Hair has attracted more attention for its cosmesis than for its medical relevance. It is one of the most common complaints among patients visiting Outpatient Department (OPD), causing diagnostic confusion to the Dermatologists because of its multiple causes. It is usually recognised more readily by females than males [1,2]. There are different causes of diffuse hair loss, the most common being Acute Telogen Effluvium (ATE), followed by Female Pattern Hair Loss (FPHL) and Chronic Telogen Effluvium (CTE). Telogen Effluvium (TE) is a self limiting disorder which usually occurs two to three months after a triggering event and is characterised by sudden onset, and rapid, diffuse, excessive shedding of normal club hairs [3]. Androgenetic alopecia or patterned hair loss is characterised by gradual loss of terminal hair in a patterned distribution. In male patterned hair loss, there is progressive involvement of frontal, temporal, mid scalp and vertex region, whereas in FPHL there is incomplete involvement of these regions with preservation of frontal hairline [4].
All the previous studies assessing the QoL in females with hair loss have been conducted outside India and also were focused mainly on FPHL patients [15-17]. As such, Indian studies assessing the QoL both in FPHL and TE are lacking and hence, authors planned this study to assess the impact of diffuse hair loss on the QoL among South Indian female patients using the DLQI, and also to compare the DLQI among FPHL and TE, which in turn will help in providing better treatment outcome.
Materials and Methods
The present study was a hospital based cross-sectional study carried out over a period of one year from February 2019 to February 2020 in the Dermatology OPD at a tertiary care centre in South India. The study was approved by the Institutional Ethics Committee (IEC no: VMKVMC&H/IEC/19/11). Written consent was obtained from all patients prior to enrollment.
Inclusion and Exclusion criteria: All female patients more than 18 years, presenting to the OPD with complaints of diffuse hair loss were recruited in the study and the exclusion criteria being patients who were already on treatment for hair loss in the past one month, those with underlying psychiatric illness, and those on any chemotherapeutic drugs.
Study Procedure
A total of 100 patients were enrolled in the study which included 52 patients of ATE followed by 30 FPHL and 18 CTE patients. All the demographic details and any history of prior precipitating factors such as medical illness or surgery, psychological stress, postpartum period etc., associated with worsening of hair loss were elicited and recorded.
All patients were then subjected to hair pull test, a simple clinical test done by firmly pulling around 20-60 hairs grasped between the thumb, index and middle fingers from the base of the hairs tugged away from the scalp [18]. The test was considered positive if there are more than 10% hairs pulled away from the scalp, which suggests active hair shedding. The final diagnosis of each condition was made based on a thorough history and clinical examination findings.
Severity of hair loss in FPHL was assessed using Ludwig’s scale ranging from grade 1 to 3 based on the severity of hair loss [19]. QoL was assessed in all patients based on the DLQI scale modified for alopecia by Zhuang XS et al., DLQI has 10 questions, covering six domains of QoL- symptoms and feelings (Q1,2), daily activities (Q3,4), leisure activities (Q5,6), work and schooling (Q7), personal relationships (Q8,9), and treatment of alopecia (Q10) [15]. Each question is answered by a simple tick box and scored 0-3 [Table/Fig-1]. The sum of the scores for each question was taken and categorised as no effect (0-1), mild effect (2-5), moderate effect (6-10), severe effect (11-20), and extremely large effect (21-30) on the QoL.
Dermatology life quality index questionnaire.
