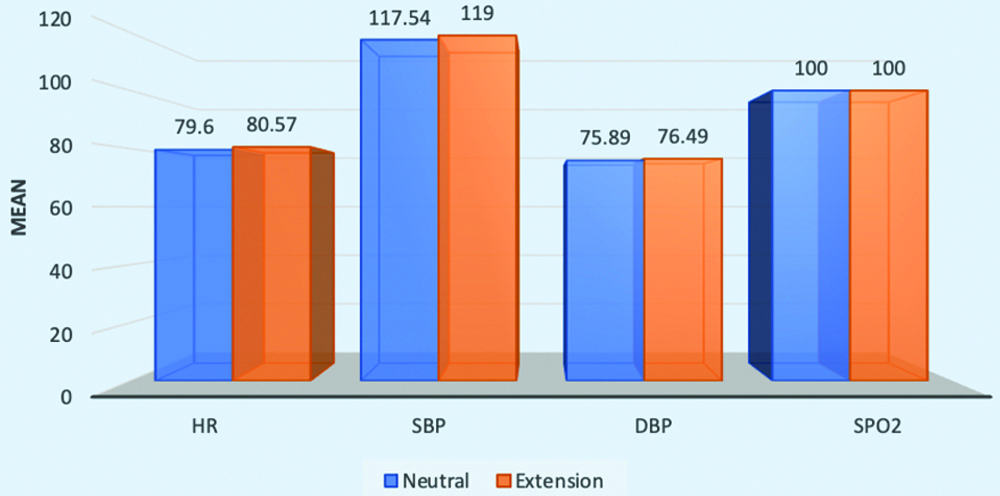
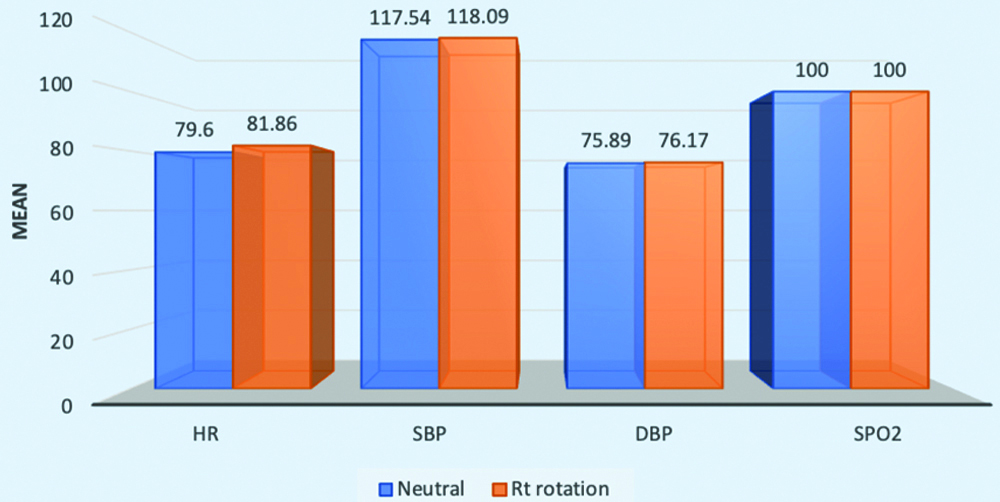
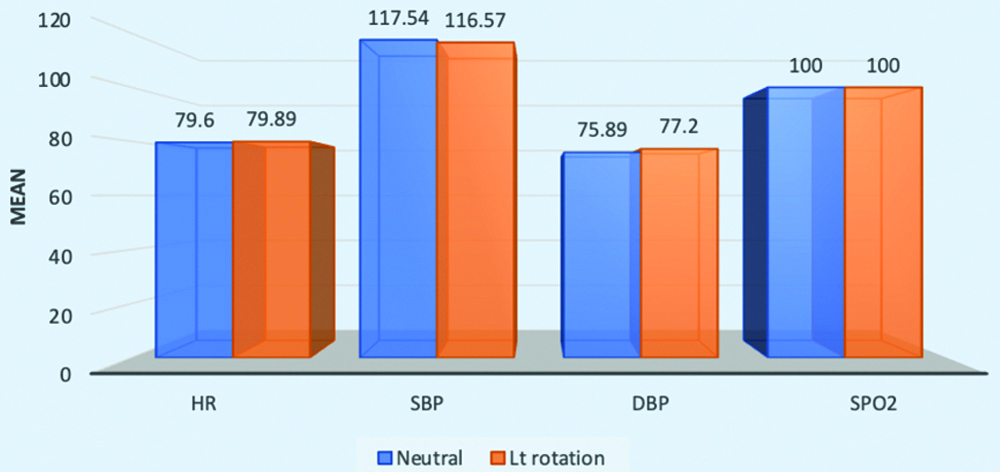
All the patients were comparable in terms of their demographic profiles, as shown in [Table/Fig-3]. Hemodynamically, no significant differences were noted in the various head and neck positions [Table/Fig-4,5,6,7 and 8]. There was no significant difference in the change in SpO2 from the preoperative period to any of the follow-up time points.
