Laparoscopy is endoscopic visualisation of the peritoneal cavity usually assisted by a pneumoperitoneum that distends and separates the abdominal wall from its contents. The abdominal cavity is inflated with a suitable gas, most commonly carbon dioxide (CO2), to create the pneumoperitoneum [1].
From the early 1970s, laparoscopic procedures were used to treat and diagnose various gynecological conditions [2]. It became well established due to advantages like reduced postoperative pain, improved cosmesis and reduced hospital stay [3]. Laparoscopic procedures are also associated with several undesirable cardiorespiratory perturbances. A combination of several factors, namely pneumoperitoneum, patient position, anaesthesia and hypercapnia from the absorbed CO2 are responsible for the haemodynamic changes observed during laparoscopy. These includes increased HR, increased arterial pressures, increased systemic vascular resistance and increased pulmonary vascular resistance [2,4]. Increased plasma catecholamines and vasopressin levels during pneumoperitoneum is associated with changes in total peripheral resistance [5,6].
Cardiovascular events occurring during induction, intubation and surgical stimulation are usually transient and well tolerated in healthy individuals. However, these may be hazardous to individuals with hypertension, coronary artery disease or cerebrovascular diseases [5,7] and can result in potentially life threatening effects like pulmonary oedema, myocardial insufficiency [8], dysrhythmias and cerebrovascular accidents [6].
Various pharmacological agents like nitroglycerine, beta blockers, magnesium sulphate, calcium channel blockers and opioids have been used to provide haemodynamic stability during pneumoperitoneum with their own limitations [8-11].
There is a need for a single drug which can reduce the haemodynamic changes during laparoscopy with minimal adverse effects. The drug must be capable of being used in all age groups, should have minimal adverse effects and should have quick recovery.
Alpha-2 (α2) adrenergic agonists have shown promising results in maintaining the baseline haemodynamic parameters during laparoscopic surgeries with minimal adverse effects [11-13]. These agents help in attenuating the haemodynamic response to tracheal intubation, surgical stimulus, creation of pneumoperitoneum, extubation and in maintaining postoperative analgesia and sedation.
Alpha-2 adrenergic drugs are useful in attenuating the haemodynamic responses produced by pneumoperitoneum. However, not many studies have been carried out on studying the comparative effect of these two drugs especially in laparoscopic onco-surgeries. Onco-surgeries are extensive, produces more inflammatory responses with more postoperative pain when compared to other laparoscopic surgeries. Hence, this trial was taken up to compare intravenous dexmedetomidine and clonidine on haemodynamic response in laparoscopic lower abdominal onco-surgeries.
The aim of the trial was to compare clonidine and dexmedetomidine in attenuating haemodynamic stress response during laparoscopic lower abdominal onco-surgeries. According to null hypothesis, the difference (in mean value of various parameters) between the two groups in attenuating haemodynamic stress response during laparoscopic lower abdominal onco-surgeries was not statistically significant.
Materials and Methods
A comparative, randomised controlled trial was conducted at Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India, during the period of December 2018 to May 2019. The trial was approved with the Institutional Ethical Committee and the trial was registered with CENTRAL TRIAL REGISTRY OF INDIA with reg. number CTRI/2019/06/019683.
Sample size calculation: The sample size was estimated with 80% power and 95% confidence limit by assuming equal sample size among two arm groups. The total sample size calculated was 48.