| Questions | 0 (Not at all) | 1 (A little) | 2 (A lot) | 3 (Very much) |
|---|
| Over the last week, how have you been affected by alopecia? Have you felt burning, pain, itching, irritation or oil on your scalp? | | | | |
| Over the last week, how embarrassed, frustrated or self-conscious have you been because of your alopecia? | | | | |
| Over the last week, how much has your alopecia interfered with your shopping or other outdoor activities? | | | | |
| Over the last week, how much has your alopecia influenced your hair style? Do you need to wear a hat, wig or special hair type to cover the thinner area? | | | | |
| Over the last week, how much has your alopecia affected any social or leisure activities? | | | | |
| Over the last week, how much has your alopecia made it difficult for you to do any sport or hobbies? | | | | |
| Over the last week, has your alopecia prevented you from working or studying? | | | | |
| Over the last week, how much has your alopecia created problems with your partner or any of your close friends or relatives? | | | | |
| Over the last week, how much has your alopecia caused any sexual difficulties? | | | | |
| Over the last week, how much of a problem has the treatment for your alopecia been, for example by making your home messy, or by taking up time? | | | | |
Statistical Analysis
The findings were recorded in a proforma for analysis and interpretation of data. The data gathered were compiled, coded and then entered in Statistical Package for the Social Sciences (SPSS) spreadsheets. Statistical analysis was done using SPSS software version 23.0. Mean±SD was calculated for quantitative variables. Analysis of variance (ANOVA) test was used to compare mean values of quantitative data, while Fisher’s-exact test was used to analyse qualitative data. Post-hoc ANOVA was used to test the statistical significance within the groups. The p-value <0.05 was considered statistically significant.
Results
Majority of the study subjects were in the age group of 18-39 years (64%). The mean age of the study population was 35.36±10.30 years. Majority of patients had a history of hair loss less than six months duration (62%). However, the mean duration of disease was longer in CTE and statistically significant as compared to FPHL and ATE (p-value=0.0001). Positive family history was observed in 17 (56.67%) patients with FPHL and none in other subtypes. Majority of patients with FPHL belonged to Ludwig’s Grade 2 in 14 (46.66%), followed by Grade 1 in 9 (30.0%) and Grade 3 in 7 (23.33%) patients. Hair pull test was significantly positive in females with ATE as compared to FPHL and CTE (p-value=0.007). The mean duration of hair loss was 8.14±8.639 months [Table/Fig-2].
Comparison of major demographic and clinical characteristics among different alopecias.
| Parameter | Acute telogen effluvium (n=52) | Female pattern hair loss (n=30) | Chronic telogen effluvium (n=18) | p-value |
|---|
| Age group (years) |
| 18-29 | 18 (34.62%) | 8 (26.67%) | 5 (27.78%) | |
| 30-39 | 16 (30.77%) | 13 (43.33%) | 4 (22.22%) |
| 40-49 | 14 (26.92%) | 6 (20%) | 6 (33.33%) |