Demographic variable distribution of the patients.
| Variable | Mean |
|---|
| Age (years) | 42.26±14.55 |
| Weight (kg) | 63.34±8.23 |
| Gender (M/F) | 17/18 |
| Mallampati grade (I/II) | 16/19 |
Comparison of Heart Rate (HR), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Serum Pressure of Oxygen (SpO2) in baseline to neutral position.
Comparison of HR, SBP, DBP and SpO2 in neutral to flexion position.
Comparison of HR, SBP, DBP and SpO2 in neutral to extension position.
Comparison of HR, SBP, DBP and SpO2 in neutral to right lateral position.
Comparison of HR, SBP, DBP and SpO2 in neutral to left lateral position.
The mean value of OLP in the flexion position was observed to be higher, with a seal pressure of 31.89 cm H2O (SD 5.080 cm H2O) in the neutral position versus 34.49 cm H2O (SD 4.804 cm H2O) in the flexion position. The difference between these two groups was statistically significant (p<0.05). On the other hand, the PIP attained in the neutral position had a mean of 15.38 cm H2O (SD 2.844 cm H2O), while in flexion, the mean was 16.86 cm H2O (SD 2.830 cm H2O), with a p-value of 0.13, which was statistically insignificant. No significant difference in OLP was observed when changing to different head and neck positions, i.e., in extension, right lateral, and left lateral positions [Table/Fig-9].
OLP, PIP, VS in neutral, flexion, extension, right rotation and left rotation position.
| Airway pressures | Neutral | Flexion | Extension | Rt rotation | Lt rotation |
|---|
| OLP (cm H2O) | 31.89±5.080 | 34.49±4.804* | 30.43±5.220 | 32.17±5.448 | 31.94±5.536 |
| PIP (cm H2O) | 15.83±2.844 | 16.86±2.830 | 17.06±3.447 | 16.23±3.163 | 16.43±3.202 |
| VS | 3.00±0.000 | 3.00±0.000 | 3.00±0.000 | 3.00±0.000 | 3.00±0.000 |
OLP: Oropharyngeal leak pressure; PIP: Peak inspiratory pressure; VS: Ventilatory score; *p-value <0.05
The Ventilation Score (VS) for all the different head and neck positions was three, indicating that ventilation is not affected in any position. This suggests that the device can be used in various head and neck positions without issue.
The mean time of insertion was 12.17 seconds, with a standard deviation of 3.04 seconds. The mean total time of insertion was 14.28 seconds, with a standard deviation of 6.21 seconds, a minimum time of 8 seconds, and a maximum time of 32 seconds. The ease of insertion of the Supraglottic Airway Device (SGD) was evaluated based on the manouver used during the insertion of the LMA Protector device: “easy” for no manouver, “fair” for one type of manouvers, and “difficult” for more than one type of manoeuvre [Table/Fig-10].
