Felty syndrome is a rare and serious complication of Rheumatoid Arthritis (RA), characterised by a triad of RA, splenomegaly (enlarged spleen), and neutropenia (low neutrophil count). RA, a systemic autoimmune inflammatory disease marked by synovitis, commonly occurs in the fifth or sixth decade of life and often affects patients with a history of RA exceeding ten years. It is more prevalent in the Caucasian population due to the underexpression of the Human Leukocyte Antigen (HLA)-DR4 gene in African Americans. Felty syndrome requires the presence of neutropenia, defined as an Absolute Neutrophil Count (ANC) below 2000 cells/mm3, alongside splenomegaly and long-standing RA. Hereby, the authors present a case report of a 44-year-old female with a three-year history of RA, who presented with ascites for nine months and was found to have portal hypertension. Her diagnosis of Felty syndrome was confirmed based on the triad of RA, neutropenia, and splenomegaly, highlighting the importance of early recognition and management to prevent severe complications such as infections and systemic issues like portal hypertension.
Case Report
A 44-year-old female patient presented with the chief complaint of insidious onset of painless progressive abdominal distension over the past nine months, associated with early satiety and two episodes of blood in her vomit, as well as black, tarry stools one day prior. There was no history of yellowish discolouration of the skin, altered sleep cycle, or decreased urine output. She had been a known case of Rheumatoid Arthritis (RA) for three years, diagnosed based on her initial presentation of pain, swelling, and early morning stiffness in both wrists and proximal fingers over a three-year duration.
Examination revealed tenderness of the proximal interphalangeal joints and wrists, along with swelling, indicative of inflammatory polyarthritis involving both small and large joints. Laboratory tests showed raised C-reactive Protein levels (11.1 mg/dL), and she tested positive for anti-cyclic citrullinated peptide and rheumatoid factor.
She was being managed with a maintenance dose of oral steroids (Tab Prednisolone 5 mg once daily), along with Disease-modifying Antirheumatic Drugs (DMARDs) (Tab Methotrexate 15 mg weekly and Tab Hydroxychloroquine 200 mg twice daily). The course of her disease was complicated by interstitial lung disease (non specific interstitial pneumonia) for one year, as evidenced by High Resolution Computed Tomography (HRCT) chest imaging showing diffuse ground-glass opacities following an apical and anteroposterior gradient in both lung fields, with minimal traction bronchiectasis. She also had pulmonary artery hypertension for one year, with HRCT chest findings indicating a Main Pulmonary Artery (MPA) diameter of 33.2 mm and an MPA/aorta ratio greater than 1.0, signifying pulmonary artery hypertension.
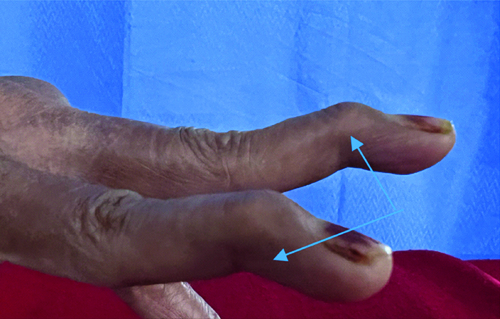
Upon examination, her vital parameters were normal, but she exhibited pallor. A musculoskeletal examination revealed Swan neck deformities [Table/Fig-1,2] in her hands, as well as hallux valgus deformities [Table/Fig-3,4] in her feet.

Swan neck deformity (closer view).
Dorsal view of hallus valgus deformity of left foot.

Ventral view of hallus valgus deformity of left foot.

The respiratory examination revealed velcro crackles in the bilateral infra-scapular and infra-axillary regions. The abdominal examination indicated a distended abdomen, with the spleen palpable up to the umbilicus and shifting dullness present on percussion. A per-rectal examination showed ongoing melena. Investigations revealed pancytopenia with neutropenia [Table/Fig-5].