| 50-59 | 4 (7.69%) | 3 (10%) | 3 (16.67%) |
| Mean age | 35.27±10.35 | 35.43±9.13 | 35.5±12.41 | 0.996 (ANOVA) |
| Mean age of onset | 35.27±10.351 | 34.87±9.317 | 34.50±12.515 | 0.961 (ANOVA) |
| Duration of disease |
| <6 months | 52 (100%) | 10 (33.33%) | 0 | |
| 6-12 months | 0 | 15 (50%) | 13 (72.22%) |
| >12 months | 0 | 5 (16.67%) | 5 (27.78%) |
| Mean duration of disease (months) | 3.69±1.541 | 10.63±7.247 | 16.83±13.652 | 0.0001* (ANOVA) |
| Family history | 0 | 17 (56.67%) | 0 | 0.0001* (Fisher’s-exact test) |
| Precipitating factors |
| Nil | 7 (13.46%) | 23 (76.67%) | 7 (38.89%) | |
| Preceding medical/Surgical illness | 19 (36.54%) | 2 (6.67%) | 3 (16.67%) |
| Psychological stress | 24 (46.15%) | 5 (16.66%) | 8 (44.44%) |
| Postpartum | 2 (3.85%) | 0 | 0 |
| Hair pull test |
| Positive | 19 (36.54%) | 3 (10%) | 2 (11.11%) | 0.007* (Fisher’s-exact test) |
| Negative | 33 (63.46%) | 27 (90%) | 16 (88.89%) |
*Statistically significant, (p-value <0.05 was considered statistically significant)
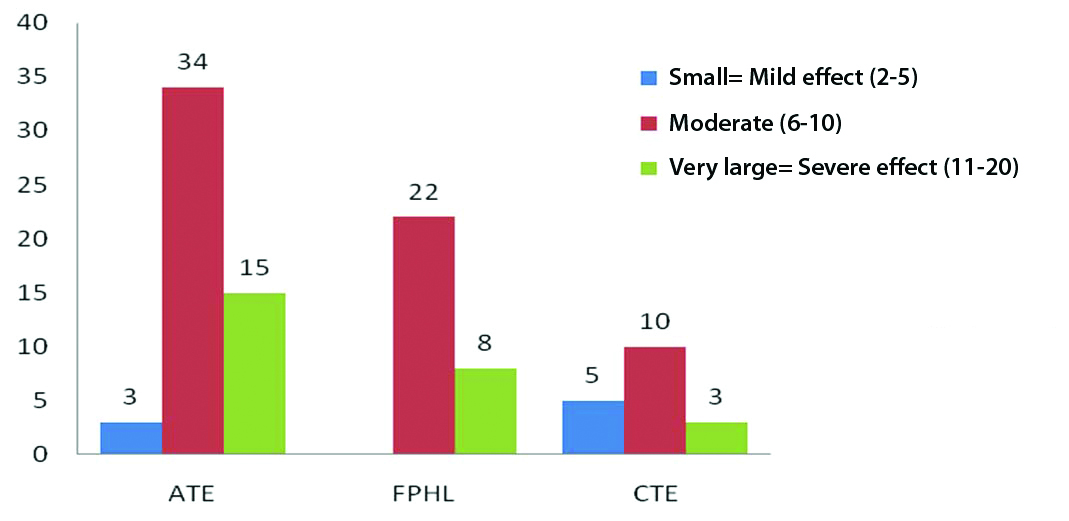
DLQI scores: Of the 100 patients, majority (66%) had moderate effect on the QoL. This was followed by 26% with severe effect and 8% with a mild effect on the QoL [Table/Fig-3]. The mean DLQI of the study population in toto was 8.45±2.17. The mean DLQI values in FPHL (8.77±1.83) and ATE (8.73±1.98) were found to be higher than CTE (7.11±2.78) and the difference is statistically significant (p-value=0.014). When comparing the mean DLQI with disease duration, it was observed that the mean DLQI was highest in those, with a history of hair loss more than one year, whereas, it is lesser comparatively in other two groups. This implies that, there is statistically significant association between the mean DLQI and duration of hair loss in the present study population (p-value=0.0381) [Table/Fig-4].
DLQI in study population.
Comparison of Dermatology Life Quality Index (DLQI) with various parameters.
| Parameter | DLQI Mean±SD | p-value (ANOVA test) |
|---|
| Age (years) |
| 18-29 (n=31) | 8.70±2.253 | p=0.0275* |
| 30-39 (n=33) | 8.63±1.816 |
| 40-49 (n=26) | 8.65±2.038 |
| 50-59 (n=10) | 6.5±2.677 |
| Duration of alopecia |
| <6 months (n=62) | 8.75±1.956 | p=0.0381* |
| 6-12 months (n=28) | 7.57±2.559 |
| >12 months (n=10) | 9.00±1.763 |
| FPHL staging |
| Grade 1 (n=9) | 7.67±1.000 | p=0.0001* |
| Grade 2 (n=14) | 8.14±1.292 |
| Grade 3 (n=7) | 11.43±0.535 |
| Type of hair loss |
| ATE (n=52) | 8.73±1.981 | p=0.014* |
| FPHL (n=30) | 8.77±1.832 |
| CTE (n=18) | 7.11±2.784 |
*Statistically significant, (p-value <0.05 was considered statistically significant)
The mean DLQI in FPHL patients with greater severity grading (i.e., Grade III) is significantly higher than the mean DLQI with lower severity grading in present study (p-value=0.0001). Post-hoc ANOVA was done to find the relation between DLQI and severity grades in Ludwigs staging, and found that the inter differences between Grade 1 and Grade 2 (p-value=0.0001), Grade 2 and Grade 3 (p-value=0.0001) and Grade 1 and Grade 3 were statistically significant (p-value=0.0001) [Table/Fig-5].