Ease of insertion wise distribution of the study.
| Frequency(%) |
|---|
| D (Difficult) | 3 (8.58) |
| F(Fair) | 5 (14.28) |
| E (Easy) | 27 (77.14) |
| Total | 35 (100.0) |
Fiberoptic grading: The anatomical position of the device in-situ was assessed using fiber optic evaluation through the airway tube of the device, according to the Brimacombe and Berry scoring system. The authors observed that vocal cords were visible in all patients, meaning that no Grade I observations were made. A total of 24 patients (68.6%) had Grade IV, while 5 patients (14.3%) had Grade II, and 6 patients (17.1%) had Grade III.
Postoperative airway morbidity: After the removal of the LMA Protector airway device, the device was grossly examined for the presence of bile or blood-stained secretions. Trauma to the tongue, teeth, gums, and lips was also assessed. Patients were monitored postoperatively for complaints of sore throat, dysphagia, and hoarseness of voice immediately after removal of the device, as well as half an hour and one hour later [Table/Fig-11].
| Blood on device | Frequency (%) |
|---|
| No | 28 (80.0) |
| Yes | 7 (20.0) |
| Total | 35 (100.0) |
None of the patients experienced immediate postoperative nausea; however, one out of 35 patients reported nausea after 30 minutes in the postoperative period, and another patient experienced nausea after one hour in the postoperative period, yielding a p-value of 0.6, which was statistically insignificant. Both cases resolved without any intervention.
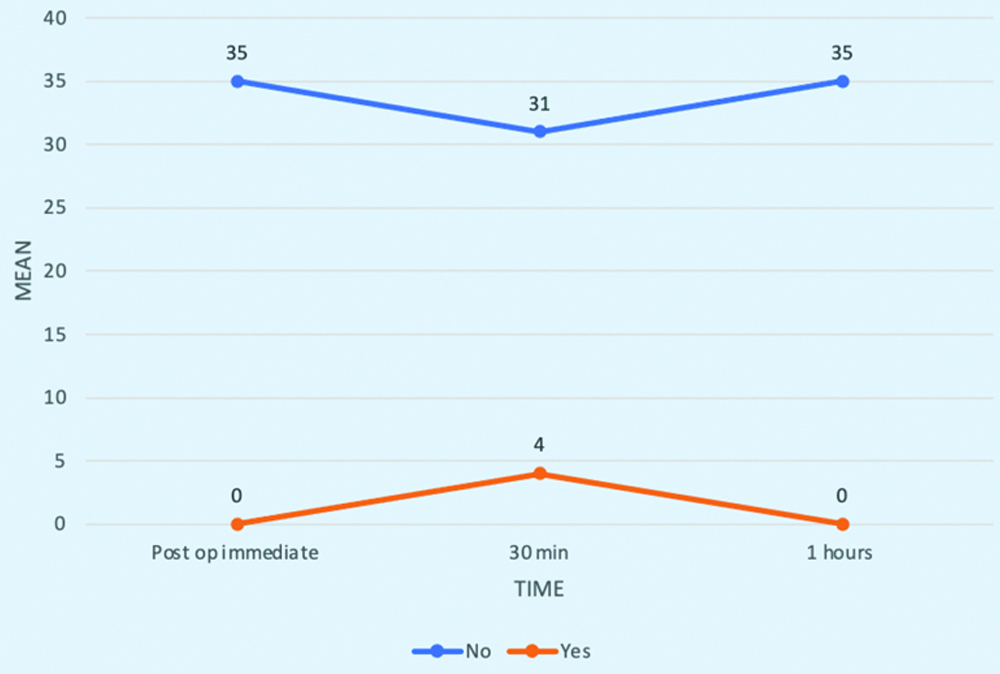
None of the patients had immediate postoperative sore throat; however, four patients out of 35 reported a sore throat after 30 minutes in the postoperative period, resulting in a p-value of 0.01, which is highly significant concerning the LMA Protector device. These patients also experienced self-resolving symptoms without any intervention [Table/Fig-12].
