Arthroscopic reconstruction of the ACL using hamstring grafts is a known and accepted surgical procedure [1]. Arthroscopic techniques for ACL reconstruction have various advantages such as smaller incisions, no disturbance of uninvolved structures and maintenance of normal anatomy.
The position of the bone tunnels, and therefore the graft, is one of the most important factor associated with successful reconstruction [2]. Correct positioning of the tunnels is an important intraoperative variable, and is influenced by the technique [3]. The positioning of the bone tunnels has a fundamental role in the graft’s tensional behaviour during knee range of motion. An incorrect positioning may result in impingement of neoligament at roof of intercondylar notch, or impaction against PCL or may cause abnormal tension on the graft and may cause clinical problems such as loss of range of motion and recurrent instability [4].
Several methods have been described for measuring the positioning of the tunnels in ACL reconstruction surgery [2,5,6]. Among these, the methods of Harner CD et al., and Aglietti P et al., for the femoral tunnel and the method of Stäubli HU and Rauschning W for the tibial tunnel are greatly used [5-7].
Only few prospective studies have evaluated the effect of tunnel placement on functional outcome [2,5]. The present study had the aim of evaluating and comparing the positioning of the bone tunnels in coronal and sagittal plane in a series of patients who underwent ACL reconstruction surgery using the arthroscopic ACL reconstruction with hamstring tendon graft. Also, this study aims to establish its relationship with functional outcome as assessed by IKDC, Lysholm scoring, pivot shift and Lachman test and by patient’s own subjective estimate of knee function before and after surgery.
Materials and Methods
This prospective longitudinal cohort study was conducted at a tertiary healthcare centre in Southern India, Department of Orthopaedics from December 2017 to November 2019. Fifty patients who had isolated ACL substance injury of only one limb were kept under the study, with minimum follow-up of one year. Prior approval was taken from research Ethical Committee at college with no. F.1/Acad/MC/JU/17/17526.
Sample size calculation: It was calculated at 95% confidence interval to verify an expected 79% good knee function postoperatively (as per reference article) [8] at relative allowable error of 12%. Sample size was calculated to be minimum 44 subjects; taking into consideration 15% attrition. Sample size was enhanced and rounded off to 50 subjects.
Inclusion criteria: The patients who had ACL injury alone; confirmed by clinical examination, MRI and arthroscopy after acute inflammatory phase of the injury had subsided and full range of motion and good quadriceps strength had been regained with no extensor lag (usually after 4-6 weeks of injury) were included in study after informed consent was taken.
Exclusion criteria: The patients excluded from the study were with bilateral ACL tear or ACL avulsion injury, patients with any other associated ligament injuries of the knee (complete tear of PCL, medial and lateral collateral ligament requiring treatment), grade 3 meniscal injuries, concurrent musculoskeletal condition e.g., hip or ankle injury, or neuromuscular disorder, limb fractures and those with immature skeleton.
Study Procedure
For this prospective study the patients were evaluated with thorough general and local clinical examination of the knee. Questions of the subjective IKDC questionnaire [9] and the Lysholm Knee Scoring Scale [10] were asked. The IKDC includes seven criteria, based on which it is objectively divided in group A (normal), group B (nearly normal), group C (abnormal), and group D (severely abnormal). Lysholm score takes mechanical locking, instability, pain, and swelling, stair climbing, and squatting into consideration. Clinical examinations was also performed to find out whether there was any joint effusion, crepitation, pain or laxity (Lachman, pivot shift and anterior drawer tests), and knee goniometry was performed.
All the patients included in the study had undergone standard arthroscopic ACL reconstruction technique. Postoperatively, all patients were subjected to similar standard ACL rehabilitation protocol. Postoperatively patients were placed in knee brace. Mobilisation was started immediately, giving priority to the recovery of full extension. Active static quadriceps exercises and ankle pumps were started as soon as the patient recovered from anaesthesia. Closed chain exercises were continued for one month followed by open chain exercises. Weight bearing with 50% of the body weight was allowed with support after one month. Clinical assessment was made in Out Patient Department (OPD) during follow-up first weekly for three weeks then monthly upto six months and at one year. Patients were asked about their own estimate of knee function in postoperative, IKDC questionnaire (IKDC, 2000) and the Gilquist-Lysholm Knee Scoring Scale. Clinical examination was done for any swelling, pain and laxity namely Lachman, pivot shift and anterior drawer tests.