Inclusion criteria
Patients aged between 18-60 years and who gave informed written consent
American Society of Anaesthesiologists (ASA) physical status classification Grade I and II
Carcinoma stage I and II
Exclusion criteria
Unwilling patients
Age below 18 and above 65 years
ASA classification of physical status Grade III and IV
Patients with cardiac dysfunction, hepatic and renal diseases, psychiatric disorders and allergic disorders
Carcinoma stage III and IV
Study Procedure
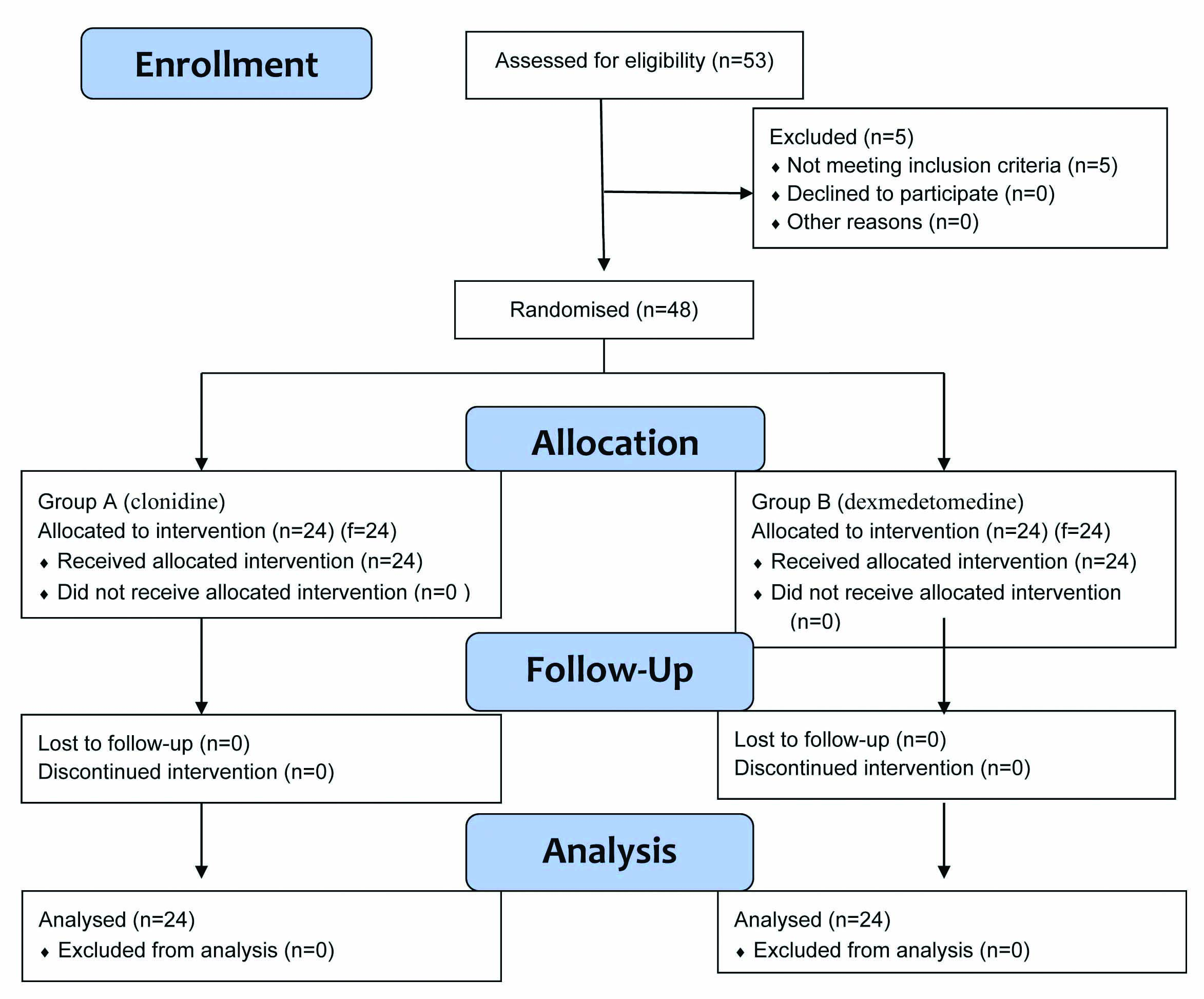
A total of 53 patients were enrolled in which five were not eligible (did not meet inclusion criteria) for the study. A total of 48 patients were allocated into two groups, group A with 24 patients and group B with 24 patients. All 48 patients received intervention and all were analysed. As shown in [Table/Fig-1].
After the detailed pre-anaesthetic evaluation, informed written consent was obtained. Patients were advised nil by mouth as per American Society of Anaesthesiology (ASA) fasting guidelines and were pre-medicated with tablet pantoprazole 40 mg and tablet alprazolam 0.5 mg orally on the night prior to the surgery.
