Cold Urticaria: An Under-recognised Cause of Perioperative Anaphylaxis
Monika1, Himani2, Monica Chhikara3, Akshay Jaswal4, Vivek Singh Kataria5
1 Senior Resident, Department of Anaesthesia and Critical Care, PGIMS, Rohtak, Haryana, India.
2 Senior Resident, Department of Anaesthesia and Critical Care, PGIMS, Rohtak, Haryana, India.
3 Associate Professor, Department of Anaesthesia and Critical Care, PGIMS, Rohtak, Haryana, India.
4 Junior Resident, Department of Anaesthesia and Critical Care, PGIMS, Rohtak, Haryana, India.
5 Junior Resident, Department of Anaesthesia and Critical Care, PGIMS, Rohtak, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Monika, Senior Resident, Department of Anaesthesia and Critical Care, PGIMS, Rohtak-124001, Haryana, India.
E-mail: mk.yadu29@gmail.com
Anaphylaxis is a rare but severe, potentially life threatening allergic reaction which commonly presents with cutaneous to multi-system involvement. The overall incidence rate of anaphylaxis during general anaesthesia varies greatly, ranging from 1:20,000 to 1:38. Cold urticaria, subset of chronic urticaria, is characterised with the presence of localised wheals to systemic and anaphylactic reactions. Physical urticaria can be due to physical stimuli such as friction, pressure, sun exposure and cold. Cold urticaria mainly comprises of physical urticaria rather which ranges from 3-33.8% with a higher incidence in cold climate. A case of physical cold urticaria was reported during perioperative period in a 40-year-old male who was posted in urology OT for a planned Ureteroscopy (URS). On pre-anaesthetic evaluation, patient’s medical, surgical and personal history found to be inconclusive. Patient was fit for surgery under ASA grade 1 and advised to be kept nil per orally for six hours for solid food and two hours for clear fluid. At the conclusion of surgery, patient developed shivering and was managed with warm blankets and radiant heater. After some time, patient develop wheals over chest, abdomen and lower back. Patient was managed with warm fluids, warming the patient, maintaining ambient OT temperature and drugs like injection pheniramine, epinephrine and dexamethasone to prevent catastrophic reaction. Through evaluation during preoperative period plays a key role in anticipation of these kind of untoward events. This case report describes the occurrence and management of this rare condition.
Allergic reactions, Localised wheals, Temperature regulation
Case Report
A 40-year-old male posted in urology OT for URS under a subarachnoid block with 2 mL of 0.5% bupivacaine heavy. On pre-anaesthetic evaluation, history found to be inconclusive. On physical examination, patient was weighing around 75 kg and height of 160 cm. General and systemic examinations were found to be normal. Patient was fit for surgery under ASA 1 grade after taking appropriate informed and written consent.
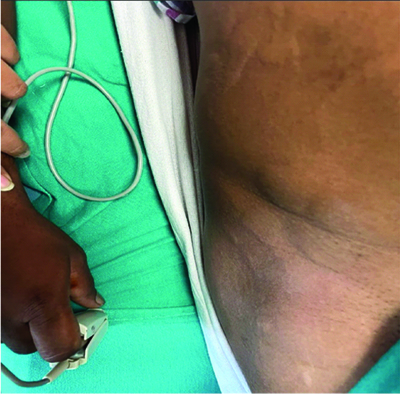
Patient was shifted to OT for the planned procedure after WHO checklist. OT theatre was prepared as per the need. Standard ASA monitors were attached and his vitals were recorded. A pulse of 80 bpm, blood pressure of 110/68 mmHg and SpO2 of 99% on room air were noted. All standard monitoring was carried out during the procedure. At the conclusion of surgery, patient developed shivering and was managed with warm blankets and radiant heater. After some time, patient develop wheals over chest, abdomen and lower back as showed in [Table/Fig-1,2] which was not associated with itching. Cause of hypothermia in patient undergoing urological procedure can be multiple including cold OT temperature, regional anaesthesia and cold irrigating fluid. Patient was managed with injection pheniramine (25 mg) and dexamethasone (6 mg). Fall in blood pressure was also noticed up to 80/50 mmHg, for which 0.1 mg of epinephrine (1:1000, 1 mg) was given subcutaneously and warm fluids was rushed intravenously. Urticaria resolved and blood pressure returns to normal range afterwards (BP: 112/70 mmHg). As per the Ring and Messmer grading system, patient had grade 2 cold urticaria as showen in [Table/Fig-3]. Other causes of anaphylaxis like medications (Neuromuscular Blocking Agents (NMBAs), antibiotics, antiseptics), gelatin and latex, were ruled out. Antibiotic sensitivity test which was done preoperatively was found to be negative for sensitivity. As we secured a wide bore cannula (18 G) over right dorsum of hand while wearing latex gloves, we checked the local site for any allergic reactions which was found to be inconclusive. On enquiring about history related to cold urticaria, he elaborated that whenever exposure to cold water or wind, he developed this condition which always resolved with injection epinephrine taken at local hospital.