Investigations of patient.
| Investigations | Results |
|---|
| Haemoglobin | 8.1 g/dL |
| Total leukocyte count/absolute neutrophil count | 2300/900 cumm |
| Platelets | 60000/cumm |
| Sodium/potassium | 140/3.6 meq/dL |
| Total bilirubin | 0.39 mg/dl |
| Total protein/albumin | 6.3/2.4 mg/dL |
| AST/ALT | 34/35 IU/L |
| Urea/creatinine | 12/0.09 mg/dL |
| HBsAg/Anti-HCV/HIV | Negative |
| ICT MP | Negative |
| IgM/IgG EMV | Negative |
| Sputum for AFB | Negative |
| Sputum for CBNAAT | Negative |
| Chest X-ray | Negative |
| PBS | Pancytopenia with normal reticulocytes |
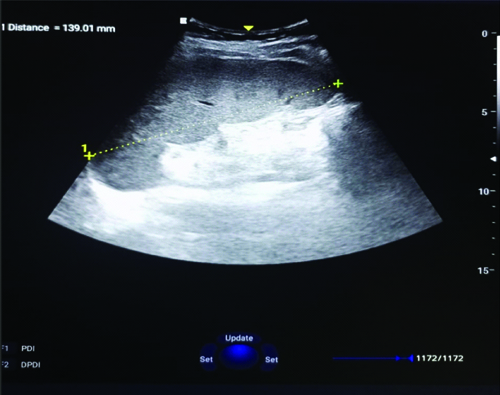
| Ultrasonography abdomen | Massive splenomegaly with recanalised thrombus of the portal vein. Spleen 21 cm, PV 26 cm at the region of eccentric thrombus in the Portal Vein extending from the region of confluence upto bifurcation and extending upto its tight branch |
| Bone marrow aspiration | Erythroid hyperplasia. No evidence of haemato-lymphoid malignancy |
AST: Asparate amino transferase; ALT: Alanine aminotransferase; HCV/HIV: Hepatitis C virus/Human immunodeficiency virus; ICT MP: Immunochromatographic malaria plasmodiun; AFB: Acid fast bacilli; PBS: Peripheral blood smear; EMV: Equine morbillivirus
Ultrasound of the abdomen confirmed splenomegaly (8 cm in size along the longest axis) [Table/Fig-6].
USG Abdomen showing splenomegaly of 13 cm.
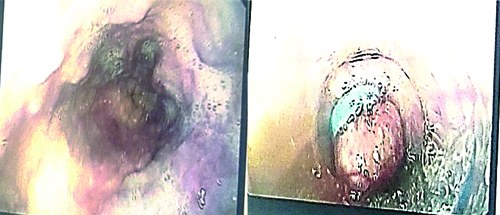
Based on the triad of RA with neutropenia and splenomegaly, she was diagnosed with Felty syndrome and portal hypertension. In light of the ongoing Upper Gastrointestinal (UGI) bleed, she was initially resuscitated, after which she underwent an upper Gastroinstestinal Tract (GI) endoscopy. The endoscopy revealed grade II varices in three locations, characterised by red colour spots/signs [Table/Fig-7]. Endoscopic variceal ligation was performed.
UGI endoscopy showing grade II varices in three locations with red colour spot sign.
She was discharged on the following medications: hydroxychloroquine 200 mg twice daily, carvedilol 3.125 mg twice daily, furosemide/spironolactone (40/12.5 mg once daily), and prednisolone 5 mg once daily. She was followed-up on a monthly basis in the Outpatient Department (OPD). She had no recurrence of UGI bleeding. Her DMARDs, diuretics, and beta-blocker were continued. A repeat UGI endoscopy was planned for six months later.