On shifting the patients to the operating room, ASA standard monitors were connected and baseline reading of parameters were noted. An intravenous access was secured and intravenous fluid ringer’s lactate was started. All patients were randomised into group A or B based on computer generated table of random numbers. It was a single blinded study as none of the patients were aware of which group they were allocated.
Group A: (24 patients) calculated dose of intravenous clonidine (1 mcg/kg) was diluted to 50 mL with normal saline and was given via infusion pump over 15 minutes as bolus.
Group B: (24 patients) calculated dose of intravenous dexmedetomedine (1 mcg/kg) was diluted to 50 mL with normal saline and was given via infusion pump over 15 minutes as bolus.
Once the bolus infusion of the trial drug was completed, Patient was pre-oxygenated for three minutes with 100% oxygen. Patient was pre-medicated with injection midazolam 0.02 mg/kg plus injection fentanyl 2.0 μg/kg and was induced with injection propofol 2 mg/kg and muscle relaxant used was injection rocuronium 0.8 mg/kg. Patient was intubated with appropriate sized, cuffed endotracheal tube and put on intermittent positive pressure ventilation and was maintained with nitrous oxide and oxygen in the ratio of 33:66, 0.6% isoflurane and injection rocuronium (0.2 mg/kg).
The CO2 was insufflated into the peritoneal cavity (at a rate of 2 L/min) to create pneumoperitoneum. Intra-abdominal pressure was maintained to 10-14 mmHg and EtCO2 was maintained below 35 mmHg at any course of the procedure.
Following were the parameters recorded during the trial at Induction, pneumoperitonium, intraoperative period and at extubation:
Heart rate
Systolic blood pressure
Diastolic blood pressure
Mean arterial pressure
At the end of surgical procedure, once the reversal criteria was obtained, residual paralysis was reversed with inj. neostigmine 0.05 mg/kg and inj. glycopyrrolate 8 μg/kg, and the patient was extubated after extubation criteria was obtained. Patient was monitored and shifted to the Postanaesthesia Care Unit (PACU). Inj. atropine (0.01 mg/kg) was given intravenously when bradycardia was noted. Inotropes and vasodilator were kept ready to counter hypotension or hypertension.
Any side effects like bradycardia, hypotension and other complications were noted. Postoperative pain was assessed by Visual Analogue Scale (VAS) and score more than 4 was treated with Inj. fentanyl 1-2 mcg/kg, Inj. paracetamol 10-15 mg/kg.
Statistical Analysis
All the data were analysed using the statistical software R (V3.6.2). Continuous data are presented in the form of Mean±SD. Discrete data were presented in the form of “n and percentages”. The difference in mean value of the various parameters between the two groups was analysed using Student’s t-test. A p-value of <0.05 was considered to be significant.
Results
A total of 48 patients were randomly allocated in two groups, Group A (clonidine) and Group B (dexmedetomidine) of 24 each, undergoing elective laparoscopic onco-surgeries under general anaesthesia were studied.
There were no significant differences between the two groups with regard to demographic data such as age and weight. All the cases were females so the groups were comparable in relation to gender also [Table/Fig-2].
Demographic Profile (Mean±SD).
| Patient characteristics | Group A (Clonidine) | Group B (Dexmedetomidine) | p-value |
|---|
| Mean±SD | Mean±SD |
|---|
| Age (Years) | 46.76±8.17 | 46.24±9.70 | 0.835 |
| Weight (Kg) | 55.76±7.28 | 56.08±6.06 | 0.867 |
Student t-test; p*<0.05 significant
In the present trial, with regards to the mean values of the HR, both groups showed reduction in the HR compared to basal values. Statistically significant reduction in the HR was noticed in group B as compared to group A at 12th minute of infusion (p=0.008), at the end of infusion (p=0.014), before intubation (p=0.005), 10 minutes after intubation (p=0.008) and immediately after Pneumoperitonium (PP) (p=0.045) as shown in [Table/Fig-3].