Comparison of severity staging between the FPHL grades.
| Post-hoc ANOVA | p-value |
|---|
| Grade 1 and Grade 2 | 0.0001* |
| Grade 2 and Grade 3 | 0.0001* |
| Grade 3 and Grade 1 | 0.0001* |
*Statistically significant; p-value<0.05 was considered statistically significant
Discussion
In present study population, the most common type of hair loss seen was ATE noted in 52% of patients. This was followed by FPHL in 30% and CTE in 18% of patients. This is similar to the observations by Malkud S and Patel KB et al., where the most common type seen was ATE (64.44% and 31%), followed by CTE (15.55% and 22%) and FPHL (11.66% and 10%) respectively [20,21]. Some have included both ATE and CTE in a single category of TE, of which TE (62.2%) was the most common type, like in a study conducted by Deo K et al., [22]. In contrast, CTE and FPHL were the common types in few other studies [23-25]. Poonia K et al., and Shrivastava SB and Sagar V, studied the clinico-aetiological profile of 100 and 200 female patients respectively with non scarring diffuse hair loss and found that, the most common type was CTE (62% and 35.5%), followed by FPHL (22% and 35%) and ATE (16% and 23%), respectively [23,24]. Agarwal S et al., in their study to assess the clinico-aetiological profile of female patients presenting with diffuse hair loss found FPHL to be the most common type seen in 61%, followed by ATE in 25% and CTE in 14% patients [25].
The mean age of the study population was 35.36±10.30 years. Majority of patients in present study were in the age group of 18-39 years (64%). Similar findings were reported by other studies conducted by Malkud S (71.66%), Deo K et al., (83.70%) and Poonia K et al., (70), [20,22,23]. The mean duration of hair loss in our study was 8.14±8.639 months, which is lesser compared to other studies by Deo K et al., (15.64±16.0), Poonia K et al., (14.4±14.2), and Agarwal S et al., (18.84±25.5) [22,23,25]. This may be attributed to the higher percentage of patients with ATE in our study as compared to the previous studies, where FPHL and CTE were the common types. However, the mean duration of hair loss in CTE (16.83±13.652) was significantly higher when compared to ATE (3.69±1.541) and FPHL (10.63±7.247) in this study reflecting the longer and persistent nature of hair loss in CTE.
Family history among patients with FPHL is statistically significant (p-value=0.0001, Fisher’s-exact test) when compared to ATE and CTE, which implies that positive family history is seen more frequently in FPHL patients. Gonzalez ME et al., (84.61%) and Siah TW et al., (85%) reported a higher percentage of FPHL patients with positive family history [26,27], whereas Deo K et al., (4.4%) and Poonia K et al., (3%) reported a very lower percentage of FPHL patients with positive family history [22,23]. This difference could be due to different genetic factors in different ethnicities.
DLQI: In present study, it was observed that, majority (66%) had a moderate effect on the QoL. The value of DLQI ranged from 4-12. Mean DLQI of the study population was 8.45±2.17. This is consistent with a Canadian study by Williamson D et al., including 70 females, where the DLQI ranged from zero to 23 with a mean DLQI of 8.3±5.6 [28]. Other studies by Zhuang XS et al., Cartwright T et al., and Tahir K et al., observed a comparatively higher mean DLQI, which is in contrast to our study [15-17]. The above mentioned studies mainly assessed the DLQI among patients with FPHL, whereas present study assessed the DLQI among FPHL as well as ATE and CTE. This may be one of the reasons for comparatively lower mean DLQI of our study population.
DLQI and type of hair loss: Mean DLQI in FPHL was comparatively higher than the mean DLQI in ATE and CTE and it was statistically significant (p-value=0.014, ANOVA). The reason for a higher mean DLQI in FPHL and ATE could be due to early visibility of the patterned hair loss in FPHL to self and the society thereby seeking immediate attention and due to sudden onset shedding of hair in ATE both of which may cause significant anxiety and depression and affect their overall QoL.