Tunnel positions in radiographs were assessed in postoperative period. The parameters for radiograph were: 1) Postoperative full-extension Anterioposterior (AP) (tibio-fibular overlap within 5 to 15 mm); and 2) lateral radiographs of the knee (less than 5 mm short of femoral condyle overlap). Radiographs with poor quality (inappropriate penetration), extreme obliquity for laterals (more than 5 mm short of femoral condyle overlap), or inappropriately angled, were repeated for appropriate ones.
The position of femoral and tibial tunnels on the postoperative radiographs was independently assessed by two of the observers. Differences between observations were calculated and statistical analysis was done on differences.
A system was used to measure radiographic tunnel position as shown in [Table/Fig-1,2,3,4 and 5] for all parameters. The measurements were converted to percentage to account for variation in radiographic magnification and skeletal size.
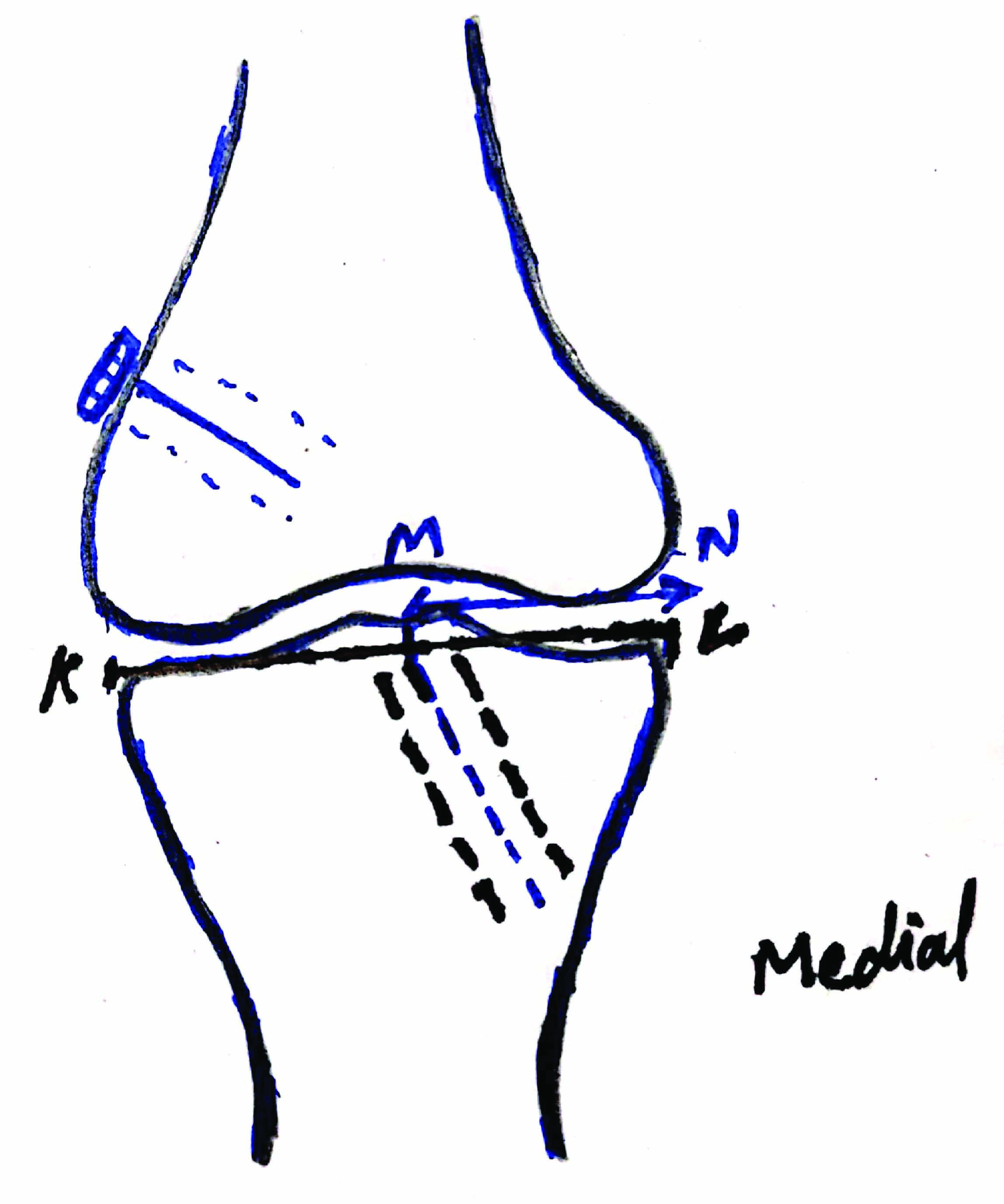