Comparison of Heart Rate (HR) between the two groups.
| Time interval | Heart rate Mean±SD | Statistical significance (Student t-test) |
|---|
| Group A | Group B |
|---|
| Mean | SD | Mean | SD | p-value | Remark |
|---|
| Baseline | 82.00 | 20.14 | 83.40 | 12.41 | 0.769 | NS |
| At 6 minutes of infusion | 78.92 | 12.00 | 72.96 | 10.88 | 0.072 | NS |
| At 12 minutes of infusion | 75.44 | 10.71 | 67.32 | 10.03 | 0.008 | S |
| After infusion | 74.36 | 12.56 | 66.28 | 9.77 | 0.014 | S |
| Before intubation | 76.12 | 9.49 | 68.72 | 8.35 | 0.005 | S |
| After intubation | 79.52 | 9.89 | 75.36 | 9.31 | 0.132 | NS |
| 10 minutes after intubation | 77.92 | 9.60 | 71.32 | 7.21 | 0.008 | S |
| Before pneumoperitoneum (PP) | 76.96 | 10.89 | 72.16 | 9.97 | 0.111 | NS |
| After PP | 81.48 | 11.59 | 75.68 | 8.02 | 0.045 | S |
| After 20 minutes PP | 79.16 | 9.81 | 74.52 | 8.72 | 0.084 | NS |
| After 40 minutes PP | 80.56 | 9.13 | 75.32 | 9.96 | 0.058 | NS |
| After 60 minutes PP | 78.64 | 8.01 | 75.00 | 9.16 | 0.145 | NS |
| After 90 minutes PP | 78.58 | 8.16 | 73.85 | 7.98 | 0.075 | NS |
| After 120 minutes PP | 76.00 | 10.48 | 74.00 | 10.01 | 0.652 | NS |
| End PP | 76.16 | 8.56 | 72.84 | 7.59 | 0.153 | NS |
| Before extubation | 73.60 | 7.07 | 74.36 | 8.49 | 0.732 | NS |
| After extubation | 82.00 | 9.15 | 80.28 | 10.73 | 0.545 | NS |
S: Significant; NS: Not significant
There were three occasions in three different patients when intravenous atropine (dose-0.01 mg/kg) was given to combat the bradycardia in dexmedetomidine group (group B).
There were no statistically significant changes in Systolic Blood Pressure (SBP) between the two groups. But group B when was compared to group A after intubation, pneumoperitoneum and extubation, it showed better attenuation of the haemodynamic response to extubation which was statistically significant (p=0.006) [Table/Fig-4,5]. At 6 minutes after infusion, there was statistically significant difference in Mean Arterial Pressure (MAP) (p=0.039) [Table/Fig-6].
Comparison of systolic blood pressure between the two groups (Mean and SD).
| Time interval | SBP | Mean±SD | Statistical significance |
|---|
| Group A | Group B |
|---|
| Mean | SD | Mean | SD | p-value | Remark (Student t-test) |
|---|
| Baseline | 129.64 | 11.47 | 128.20 | 9.85 | 0.636 | NS |
| At 6 minutes of infusion | 120.60 | 8.80 | 116.44 | 7.13 | 0.073 | NS |
| At 12 minutes of infusion | 110.64 | 9.31 | 107.80 | 6.93 | 0.227 | NS |
| After infusion | 106.80 | 9.06 | 104.80 | 7.99 | 0.412 | NS |
| Before intubation | 107.04 | 11.74 | 105.20 | 7.78 | 0.517 | NS |
| After intubation | 112.72 | 15.59 | 113.60 | 8.96 | 0.808 | NS |
| 10 minutes intubation | 107.20 | 13.21 | 106.48 | 10.51 | 0.832 | NS |
| Before pneumoperitoneum (PP) | 114.04 | 15.09 | 106.88 | 12.25 | 0.072 | NS |
| After PP | 121.16 | 12.38 | 115.68 | 9.87 | 0.090 | NS |
| After 20 minutes PP | 111.36 | 9.61 | 114.80 | 9.26 | 0.204 | NS |
| After 40 minutes PP | 114.48 | 10.08 | 111.92 | 8.70 | 0.341 | NS |
| After 60 minutes PP | 116.04 | 8.65 | 113.08 | 9.48 | 0.262 | NS |
| After 90 minutes PP | 118.00 | 8.77 | 116.25 | 7.51 | 0.507 | NS |
| After 120 minutes PP | 114.18 | 15.11 | 116.83 | 9.90 | 0.621 | NS |
| End PP | 113.64 | 13.59 | 114.88 | 8.09 | 0.691 | NS |
| Before extubation | 113.08 | 12.27 | 116.28 | 8.72 | 0.293 | NS |
| After extubation | 127.56 | 12.57 | 125.28 | 10.37 | 0.488 | NS |
S: Significant; NS: Not significant
Comparison of systolic blood pressure after intubation, pneumoperitoneum and extubation.
