The primary objective of root canal therapy is to completely debride the pulp space of necrotic pulp tissue, microorganisms and endotoxins. Various iatrogenic errors like inadequate debridement and asymmetrical shaping, especially in curved root canals, may lead to failure of endodontic therapy by developing abnormal root surface strain, ledge, canal center transportation and perforation in the root surface that ends up in root fractures [1].
Introduction of NiTi rotary systems with improved blade designs with varying tapers, diverse cross-sections, superior torsional fracture resistance, non cutting safety tips and variable length of cutting blades in conjunction with the improved metallurgic properties of NiTi alloys has led to improved instrumentation of curved root canals [2,3].
The F6 SkyTaper is a single-file conventional NiTi alloy instrument, with a constant taper of 0.06 and a modified S-shaped cross-section [4]. One Shape is also a single-file conventional Ni-Ti alloy file system with an asymmetrical cross-section. It has additional Apical 1 and Apical 2 files for additional apical enlargement [5]. Navigator EVO is a set of highly flexible multiple files which are thermally treated with a 6% taper and inactive tip [6].
To our knowledge, no previous study has compared the shaping ability of F6 SkyTaper, Navigator EVO and One Shape. Thus, the purpose of this study was to evaluate and compare the canal transportation, canal centering ability, and time taken for preparation of curved root canals after instrumentation with F6 SkyTaper, Navigator EVO and One Shape using CBCT imaging.
Materials and Methods
The present in vitro study was conducted in the Department of Conservative Dentistry and Endodontics, I.T.S Centre for Dental Studies and Research, Ghaziabad, Uttar Pradesh, India in July 2020. The study protocol was approved by the Institutional Ethical Review Committee under protocol number ITSCDSR/IIEC/2016-19/CONS/03.
Inclusion criteria: Extracted human mandibular first molars with intact roots and fully formed apex were included in the study.
Exclusion criteria: Teeth with cracks, fractures or defects, root caries or resorptive defects were excluded from the study.
Sample size calculation: Sample size was estimated based on the results of pilot study which were not included in the main study. The effect size was calculated as 0.6. With 80% power of the study, 5% α error the final sample size was estimated to be 30 using G*power software, version 3.1.9.7 (FranzFaul universitat, Kiel, Germany). The sample size was calculated as 30.
From a total of 61 teeth, 30 extracted human mandibular first molars with two separate curved mesial canals fulfilling the inclusion criteria were taken up for the study. Access opening was done using endo access bur (Dentsply, Maillefer), and thereafter, mesiobuccal canals known to have abrupt canal curvatures were localised and explored with a 10 K-file (Dentsply, Maillefer). Those canals with curvature 20 to 40 degrees were further included in the study as assessed using Schneider’s method using two intersection lines, one drawn along the long axis of the canal and another one drawn at the apical straight portion of the canal [7]. Coronal part of the tooth was sectioned to obtain the final dimension of 18 mm and working length of 17 mm. Distal roots were discarded.
Specimens were randomly alotted into three experimental groups (n=10) according to the rotary NiTi file system used for canal instrumentation as follows:
Group I: F6 SkyTaper (Komet, Brasseler GmbH & Co., Lemgo, Germany)- glide path was prepared with hand files till size 20, followed by instrumentation with F6 SkyTaper 30/6%.
Group II: Navigator EVO (Medin, Czech Republic)- coronal flaring was done with W-XN 25/7%, glide path with W1 10/4%, and W2 15/5%. Shaping was done with W3 20/6%, W4 25/6%, W5 30/6%.
Group III: One Shape (Micro-Mega, Besancon Cedex, France)- hand files no. 10 and 15 were used till the apex, followed by path files G1 (12/3%) and G2 (17/3%) to obtain a glide path. Orifice was shaped using Endoflare. Canal was shaped using file 25/6%, followed by apex preparation file ‘Apical 1’ of size 30/6%.
Canal instrumentation was performed in accordance with the manufacturer’s recommendation; operated by a 16:1 gear reduction handpiece powered by electric torque control motor (Dentsply, Maillefer, Switzerland) and the final apical preparation size was standardised to 30/6% [8].