Sketch of knee joint with lower end femur and proximal tibia anteroposterior view showing illustration of the method to measure the distance of center of tibial tunnel (point M) from medial edge of tibia (N) on anteroposterior radiograph. Black line KL is the distance from the medial border to the lateral border of the tibial plateau.
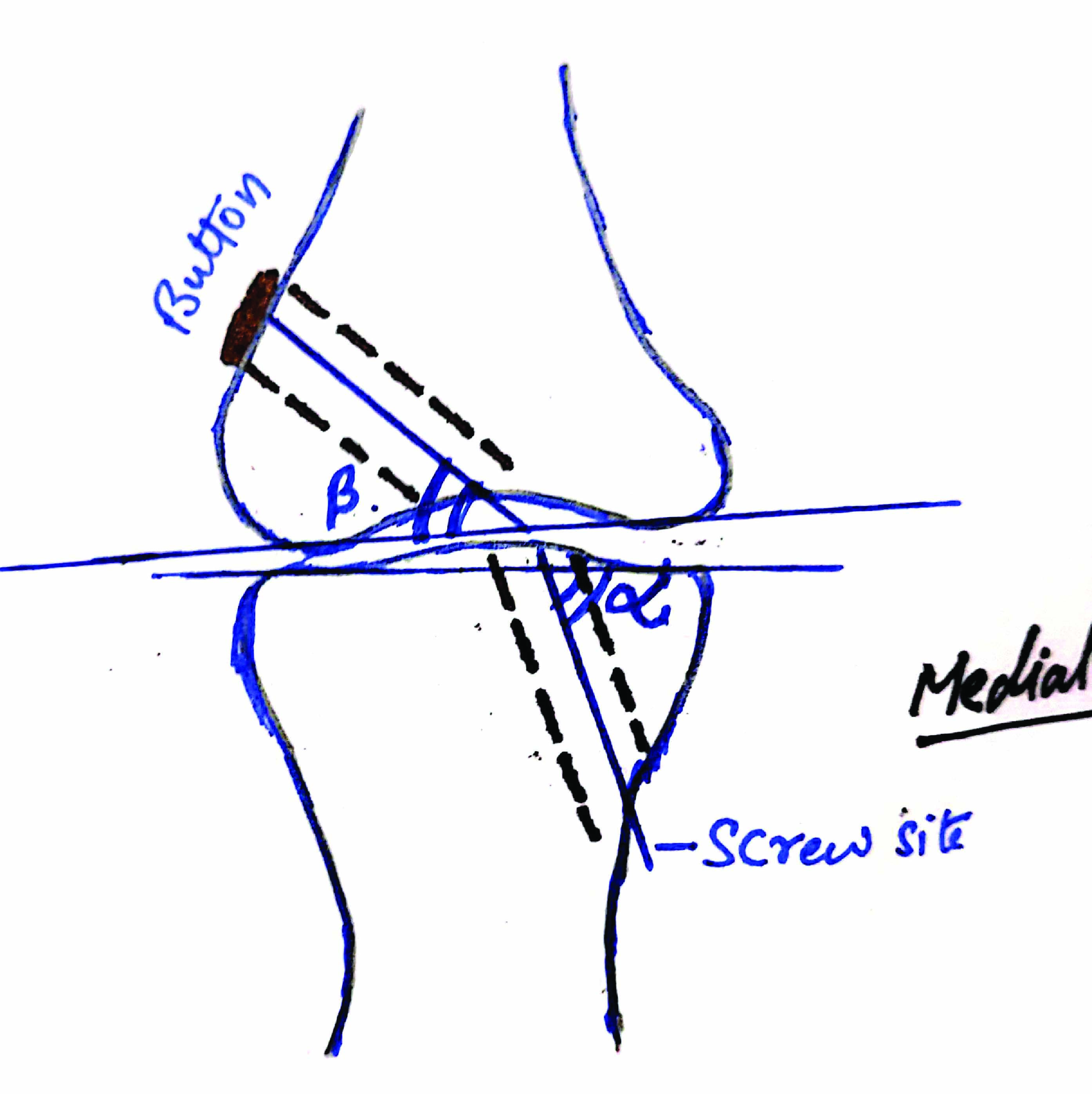
Sketch of knee joint with distal femur and proximal tibia showing illustration of method to measure tibial tunnel coronal angle (α) and femoral tunnel inclination (β).
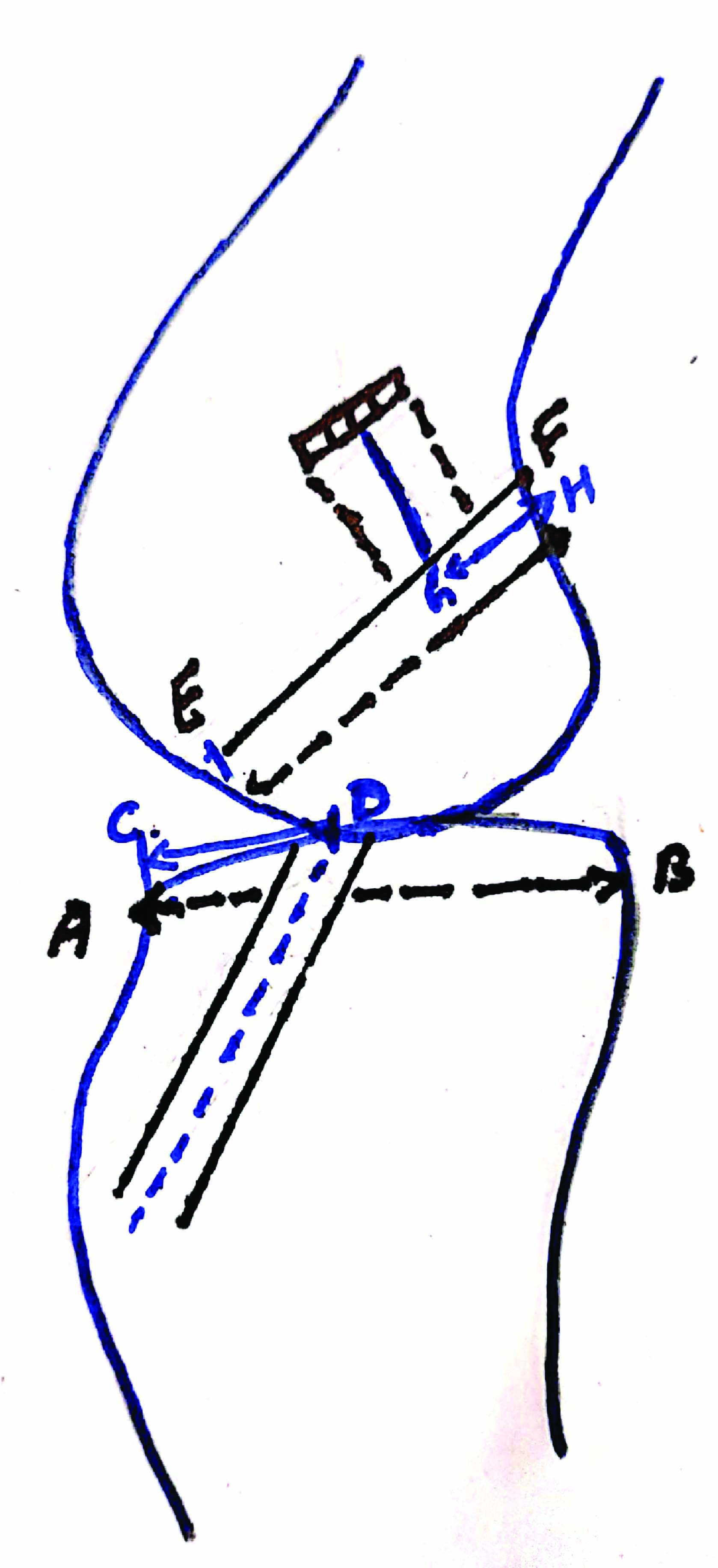
Sketch of knee joint with proximal tibia and distal femur lateral view showing the method to measure the distance of center of tibial tunnel from the anterior edge of the tibia (line CD) on lateral radiograph. Black line AB is the distance from the anterior border to the posterior border of the tibial plateau. Also, it shows measurement of the position of femoral tunnel from posterior. Black line