| SBP | Group | N | Mean difference | SD | t | p-value (Student t-test) | Remarks |
|---|
| Intubation | Group A | 24 | -5.68 | 9.83 | 1.131 | 0.264 | NS |
| Group B | 24 | -8.40 | 6.93 |
| Pnuemo-peritonium | Group A | 24 | -7.12 | 10.25 | 0.609 | 0.545 | NS |
| Group B | 24 | -8.80 | 9.23 |
| Extubation | Group A | 24 | -14.48 | 8.08 | 2.877 | 0.006 | S |
| Group B | 24 | -9.00 | 5.04 |
S: Significant; NS: Not significant
Comparison of mean arterial pressure between the two groups.
| Time interval | MAP | Mean±SD | Statistical significance (Student t-test) |
|---|
| Group A | Group B |
|---|
| Mean | SD | Mean | SD | p-value | Remark |
|---|
| Baseline | 102.00 | 11.42 | 98.48 | 10.69 | 0.266 | NS |
| At 6 minutes of infusion | 92.28 | 7.00 | 88.16 | 6.70 | 0.039 | S |
| At 12 minutes of infusion | 84.24 | 8.30 | 81.68 | 7.54 | 0.259 | NS |
| After Infusion | 80.64 | 10.04 | 80.28 | 7.20 | 0.885 | NS |
| Before intubation | 82.36 | 11.70 | 81.48 | 7.67 | 0.754 | NS |
| After intubation | 86.84 | 14.50 | 88.12 | 9.11 | 0.710 | NS |
| 10 minutes intubation | 80.72 | 10.18 | 81.36 | 8.46 | 0.810 | NS |
| Before Pneumoperitonium (PP) | 89.28 | 10.04 | 84.04 | 9.28 | 0.061 | NS |
| After PP | 94.44 | 9.82 | 91.96 | 8.69 | 0.349 | NS |
| After 20 minutes PP | 86.36 | 8.92 | 88.52 | 6.57 | 0.334 | NS |
| After 40 minutes PP | 89.32 | 7.94 | 87.48 | 7.98 | 0.418 | NS |
| After 60 minutes PP | 90.46 | 7.19 | 89.08 | 6.97 | 0.504 | NS |
| After 90 minutes PP | 93.05 | 8.17 | 88.75 | 7.46 | 0.094 | NS |
| After 120 minutes PP | 93.55 | 6.62 | 88.82 | 6.76 | 0.113 | NS |
| End PP | 90.00 | 8.43 | 88.88 | 9.33 | 0.662 | NS |
| Before extubation | 89.08 | 8.72 | 90.80 | 9.36 | 0.510 | NS |
| After extubation | 99.13 | 7.71 | 97.52 | 10.17 | 0.538 | NS |
S: Significant; NS: Not significant
The diastolic blood pressure showed statistically significant lower values in Group B compared to the group A at 6 minutes of infusion, before PP and at the end of PP, as shown in the [Table/Fig-7].