In Group I, glide path was prepared with hand files till size 20, followed by instrumentation with F6 SkyTaper 30/6%.
In Group II, coronal flaring was done with W-XN 25/7%, glide path with W1 10/4%, and W2 15/5%. Shaping was done with W3 20/6%, W4 25/6%, W5 30/6%.
Group III, hand files no. 10 and 15 were used till the apex, followed by path files- G1 (12/3%) and G2 (17/3%) to obtain a glide path. Orifice was shaped using Endoflare. Canal was shaped using file 25/6%, followed by apex preparation file ‘Apical 1’ of size 30/6%.
For all the three groups, Glyde (Dentsply Maillefer, Switzerland) was used as a lubricant; canals were irrigated with 3 mL of 5% NaOCl solution during instrumentation. Final irrigation was done with 1 mL of 17% Ethylenediaminetetraacetic Acid (EDTA) for one minute followed by a final flush with 3 mL of NaOCl . Every file system set was used to prepare three specimens each, after which the system set was replaced.
Image Analysis
Specimens were embedded in an acrylic base shaped as a mandibular arch [Table/Fig-1]; scanned both preoperatively and postoperatively in the CBCT unit NewTom GiANO at 90 kvp, 3 mA, scan resolution/voxel size of 100 microns and Field of View (FOV) of 8x5 cm for 9.0 sec within the confines of the laser beam position indicators [Table/Fig-2] [9]. Obtained scans and data was stored for image analysis.
Pre-preparation samples embedded in an acrylic base as mandibular arch.

Arch placed in CBCT unit for scanning.

On the NewTom NNT (version 7.0) interactive CBCT imaging software in the MPR tab, each tooth was localised and triangulated in all three orthogonal planes (axial, sagittal, coronal). The distance measurement toolbar was then selected and then the distance tab was selected for linear measurements. The measurement was done from the root apex coronally at four points: 3 mm, 5 mm, 7 mm, and 9 mm, respectively.
The following measurements were taken at these four points [Table/Fig-3] [8]:
Measurement of instrumented root section.
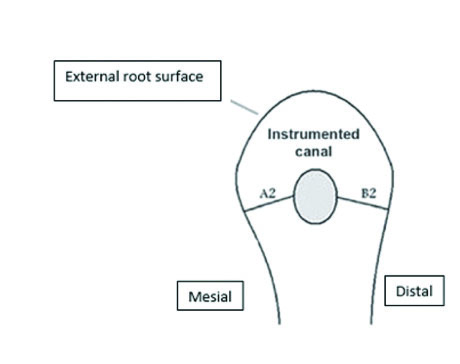
A1- Shortest distance from the mesial edge of the root to the mesial edge of the un-instrumented canal
A2- Shortest distance from the mesial edge of the root to the mesial edge of the instrumented canal
B1- Shortest distance from the distal edge of the root to the distal edge of the un-instrumented canal, and
B2- Shortest distance from the distal edge of the root to the distal edge of the instrumented canal
Calculation of canal transportation and canal centering ability at each level:
1) To calculate the degree of canal transportation at each level, following formula was used:
(A1-A2) - (B1-B2);
2) To calculate the canal centering ability at each level, following ratio was used:
(A1-A2)/(B1-B2) or (B1-B2)/(A1-A2) [8]
The mean working time taken for the cleaning procedure (excluding the time for instrument change and irrigation) was recorded using an electronic stopwatch. The entire procedure was done by a single operator. According to this formula, a result other than 0 will indicate that transportation has occurredin the canal. If these numbers were not equal, the lower figure was considered the numerator of the ratio. According to this formula, a result of 1 will indicate perfect centering [10]. The readings of each sample was recorded and subjected to statistical analysis.
Statistical Analysis
The data collected were evaluated statistically using one-way with Bonferroni post-hoc test to obtain intergroup mean canal transportation. Repeated ANOVA followed by post-hoc Bonferroni tests were used to make an intragroup comparison at different levels. Kruskal-Wallis test followed by Mann-Whitney U test were used to obtain mean canal centering ability. Repeated ANOVA and Wilcoxon Rank Tests were done to make an intragroup comparison at different levels. One-way ANOVA followed by a post-hoc Bonferroni test was done to compare mean time taken by all groups. Tests were done using Statistical Package for the Social Sciences (SPSS) software version 21.0 (SPSS Inc, Chicago, IL). The p-value <0.05 was considered statistically significant.