EF represents the Blumensaat’s line. Line GH represents the distance from posterior cortex of the lateral femoral condyle to the center of the femoral tunnel.
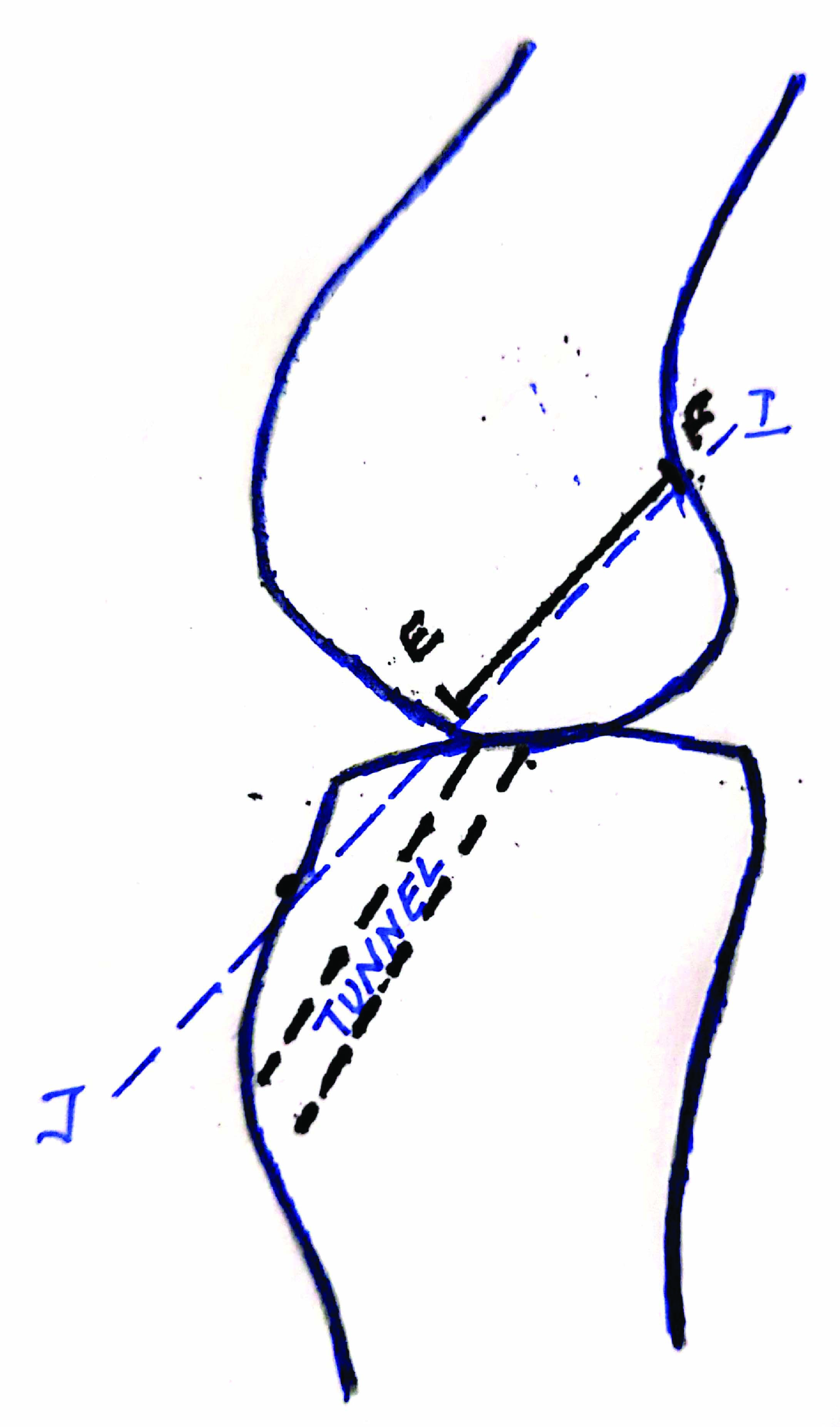
Sketch of knee joint with proximal tibia and distal femur showing method to measure graft impingement on lateral radiograph in full extension. (Images from left to right)
Measurements of tunnel shown on radiograph (AP and Lateral view).

Statistical Analysis
Coronal and sagittal tunnel position was the variables studied and were evaluated using Statistical Package for the Social Sciences (SPSS) software (Trial version). Student’s t-test was used for analysing the results. Two observers evaluated the data and cronbach alpha value was calculated as 0.8, proving no significant variability in radiographic measurements between observers.
Results