Comparison of diastolic blood pressure between the two groups.
| Time interval | DBP | Mean±SD | Statistical significance (Student t-test) |
|---|
| Group A | Group B |
|---|
| Mean | SD | Mean | SD | p-value | Remark |
|---|
| Baseline | 84.56 | 9.18 | 83.76 | 9.68 | 0.766 | NS |
| At 6 minutes of infusion | 77.28 | 6.72 | 73.00 | 7.51 | 0.039 | S |
| At 12 minutes of infusion | 70.92 | 7.19 | 67.52 | 8.03 | 0.121 | NS |
| After infusion | 67.64 | 8.56 | 67.16 | 7.81 | 0.837 | NS |
| Before intubation | 69.00 | 10.42 | 68.20 | 7.99 | 0.762 | NS |
| After intubation | 72.76 | 12.63 | 71.68 | 8.20 | 0.721 | NS |
| 10 minutes intubation | 67.32 | 9.20 | 66.60 | 9.71 | 0.789 | NS |
| Before pneumoperitoneum (PP) | 76.44 | 9.68 | 71.32 | 7.88 | 0.046 | S |
| After PP | 79.08 | 12.54 | 76.76 | 7.63 | 0.433 | NS |
| After 20 minutes PP | 71.96 | 7.40 | 72.72 | 5.91 | 0.690 | NS |
| After 40 minutes PP | 75.16 | 8.51 | 73.16 | 8.00 | 0.396 | NS |
| After 60 minutes PP | 76.36 | 7.74 | 75.75 | 8.35 | 0.792 | NS |
| After 90 minutes PP | 78.95 | 8.08 | 74.30 | 8.04 | 0.080 | NS |
| After 120 minutes PP | 78.00 | 5.74 | 73.55 | 5.61 | 0.081 | NS |
| End PP | 76.12 | 7.26 | 71.92 | 7.50 | 0.050 | S |
| Before extubation | 75.40 | 7.21 | 75.08 | 9.26 | 0.892 | NS |
| After extubation | 83.52 | 7.86 | 81.04 | 10.08 | 0.337 | NS |
S: Significant; NS: Not significant
In the present trial, hypotension episodes were not encountered in any of the case of both the trial groups. But bradycardia episodes were observed in three patients in dexmedetomidine group (group B), which required atropine 0.01 mg/kg. No other complications were observed [Table/Fig-8].
Comparison of adverse effects between two groups.
| Adverse effects | Group A (n=24) | Group B (n=24) |
|---|
| Bradycardia | 0 | 3 (12%) |
| Hypotension | 0 | 0 |
Discussion
Laparoscopic surgery has evolved as a wonderful tool for surgeons since 1901 when it was first introduced by Kelling. In 1987 milestone was achieved after laparoscopic cholecystectomy was performed by Philip Mouret for first time [14]. Laparoscopic surgeries provide many benefits but at the cost of its own disadvantages causing haemodynamic fluctuations [2-6].
Clonidine is a centrally acting selective partial α2 agonist (α2: α1=220:1). It is known to induce sedation, decrease anaesthetic drug requirement and improve perioperative haemodynamics by attenuating Blood Pressure (BP) and HR response to surgical stimulation and protecting against perioperative myocardial ischaemia. It provides sympatho-adrenal stability and suppresses renin angiotensin activity [6].
Dexmedetomidine is a highly selective, potent and specific α2 agonist (α2:α1=1620:1). It is 7-10 times more selective for α2 receptors compared to clonidine. Similar to clonidine, dexmedetomidine also attenuates the haemodynamic response to tracheal intubation, decreases plasma catecholamine concentration during anaesthesia and decreases perioperative requirements of inhaled anaesthetics [6]. The α2 adrenergic mechanism causes dose-dependent reduction in BP and HR. In addition to that dexmedetomidine has analgesic, anxiolytic and sedative effects.
A wide variety of agents are being used both during premedication and induction. Beta blockers, α2 agonists, magnesium sulfate, opioids, vasodilators and gasless approach have been tried to negate the haemodynamic variations [8-11].
Hazra R et al., compared the effects of clonidine 1 μg/kg and dexmedetomidine 1 μg/kg given intravenously over 15 minutes prior to induction on haemodynamic responses during laparoscopic cholecystectomy and they found that dexmedetomidine was more effective in attenuating haemodynamic response to pneumoperitoneum when compared with clonidine [12]. They also found chances of bradycardia were more with dexmedetomidine. These results are comparable to present trial, but were statistically insignificant.