Results
Total 30 human extracted mandibular first molar teeth were included in the study, divided into three groups with 10 in each group. The mean and standard deviation values for the canal transportation and the canal centering ability at the studied levels by experimental groups are presented in [Table/Fig-4]. Significantly less canal transportation (0.222) and most centered (0.535) preparations were seen in group II (Navigator EVO) followed by group I (F6 SkyTaper) at the 3 mm level [Table/Fig-4].
The comparison of mean canal transportation and mean canal centering ability calculated for Group I (F6 SkyTaper), Group II (Navigator Evo) and Group III (One Shape) at 3 mm, 5 mm, 7 mm and 9 mm.
| Canal transportation | 3 mm | 5 mm | 7 mm | 9 mm |
|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD |
|---|
| Group I | 0.340 | 0.1075 | 0.390 | 0.0738 | 0.550 | 0.0972 | 0.153 | 0.0467 |
| Group II | 0.222 | 0.0873 | 0.255 | 0.1165 | 0.410 | 0.1101 | 0.085 | 0.0580 |
| Group III | 0.390 | 0.0876 | 0.480 | 0.0919 | 0.660 | 0.1174 | 0.155 | 0.0497 |
| p-value | 0.023* | <0.001* | <0.001* | 0.001* |
| Group I vs II | 0.031* | 0.021* | 0.043* | 0.012* |
| Group I vs III | 0.073 | 0.065 | 0.067 | 0.053* |
| Group II vs III | 0.001* | <0.001* | <0.001* | <0.001* |
| Canal centering ability | 3 mm | 5 mm | 7 mm | 9 mm |
| Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Group I | 0.423 | 0.0710 | 0.419 | 0.0753 | 0.303 | 0.0673 | 0.653 | 0.0663 |
| Group II | 0.535 | 0.1192 | 0.550 | 0.0850 | 0.396 | 0.0811 | 0.800 | 0.1312 |
| Group III | 0.400 | 0.667 | 0.382 | 0.0541 | 0.273 | 0.0455 | 0.613 | 0.0631 |
| p-value | 0.017* | 0.001* | 0.027* | 0.001* |
| Group I vs II | 0.021* | 0.033* | 0.035* | 0.023* |
| Group I vs III | 0.063 | 0.077 | 0.068* | 0.075 |
| Group II vs III | 0.027* | 0.001* | <0.001* | <0.001* |
Statistical analysis done with ANOVA and Bonferroni post-hoc test for assessing canal transportation and Kruskal Wallis test followed by Mann-Whitney U test for analysing canal centering ability.
*depicts significant differences between the groups
*p-value <0.05 considered as statistically significant
Maximum transportation (0.390) and least centered (0.400) preparations were seen in group III (One Shape) at the 3 mm level, although it was insignificant (p>0.05) when compared to group I. The intragroup comparison showed maximum transportation (0.660) at 7 mm and the least (0.085) at 9 mm [Table/Fig-4]. On intragroup comparison for canal transportation, insignificant difference was found between 3 mm and 5 mm in all the groups [Table/Fig-5]. The intragroup comparison showed most centered preparations at 9 mm and least at 7 mm. Insignificant difference was found between 3 mm and 5 mm in all the groups [Table/Fig-6].
Intragroup comparison of canal transportation in different groups at different levels.
| Canal transportation | Group I | Group II | Group III |
|---|
| Mean difference | p-value | Mean difference | p-value | Mean difference | p-value |
|---|
| 3 mm vs 5 mm | -1.667 | 0.061 | -0.921 | 0.066 | -1.852 | 0.071 |
| 3 mm vs 7 mm | -2.625 | 0.013* | -2.677 | 0.019* | -2.820 | 0.015* |
| 3 mm vs 9 mm | -2.814 | 0.034* | -2.842 | 0.021* | -2.820 | 0.023* |
| 5 mm vs 7 mm | -2.455 | 0.027* | -2.094 | 0.033* | -2.297 | 0.042* |
| 5 mm vs 9 mm | -2.814 | 0.044* | -2.714 | 0.025* | -2.825 | 0.023* |
| 7 mm vs 9 mm | -2.812 | 0.037* | -2.820 | 0.030* | -2.840 | 0.033* |
Statistical analysis done with Repeated ANOVA followed by post-hoc Bonferroni tests.