Image showing wheals on lower abdomen and chest.

Image showing wheals on lower abdomen and back.
Ring and Messmer grading system [4].
| Grade | |
|---|
| Grade 1 (Mild) | Generalised cutaneous signs |
| Grade 2 (Moderate) | Moderate multi-system involvement with cutaneous sign, hypotension, tachycardia and bronchial hyperreactivity |
| Grade 3 (Life-threatening) | Severe multisystem involvement (circulatory collapse, tachycardia or bradycardia, cardiac arrhythmias, bronchospasm) |
| Grade 4 (Arrest) | Circulatory or respiratory arrest |
| Grade 5 (Death) | Death |
Discussion
Anaphylaxis is a rare but severe, potentially life threatening allergic reaction which most commonly presents with involvement of various system, such as cutaneous, respiratory, cardiovascular, central nervous system and gastrointestinal system as described in [Table/Fig-4] [1]. The overall incidence rate of anaphylaxis during general anaesthesia varies greatly, ranging from 1:20,000 to 1:381 and most common causes are the use of NMBAs, antibiotics, antiseptics, latex, gelatin and others. Cold urticaria is characterised with the presence of localised wheals to systemic and anaphylactic reactions. Cold urticaria is a subset of chronic urticaria. Chronic urticaria is mainly classified into physical urticaria and idiopathic. Physical urticaria can be due to physical stimuli such as friction, pressure, sun exposure and cold. Cold urticaria mainly comprises of physical urticaria rather which ranges from 3-33.8% with a higher incidence in cold climate [1,2].
Clinical presentation of cold urticaria.
| System | Symptoms |
|---|
| Constitutional | Fever, fatigue |
| Skin and mucous membrane | Itchy wheals with or without angioedema affecting lips, tongue, pharynx |
| Respiratory | Dyspnea, hoarseness, laryngeal angioedema, nasal congestion |
| Gastrointestinal | Nausea, abdominal pain, diarrhea |
| Cardiovascular | Tachycardia, hypotension, shock |
| Reproductive | Uterine contractions |
| CNS | Headache, disorientation, fainting, vertigo |
Cold urticaria, a type I hypersensitivity reactions, consists of an allergic immune response with symptoms ranging from pruritic wheals to life-threatening angioedema, bronchospasm or anaphylactic shock [3]. Although it has an unclear mechanism, a cold stimulus can lead to degranulation of mast cell or basophil, followed by the release of histamine and inflammatory mediator. The incidence of cold urticaria is 0.05%, young adults most commonly affected with male to female ratio 1:2 [3]. It is hard to diagnose cold urticaria in perioperative period as the other differential like drugs used for sedation, anaesthesia, antibiotics, antiseptics, NMBAs, latex have to be ruled out. Moreover, patient is covered with sterile drapes and patient does not always complain of itching due to sympathetic blockade. Agbenyefia P et al., reported a case of a 45-year-old female undergoing a laproscopic Nissen fundoplication having a history of cold urticaria. She had a positive history for cold urticaria, naproxen, guaifenesin and menthol. She was taking medications including escitalopram, pramipexole, cetirizine, and ranitidine. Standard anaesthesia technique was used and temperature monitoring was done for this patient with the help of an oropharyngeal probe and a bladder probe. Just before surgical incision, patient had episode of hypotension (69/30 mm Hg) which was managed with epinephrine (1 mg). The whole procedure went uneventful and patient was shifted to recovery covered in warm blankets [2].