Anil Kumar V, compared clonidine 1 μg/kg with dexmedetomidine 0.8 μg/kg 20 minutes before induction [15]. Patients in group dexmedetomidine showed better control of arterial pressures. No significant episodes of hypotension were found in either of the groups. They concluded clonidine and dexmedetomidine attenuates haemodynamic response to pneumoperitoneum, dexmedetomidine being more effective in this regard. Similar results were found in present trial.
Kumar S et al., compared the effects of clonidine 2 μg/kg versus dexmedetomidine 1 μg/kg given intravenously prior to induction, on haemodynamic responses during laparoscopic cholecystectomy [16]. They noticed 1 μg/kg dose of dexmedetomidine is more effective than 1 μg/kg of clonidine and its effect is comparable to 2 μg/kg of clonidine.
Kholi AV et al., compared the attenuation of haemodynamic responses to induction, intubation and creation of pneumoperitoneum, surgical stimulation and extubation under general anaesthesia in patients undergoing laparoscopic cholecystectomy [17]. Their results showed that dexmedetomidine and clonidine in a dose of 1 mcg/kg intravenously cause significant attenuation of pressor response and provide significant postoperative sedation and analgesia than control. However, dexmedetomidine caused better attenuation of pressor response and provided better analgesia and sedation than clonidine.
Chiruvella S et al., compared the effects of clonidine 1 μg/kg versus dexmedetomidine 1 μg/kg given intravenously over 15 minutes prior to induction for haemodynamic stability during laparoscopic cholecystectomy and found that dexmedetomidine was more effective in attenuating haemodynamic response to pneumoperitoneum when compared with clonidine [18].
Sharma S et al., compared dexmedetomidine (1 mcg/kg) and clonidine (1 mcg/kg) premedication in perioperative haemodynamic stability and postoperative analgesia in laparoscopic cholecystectomy [19]. It was found that the dexmeditomidine showed better haemodynamic profile and postoperative analgesia. The trial concluded that Alpha-2 agonists specially dexmedetomidine produce diverse responses including analgesia, anxiolysis, sedation and sympatholysis. Similar results were found in the present trial.
Paliwal N et al., compared the attenuating effects of clonidine and dexemedetomidine on haemodynamic responses during intubation and pneumoperitoneum [20]. It was concluded that dexmedetomidine is more effective than clonidine in attenuating haemodynamic responses of intubation and pneumoperitoneum. The present trial showed similar results. The dexmedetomidine shows greater haemodynamic stability in the above mentioned studies as it is highly selective, potent and specific α2 agonist.
As oncological patients show more inflammatory response, these drugs (clonidine and dexemedetomidine) effectively blunts haemodynamic stress responses and reduce release of inflammatory mediators produced during pneumoperitoneum and intraoperatively. In the present trial, it was found that dexemedetomidine caused better attenuation of pressor response, better analgesia and sedation than clonidine in laparoscopic lower abdominal onco-surgical patients. Only three patients had bradycardia which was effectively managed with Inj. atropine and no other complications were noted.
Limitation(s)
The present trial compares various effects of clonidine and dexmedetomidine in laparoscopic surgeries in ASA I and II patients only. We could have considered Electrocardiograph (ECG) monitoring and sedation scores for the study, which was another limitation of the present trial. Further definite statistical statements cannot be made due to the small sample size of current trial, so broad randomised trials with larger sample size and a longer duration of follow-up are required to reach a consensus.
Conclusion(s)
To conclude, clonidine or dexmedetomidine effectively attenuate the haemodynamic response in patients undergoing laparoscopic lower abdominal onco-surgeries when administered as intravenous bolus dose. The dexmedetomidine causes bradycardia which can be easily combatted with atropine. However, while choosing the alpha-2 agonist in achieving the haemodynamic stability, the dexmedetomidine is better than clonidine.
Student t-test; p*<0.05 significant
S: Significant; NS: Not significant
S: Significant; NS: Not significant
S: Significant; NS: Not significant
S: Significant; NS: Not significant
S: Significant; NS: Not significant