*p-value<0.05 considered as statistically significant
Intragroup comparison of centering ability in different groups at different levels. The statistical analysis was done with repeated ANOVA and Wilcoxon rank test.
| Canal centering ability | Group I | Group II | Group III |
|---|
| Mean difference | p-value | Mean difference | p-value | Mean difference | p-value |
|---|
| 3 mm vs 5 mm | -0.086 | 0.061 | -0.851 | 0.72 | -1.225 | 0.081 |
| 3 mm vs 7 mm | -2.680 | 0.031* | -2.524 | 0.045* | -2.555 | 0.032* |
| 3 mm vs 9 mm | -2.805 | 0.026* | -2.805 | 0.017* | -2.814 | 0.042* |
| 5 mm vs 7 mm | -2.680 | 0.043* | -2.530 | 0.015* | -2.680 | 0.024* |
| 5 mm vs 9 mm | -2.810 | 0.035* | -2.812 | 0.013* | -2.807 | 0.027* |
| 7 mm vs 9 mm | -2.805 | 0.032* | -2.807 | 0.021* | -2.812 | 0.035* |
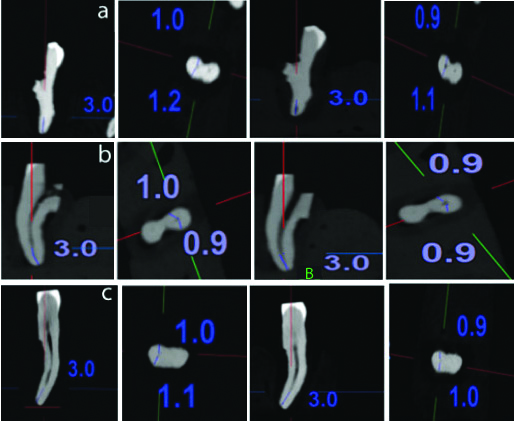
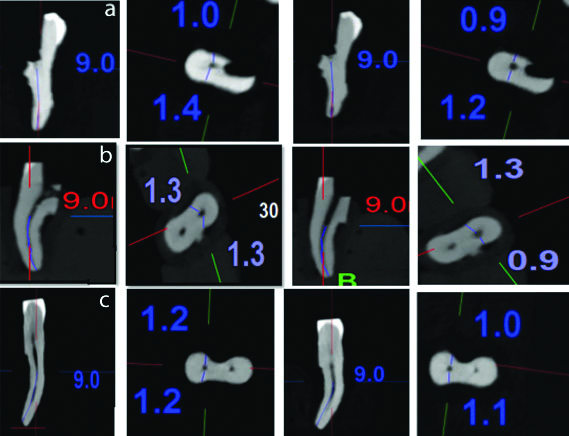
The preoperative and postoperative CBCT images of the canal centering ability at 3 mm, 5 mm, 7 mm and 9 mm are depicted in [Table/Fig-7,8,9 and 10], respectively. On using the post-hoc Bonferroni test, the mean time taken for canal preparation was found to be statistically significant for all the groups with the least time taken (75.72 sec) for group I (F6 SkyTaper) and highest (307.046 sec) for group II (Navigator EVO) [Table/Fig-11].
Preoperative (left) and postoperative (Right) CBCT images of canal centering ability of group I (F6 SkyTaper), Group II (Navigator EVO) and group III (One Shape) at 3 mm.