Postoperative sore throat.
Discussion
The present study demonstrates significantly higher OLP in the flexion position compared to the neutral position. The fixation system of the LMA Protector prevents proximal displacement during use, ensuring that the distal end seals around the upper esophageal sphincter. The inflated cuff sits comfortably in the oropharynx, contouring to the patient’s airway anatomy based on the inflated air in the pilot balloon cuff, which makes positive pressure ventilation effective. In line with the present study, Acx E et al., compared the LMA Protector with the LMA Supreme and found that OLP was consistently higher for the LMA Protector compared to the LMA Supreme [14]. Similarly, Taxak S et al., conducted a study on different head and neck positions using the LMA Classic (CLMA) and LMA-Proseal (PLMA), in which the OLP for both PLMA and CLMA was higher in the flexion and left lateral rotation positions (Neutral: 31.52±2.53, 22.76±3.07, p<0.001; Flexion: 36.32±3.11, 26.92±3.12, p<0.001) [15].
In the present study, easy insertion without the use of any manouvers was observed in 77% of the patients. The requirement for manouvers was either due to difficulties in device placement or inadequate ventilation after placing the device. Thus, the present study aligns with other studies that reported easy insertion of the LMA Protector with a fast insertion time [16-18]. These results can likely be attributed to the design of the LMA Protector, which is anatomically shaped, and its fixation system that allows for insertion without the need for digital or introducer tool guidance. This system also prevents proximal displacement during use, ensuring that the distal end seals around the upper esophageal sphincter. However, the present results contrast with the findings of Kerai S et al., who demonstrated longer insertion times and more frequent manouvers to facilitate placement [10]. This discrepancy could be explained by the relative unfamiliarity with the new device at the time their study was conducted.
The authors observed that the vocal cords were visible in all the patients with effective ventilation and oxygenation, which is consistent with the study by Shariffuddin II et al., who evaluated the performance characteristics of the LMA Protector™ in 30 unparalysed, moderately obese patients. Fiberoptic assessment showed a clear view of the vocal cords in 93% of their patients [17]. Similarly, Zaballos M et al., conducted a study evaluating the LMA® Protector in 280 ASA (I-III) patients, where fiberoptic visualisation revealed the vocal cords in 86% of cases. The use of the LMA Protector appears safe and is associated with a high success rate. These attributes suggest considerable potential for its use during anaesthesia [16].
There is a low incidence of airway injury in the present study, which is in concordance with previous studies. Shariffuddin II et al., reported that the incidence of blood staining upon removal of the device was 48%, postoperative sore throat occurred in 27% of cases, dysphagia in 10%, and dysphonia in 20% (all of which were self-limiting and resolved a few hours postoperatively), indicating relatively low postoperative airway morbidity [17]. In another study, Sng BL et al., conducted research on 23 patients and found that six patients experienced a sore throat 24 hours after the procedure, with no reports of dysphagia or hoarseness; the sore throat was self-limiting [18]. This low incidence of complications can be attributed to continuous monitoring and adjustment of intra-cuff pressure according to the needs of ventilation and airway pressure, which helps maintain adequate ventilation and prevent airway trauma.
Limitation(s)
The study could not be blinded, unlike other similar studies involving different devices. Secondly, study was conducted under controlled ventilation, the results cannot be extrapolated to spontaneously breathing patients. Thirdly, the included patients who did not fall into the difficult airway category. The airway of an obese person is a major concern for an anaesthesiologist when providing general anaesthesia.
Conclusion(s)
The LMA protector was easy to insert and required fewer attempts to successfully establish an airway. It is an effective device in terms of superior oropharyngeal seal pressure; the higher the oropharyngeal seal pressure, it better the supraglottic device. There may be clinical circumstances where achieving the desired sealing pressure in different head and neck positions is important. The present study assists airway managers in selecting the most appropriate device for the scenario encountered.
OLP: Oropharyngeal leak pressure; PIP: Peak inspiratory pressure; VS: Ventilatory score; *p-value <0.05