Cold urticaria, an unusual condition, is rare and difficult to recognise. Its incidence is relatively low; it can pose an underestimated challenge for anaesthesiologists. The possible causes of cold urticaria during perioperative period includes the infusion cannula, contact hypersensitivity to the cannula, reaction to the intravenous fluid or possible contamination, arterial injection, drug or trauma induced local tissue reaction, cold stimulus and the irrigating solution used during surgery. The main stay of treatment for perioperative anaphylaxis includes fluid resuscitation and epinephrine (starts from 20 μg and escalation accordingly). Risk of cold urticaria in patients undergoing anaesthesia is more than general population unless strict perioperative normothermia is maintained. As redistribution of core body temperature occurs peripherally within first 30 minutes to an hour following induction of anaesthesia as a result of sympathetic blockade and vasodilation. Normothermia can be achieved with air warming blankets, radiant warmer, convection warmer, warmed intravenous fluids with an in-line fluid warmer and adjustment to ambient OT temperature (70 F) [4].
Perioperative recommendations for the management of cold urticaria patients are ambient temperature OR, monitoring the patient’s body temperature and vital parameters, use of premedication (glucocorticoids, antihistamines), pre-warmed solutions for parenteral use, warming of the patients during surgery(blankets, heaters), avoid using alcohol-containing skin preparation solutions [5,6]. In the present case, cold urticaria mainly precipitated due to cold stimuli and presented with wheals and drop in blood pressure without any symptoms of itching. It was managed successfully by warming the patient actively and injection pheniramine, dexamethasone and epinephrine (subcutaneously) were given. Hence, careful planning for seamless perioperative normothermia can helps us to prevent these catastrophic events. Awareness about the aetiology, diagnosis, prevention and prompt treatment of perioperative anaphylaxis help the clinician to prevent this life-threatening event and reduce the morbidity and mortality.
Conclusion(s)
Cold urticaria is a rare potentially life threatening condition. For its prompt recognition and management, adequate knowledge about the differential diagnosis peri-operatively is essential. It is recommended for the anaesthesiologist to be vigilant about such conditions. Careful monitoring and thorough evaluation during preoperative period is the key to prevent these kind of untoward events.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 07, 2024
Manual Googling: Jul 30, 2024
iThenticate Software: Aug 03, 2024 (16%)
[1]. Zou Y, Shao LJZ, Xue FS, Perioperative anaphylaxis: A potential hazard to the safety of surgical patientsChin Med J (Engl) 2020 133(5):609-12. [Google Scholar]
[2]. Agbenyefia P, Shilliam LA, Stoicea N, Roth A, Moran KR, Perioperative management of a patient with cold urticariaFront Med (Lausanne) 2017 4:222 [Google Scholar]
[3]. Maltseva N, Borzova E, Fomina D, Bizjak M, Tehorst-Molawi D, Kosnika M, Cold urticaria - What we know and what we do not knowAllergy 2021 76(4):1077-94.10.1111/all.14674 [Google Scholar] [CrossRef]
[4]. Diaz M, Becker DE, Thermoregulation: Physiological and clinical considerations during sedation and general anesthesiaAnaesth Prog 2010 57(1):25-33. [Google Scholar]
[5]. Garvey LH, Dewachter P, Hepner DL, Mertes PM, Voltolini S, Clarke R, Management of suspected immediate perioperative allergic reactions: An international overview and consensus recommendationsBr J Anaesth 2019 123(1):e50-e64. [Google Scholar]
[6]. Starsmore L, Durbridge J, Anaesthetic implications of a patient with cold-induced anaphylaxis presenting to the labour wardInt J Obs Anes 2019 37:125-28. [Google Scholar]