DLQI and age: In present study population, it was observed that majority belonging to the younger age group (18-39 years) described significant effect on the QoL, compared to the elderly. Present study findings are in line with another study by Cash TF et al., where young adults were more affected [13]. This suggests that, although psychological distress is common across all age groups, it was more apparent among young females. This may be due to increased psychological needs of the younger age group as they are much more concerned about their beauty and self image. Hence, the need for proper counseling is equally important as medical management in the younger age group, which in turn will have a significant impact on the treatment outcome. Zhuang XS et al., and Tahir K et al., observed no significant difference in the mean DLQI scores with respect to the different age groups [15,17]. Sawant N et al., in contrast to all other studies, showed younger age group to be less affected on the QoL [29].
DLQI and duration of hair loss: The mean DLQI score was higher in patients with disease duration more than one year. Tahir K et al., also studied the mean DLQI with respect to the duration of hair loss and observed an increase in the mean DLQI, as the duration of hair loss increases [17]. Hence, we observed a higher DLQI in patients with longer duration more than one year, in accordance with the above study. Also, we observed a higher DLQI in patients with duration less than six months, which is mainly due to patients with ATE coming under this subset, where the sudden onset of diffuse hair loss in an otherwise normal individual would have seriously affected their self-esteem and overall QoL. However, Zhuang XS et al., and Williamson D et al., observed no significant difference in the mean DLQI scores with respect to the duration of hair loss [15,28].
DLQI and FPHL grading: In present study, Post-hoc ANOVA test was done, comparing the severity staging between the groups and it was observed that, the difference was statistically significant between Ludwig’s stages 1 and 2, between stages 2 and 3, and also between stages 1 and 3. Tahir K et al., also observed a statistically significant difference between all three stages [17]. Thus, the impact of FPHL on QoL is influenced mainly by the extent and visibility of hair loss.
Previous studies have mainly focused on assessing the QoL among females mainly with androgenetic alopecia. However, present study has assessed the QoL in FPHL as well as acute and CTE and also compared the DLQI among these subtypes. The comparison of mean DLQI in present study with similar studies done elsewhere is shown in [Table/Fig-6] [13,15-17,28,30].
Comparison of DLQI with similar studies done elsewhere [13,15,16,17,28,30].
| Authors | Year of study | Study population | Sample size | Diagnosis | Mean DLQI |
|---|
| Cash TF et al., [13] | 1993 | New York | 96 females | Androgenetic alopecia | Not studied |
| Williamson D et al., [28] | 2001 | Toronto, Canada | 60 females | Alopecia in general | 8.3±5.6 |
| Cartwright T et al., [16] | 2009 | London, United Kingdom | 171 females | Androgenetic alopeciaAlopecia areataAlopecia totalis/universalis | 13.01±6.81 |
| Tahir K et al., [17] | 2013 | Lahore, Pakistan | 72 females | Androgenetic alopecia | 13.49±3.91 |
| Zhuang XS et al., [15] | 2013 | China | 125 females | Androgenetic alopecia | 9.62±5.92 |
| Zhang M and Zhang N [30] | 2017 | China | 53 females | Androgenetic alopeciaAlopecia areata | 7.64±6.97 |
| Present study | 2021 | Salem, India | 100 females | Androgenetic alopecia | 8.77±1.832 |
| | | | Acute telogen effluvium | 8.73±1.981 |
| | | | Chronic telogen effluvium | 7.11±2.784 |
Limitation(s)
The major limitation of present study was the smaller sample size and being a hospital based cross-sectional study, the findings may not be generalisable to whole population. Hence, large scale studies are needed to further substantiate our results.
Conclusion(s)
As far as DLQI is concerned, most of the patients have a moderate to severe impact on the QoL. There is a strong association seen between DLQI and age, duration of disease and type of hair loss. QoL seems to be affected more in younger individuals in the age range of 18-39 years. DLQI is significantly affected in females with increased duration of hair loss more than one year. DLQI is also higher in patients with FPHL and ATE as compared to CTE. There was a significant negative impact on the QoL among females with diffuse hair loss and hence psychological aspects of hair loss need to be given utmost importance when evaluating a female with hair loss. Psychological support and counseling should go hand in hand with medical management for an effective therapeutic outcome.
*Statistically significant, (p-value <0.05 was considered statistically significant)
*Statistically significant, (p-value <0.05 was considered statistically significant)
*Statistically significant; p-value<0.05 was considered statistically significant