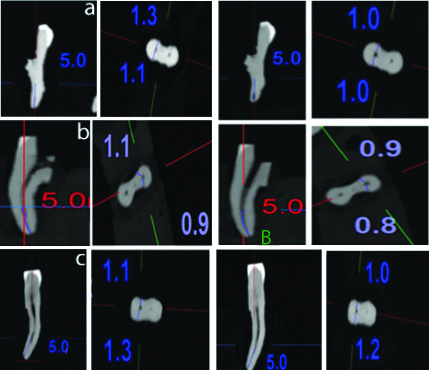
Preoperative (left) and postoperative (Right) CBCT images of canal centering ability of Group I (F6 SkyTaper), Group II (Navigator EVO) and Group III (One Shape) at 5 mm.
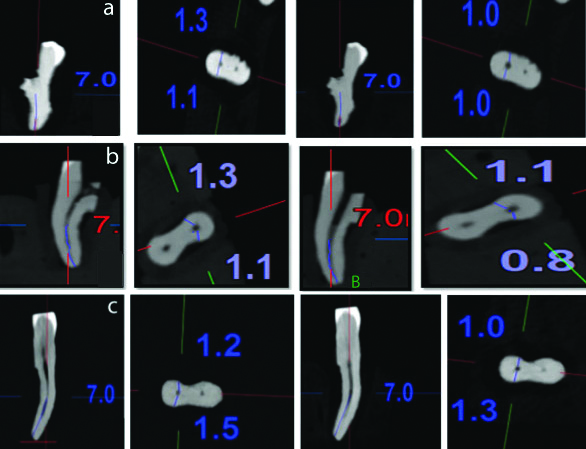
Preoperative (left) and postoperative (Right) CBCT images of canal centering ability of Group I (F6 SkyTaper), Group II (Navigator EVO) and Group III (One Shape) at 7 mm.
Preoperative (left) and postoperative (Right) CBCT images of canal centering ability of Group I (F6 SkyTaper), Group II (Navigator EVO) and Group III (One Shape) at 9 mm
Descriptive statistics of comparison of time taken by different groups for canal preparation.
| Groups | Number of samples | Mean (sec) | SD | F-value | p-value |
|---|
| Group I | 10 | 75.72 | 5.42 | 314.597 | <0.001* |
| Group II | 10 | 307.046 | 37.93 |
| Group III | 10 | 105.098 | 6.64 |
Post-hoc bonferroni test; *p-value <0.05 considered as statistically significant
Discussion
The objective of biomechanical preparation is the removal of infected tissue from the root canal thus, allowing adequate delivery of irrigants and medicaments till the root apex. The limitations of hand files led to the development of the NiTi file system which is better at negotiating curvatures because of improved metallurgic properties and features like elastic memory [8]. With the development of newer endodontic instruments, capable of negotiating challenging root canal configurations, their shaping abilities need to be tested [12].
The present study used CBCT scanning because it is non invasive, accurate and provides 3-dimensional evaluation [13]. The study by Khademi A et al., reported that 30/6% file size was effectively removing debris and smear layer from the apical portion of root canals and hence it was chosen [14]. The root canal curvature was assessed at four levels (i.e., 3 mm, 5 mm, 7 mm and 9 mm from the root apex) as they are more likely to exist in these locations.
In the present study, group II (Navigator EVO) showed least canal transportation and superior centering ability. This could be explained by a triangular cross-section with a three-bladed profile and thermal pretreatment of NiTi alloy, providing increased flexibility [15]; as compared to group I (F6 SkyTaper) and group III (One Shape) that are a conventional NiTi alloy in austenitic phase and hence are comparatively less flexible. Similar results were obtained in studies by Marceliano-Alves MFV et al., Marzouk AM and Ghoneim AG and, Saleh AM et al., suggesting that sequential use of multiple files decreases canal transportation by a gradual increase in the instrument taper unlike the single file systems [16-18].
Studies by Kumar BS et al., Burklein S et al., Kum KY et al., and Bonaccorso A et al., reported that both single and multiple file systems were comparable in their shaping abilities irrespective of glide path preparation or the number of instruments used and only the taper of the instrument plays a role [19-22]. Contrary to their belief, we standardised the apical size and the taper of all the instruments to 30/6% and yet significant differences were observed after canal preparation with different single and multiple file systems.