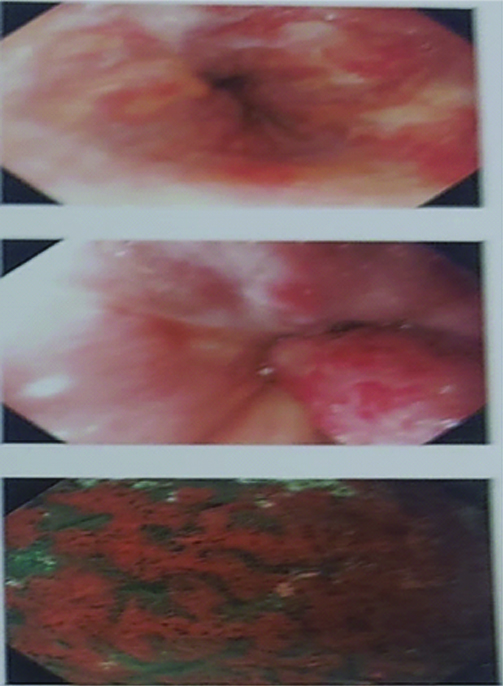
The repeat upper GI endoscopy after six months revealed grade III oesophageal varices [Table/Fig-8], along with severe portal gastropathy and duodenopathy, with no fresh episodes of bleeding.
UGI endoscopy showing grade III oesophageal varices with post Endoscopic Variceal Ligation (EVL) scarring with severe portal gastropathy and duodenopathy.
Discussion
The RA is a systemic autoimmune inflammatory disease characterised by synovitis, pannus formation, and bone destruction [1]. Felty syndrome is a rare complication that occurs in chronic RA and is characterised by extra-articular features such as splenomegaly and neutropenia. It is a diagnosis of exclusion. Felty syndrome commonly occurs in the fifth or sixth decade of life in patients with a history of diagnosed RA for more than 10 years. It is more prevalent in the Caucasian population than in the African American population, likely due to the underexpression of the HLA-DR4 gene in the latter group [2,3].
The triad of features does not have to be present in all patients, but neutropenia, defined as an Absolute Neutrophil Count (ANC) of less than 2000 cells/mm3, is a hallmark feature and must be present for diagnosis. RA primarily affecting the small joints is known to have various extra-articular manifestations, such as interstitial lung disease, pericarditis, episcleritis, vasculitis, and rheumatoid nodules [1]. It is also associated with anaemia, thrombocytopenia, recurrent bacterial infections, and, rarely, portal hypertension, as well as an increased risk of haematological malignancies such as Hodgkin’s and non-Hodgkin’s lymphoma [4-7].
Felty syndrome, characterised by the triad of RA, neutropenia, and splenomegaly, is associated with long-standing RA. Patients with Felty syndrome are usually asymptomatic. Arthritis typically appears first and is usually present for atleast 10 years [8]. Felty syndrome is often associated with severe erosive joint disease and deformity, as noted in present patient. Neutropenia occurs due to decreased production of neutrophils and the presence of autoantibodies to neutrophils, which leads to the aggregation of antigen-antibody complexes in the spleen, causing splenomegaly [9]. Additionally, antibodies to Granulocyte-colony Stimulating Factor (G-CSF), deaminated histones, and Neutrophil Extracellular Traps (NETs) contribute to the peripheral sequestration of neutrophils, worsening neutropenia [10]. Splenomegaly is found in 90% of patients with Felty syndrome [11], and in the absence of neutropenia, a diagnosis of Felty syndrome should not be made [12].
Case series on Felty syndrome in the past have reported the presence of portal hypertension resulting from idiopathic non cirrhotic portal hypertension (which includes nodular regenerative hyperplasia), with episodes leading to variceal bleeding [Table/Fig-9] [12,13]. About 20% of patients with Felty syndrome showed portal hypertension and/or bleeding oesophageal varices [14]. The mechanism of portal hypertension is partly due to increased splenic blood flow and partly due to sinusoidal resistance. The latter occurs due to compression of intrahepatic venous radicles or the presence of microthrombi. In a series of cases, it was reported that an increase in splenic blood flow was attributed as the cause of portal hypertension [15].
Comparison of patients of Felty syndrome presenting with portal hypertension [12,13].
| Author | Patients of felty syndrome | Patients with portal hypertension | Patients with variceal bleed |
|---|
| Goldberg J and Pinals RS [12] | 19 | 5 | 2 |
| Thorne C et al., [13] | 18 | 6 | 3 |
The treatment of neutropenia associated with Felty syndrome includes DMARDs (both non biologic and biologic), which are presumed to reverse the underlying abnormalities in the immune and reticuloendothelial systems. Other therapies include the use of G-CSF [16]. Splenectomy is primarily reserved for patients with neutropenia and recurrent infections who are refractory to medical therapy. The use of glucocorticoids is generally minimised to reduce the risk of infection. Low-dose weekly oral methotrexate therapy often results in improvement of both articular disease and neutropenia, typically within 1 to 2 months. Leflunomide can be used as an alternative for patients unable to take methotrexate. In patients who do not adequately respond to methotrexate, rituximab is considered instead of another non-biological DMARD or a Tumour Necrosis inhibitor. For patients with inadequate response to both methotrexate and rituximab, and who are on a prednisolone dose greater than 15 mg, abatacept may be considered. Glucocorticoids are generally avoided in the presence of active infection, although they may be useful for short-term bridging therapy.
Glucocorticoids can raise the neutrophil count through immunosuppressive action and by altering neutrophil kinetics: they stimulate the release of mature neutrophils from the bone marrow, mobilise neutrophils from the marginal pool into circulation, and impair the migration of neutrophils into tissues [16-18]. Prednisolone doses of 30 mg daily or higher often normalise the neutrophil count [19,20]. The dose is gradually reduced to a maintenance level of less than 10 mg. Our patient has been started on DMARDs and has shown resolution of neutropenia during her follow-up visit after four weeks. In patients with recurring or severe infections and persistent neutropenia despite DMARD therapy, with an ANC of less than 1000 cells/microL, G-CSF is considered for further management.
Splenectomy is indicated in patients with non healing ulcers or recurrent infections (e.g., pneumonia or sepsis) despite medical therapies [19,21]. Previous case reports have shown that splenectomy reduces portal vein flow and can be effectively used to treat oesophageal and gastric varices in patients with Felty syndrome [21-24]. However, the number of cases is limited, and no long-term follow-up data are available. Beta blockers and variceal band ligation are used as primary prophylaxis. In actively bleeding patients, management includes resuscitation with intravenous fluids and component support, along with the use of terlipressin or octreotide, followed by variceal band ligation. For present patient, we chose endoscopic therapy for the management of the varices. A six-month follow-up showed control of the varices, with no re-bleeding.
Conclusion(s)
Felty syndrome is a rare manifestation of RA characterised by neutropenia, splenomegaly, and symptoms of RA. It can be associated with portal hypertension without evidence of cirrhosis, with the liver exhibiting nodular regenerative hyperplasia. There is no definitive therapy or management plan for Felty syndrome. The present case details the presentation and clinical course of a female patient with a relatively recent diagnosis of RA who developed variceal bleeding in the context of neutropenia, which was managed with endoscopic variceal ligation.
AST: Asparate amino transferase; ALT: Alanine aminotransferase; HCV/HIV: Hepatitis C virus/Human immunodeficiency virus; ICT MP: Immunochromatographic malaria plasmodiun; AFB: Acid fast bacilli; PBS: Peripheral blood smear; EMV: Equine morbillivirus
[1]. Xiao RZ, Xiong MJ, Long ZJ, Fan RF, Lin DJ, Diagnosis of Felty’s syndrome, distinguished from hematological neoplasm: A case reportOncol Lett 2014 7(3):713-16.10.3892/ol.2013.1779 [Google Scholar] [CrossRef]