On comparing Group I (F6 SkyTaper) with group II (One Shape), the former showed lesser, although statistically insignificant, mean canal transportation. The good centering ability of F6 SkyTaper has been attributed to its thin core that decreases the undue dentine cutting at curvatures and provides resilience to the file; increasing debridement of the middle third with lesser dentin cutting in the coronal and apical third [23]. Inferior shaping ability of group III (One Shape) as compared to group I (F6 SkyTaper) was observed at all the tested levels. This can be majorly attributed to the variable cross-section of its 25/6% file size. The 25/6% file is triangular with three symmetrical cutting edges, the middle third is diamond-shaped with two asymmetrical cutting edges and the coronal third has S-shaped cross-section with two cutting edges. This design allows the instrument to progress rapidly into the curved canal creating stresses, resulting in observed canal straightening and apical transportation. The apical 30/6% file which has a symmetrical cross-section progresses in the path created by 25/6%, and is unable to manage the transportation already caused by 25/6% [23]. These results are also in accordance with the findings of Saber SEDM et al., Maitin N et al., who found that asymmetric cross-sectional design of the file considerably reduces its flexibility [24,25].
The intragroup comparison of Mean Canal Transportation at 3 mm, 5 mm, 7 mm and 9 mm was done for group I (F6 SkyTaper), group II (Navigator EVO) and group III (One Shape), and showed that the mean canal transportation at 9 mm was significantly the least and that at 7 mm was significantly the highest for all the groups which is due to the fact that the root curvature began around that region. While at the levels of 3 mm and 5 mm, transportation was comparable.
The canal transportation at 3 mm in all groups except One Shape was less than or equal to 0.35 mm, which was within the critical canal transportation value proposed by Wu MK et al., [26]. The reason for good shaping ability in of group I (F6 SkyTaper) and group II (Navigator EVO) in the apical third could be the non cutting tip design which acts as a guide allowing easy penetration with minimal apical pressure. Although One Shape also had a non-cutting tip, the inferior result can be explained by the triangular tip which reduces the flexibility, thus causing more canal transportation. Observations of Christofzik D et al., corroborated the findings of the present study [27].
The present study assessed the time for canal preparation after the initial glide path preparation with hand file till size 15. Minimum time taken for canal preparation was observed in F6 SkyTaper which used only one file for complete canal preparation. The presence of smaller core diameter in F6 SkyTaper, associated with increased chip space, increased the debris removal capacity and efficiency [28]. In the present study, One Shape took significantly more time for root canal preparation compared to F6 SkyTaper. The reason being the two additional rotary glide path files and an apical preparation files used. Navigator EVO took maximum time for canal preparation, explained by the maximum number of instruments used. Quicker preparation in One Shape may be due to its variable pitch length along the working part which eliminates the chances of threading and binding of the instrument when operating in continuous rotation motion, thus reducing the working time (Bürklein S et al., 2011) [28,29]. The time saved in canal preparation can be further reinvested in additional root canal disinfection [30].
Limitation(s)
The present study did not take into consideration the time taken for instrument change and irrigation. Also, the technique of usage and operator experience influences the time taken for root canal shaping procedure. However, in a clinical scenario, the total time for active instrumentation as well as time for instrument change, cleaning the instrument flutes, and irrigation can affect the choice of instrument for treatment.
Conclusion(s)
Within the limitations of this study, multiple file system (Navigator EVO) showed least canal transportation and highest canal centering ability compared to single file systems (F6 SkyTaper and One Shape). F6 skyTaper showed the fastest preparation of canals while Navigator EVO took the maximum time. However, further research is required to extrapolate the findings of the present study to clinical use. Further investigations are required to assess the cleaning effectiveness and incidence of dentinal defects with the use of these new single-file systems.
Statistical analysis done with ANOVA and Bonferroni post-hoc test for assessing canal transportation and Kruskal Wallis test followed by Mann-Whitney U test for analysing canal centering ability.
*depicts significant differences between the groups
*p-value <0.05 considered as statistically significant
Statistical analysis done with Repeated ANOVA followed by post-hoc Bonferroni tests.
*p-value<0.05 considered as statistically significant
Post-hoc bonferroni test; *p-value <0.05 considered as statistically significant