[2]. Lewis RB, Felty’s syndrome in blacksArthritis Rheum 1980 23(3):377-78. [Google Scholar]
[3]. Termini TE, Biundo JJ, Ziff M, The rarity of Felty’s syndrome in blacksArthritis Rheum 1979 22(9):999-1005. [Google Scholar]
[4]. Owlia MB, Newman K, Akhtari M, Felty’s syndrome, insights and updatesOpen Rheumatol J 2014 8:129-36. [Google Scholar]
[5]. Patel R, Akhondi H, Felty syndromeIn: StatPearls 2020 Treasure Island (FL)StatPearls Publishing [Google Scholar]
[6]. Thorne C, Urowitz MB, Wanless I, Roberts E, Blendis LM, Liver disease in Felty’s syndromeAm J Med 1982 73(1):35-40. [Google Scholar]
[7]. Chavalitdhamrong D, Molovic-Kokovic A, Iliev A, Felty’s syndrome as an initial presentation of rheumatoid arthritis: A case reportCases J 2009 2:206 [Google Scholar]
[8]. Liu X, Loughran TP Jr, The spectrum of large granular lymphocyte leukemia and Felty’s syndromeCurr Opin Hematol 2011 18(4):254-59. [Google Scholar]
[9]. Andreis M, Hurd ER, Lospalluto J, Ziff M, Comparison of the presence of immune complexes in Felty’S syndrome and rheumatoid arthritisArthritis Rheum 1978 21(3):310-15. [Google Scholar]
[10]. Hellmich B, Csernok E, Schatz H, Gross WL, Schnabel A, Autoantibodies against granulocyte colony-stimulating factor in Felty’s syndrome and neutropenic systemic lupus erythematosusArthritis Rheum 2002 46(9):2384-91. [Google Scholar]
[11]. Laszlo J, Jones R, Silberman HR, Banks PM, Splenectomy for Felty’s syndrome. Clinicopathological study of 27 patientsArch Intern Med 1978 138(4):597-602. [Google Scholar]
[12]. Goldberg J, Pinals RS, Felty syndromeSemin Arthritis Rheum 1980 10(1):52-65. [Google Scholar]
[13]. Campion G, Maddison PJ, Goulding N, James I, Ahern MJ, Watt I, The Felty syndrome: A case-matched study of clinical manifestations and outcome, serologic features, and immunogenetic associationsMedicine (Baltimore) 1990 69(2):69-80. [Google Scholar]
[14]. Rosenstein ED, Kramer N, Felty’s and pseudo-Felty’s syndromesSemin Arthritis Rheum 1991 21(3):129-42. [Google Scholar]
[15]. DeCoux RE Jr, Achord JL, Portal hypertension in Felty’s syndromeAm J Gastroenterol 1980 73(4):315-18.7416125 [Google Scholar] [PubMed]
[16]. Patel R, Killeen RB, Akhondi H, Felty Syndrome. 2024 Jan 11In: StatPearls [Internet] 2024 Jan Treasure Island (FL)StatPearls Publishing31536299 [Google Scholar] [PubMed]
[17]. Bishop CR, Athens JW, Boggs DR, Warner HR, Cartwright GE, Wintrobe MM, Leukokinetic studies. 13. A non-steady-state kinetic evaluation of the mechanism of cortisone-induced granulocytosisJ Clin Invest 1968 47(2):249-60. [Google Scholar]
[18]. Shoenfeld Y, Gurewich Y, Gallant LA, Pinkhas J, Prednisone-induced leukocytosis. Influence of dosage, method and duration of administration on the degree of leukocytosisAm J Med 1981 71(5):773-78. [Google Scholar]
[19]. Smith MD, Ahern MJ, Brooks PM, Roberts-Thomson PJ, The clinical and immunological effects of pulse methylprednisolone therapy in rheumatoid arthritis. III. Effects on immune and inflammatory indices in synovial fluidJ Rheumatol 1988 15(2):238-41. [Google Scholar]
[20]. Patel R, Killeen RB, Akhondi H, Felty Syndrome. 2024 Jan 11In: StatPearls [Internet] 2024 Jan Treasure Island (FL)StatPearls Publishing31536299 [Google Scholar] [PubMed]
[21]. Kaprove RE, Felty’s syndrome: Case report and rationale for disease-suppressant immunosuppressive therapyJ Rheumatol 1981 8(5):791-96. [Google Scholar]
[22]. Coon WW, Felty’s syndrome: When is splenectomy indicated?Am J Surg 1985 149(2):272-75. [Google Scholar]
[23]. Yang S, Quan M, Li Y, Pan CQ, Xing H, Porto-sinusoidal vascular disease as the cause of portal hypertension in Felty’s Syndrome: A case report and literature reviewBiomed Res Int 2020 2020:2618260 [Google Scholar]
[24]. Stock H, Kadry Z, Smith JP, Surgical management of portal hypertension in Felty’s syndrome: A case report and literature reviewJ Hepatol 2009 50(4):831-35. [Google Scholar]