Out of total 50 patients, 48 (96%) were male and 2 (4%) were female. Mean age of the patients was 29.9 years [Table/Fig-6]. Most of the patients were operated within six months of injury (n=30, 60%). Rest of the patients were operated upon after six months of injury (n=20, 40%). On clinical examination, instability and swelling was found in all cases followed by pain in 96% of the patients [Table/Fig-7].
| Demographic parameters | Variables | n (%) |
|---|
| Gender | Male | 48 (96%) |
| Female | 2 (4%) |
| Age group (years) | <20 | 3 (6%) |
| 21-30 | 30 (60%) |
| 31-40 | 13 (26%) |
| 41-50 | 4 (8%) |
| Mode of injury | Sports Injury | 20 (40%) |
| Fall | 19 (38%) |
| RTA | 11 (22%) |
| Side of injury | Right | 32 (64%) |
| Left | 18 (36%) |
RTA: Road traffic accidents
| Clinical findings | No. of patients | Percentage (%) |
|---|
| Pain | 48 | 96 |
| Swelling | 50 | 100 |
| Instability | 50 | 100 |
| Locking | 0 | 0 |
| Joint line tenderness | 22 | 44 |
In the present study, the mean position of tibial tunnel in coronal plane was 45.48±2.55 from medial edge with 48 patients in range of 40-50%. Similarly average tibial tunnel angle in coronal plane was 69.46±7.57 degrees with only one patient having tibial tunnel >80 degrees (range 58-87). Coronal angle of femoral tunnel was 42.52±6.34 average with no patient having coronal femoral angle of >60 degrees. Position of femoral tunnel along Blumensaat’s line from posterior edge of femoral cortex was 35.19±6.09 (range being 21-50%) [Table/Fig-8].
Parameters of tunnel position.
| Parameters | Mean | SD |
|---|
| Coronal tibial tunnel position (%), from medial | 45.48 | 2.55 |
| Coronal Tibial Angle | 69.46 | 7.57 |
| Sagital tibial tunnel position (%), from anterior | 41.35 | 7.3 |
| Coronal femoral angle | 42.52 | 6.34 |
| Position of femoral tunnel On Blumensaat’s line (%), from posterior | 35.19 | 6.09 |
Graft impingement was not found in any of the case intraoperatively as well as postoperatively as analysed on x-rays, also no patient complained of extensor lag.
All the variables analysed by both the observers were evaluated using SPSS software (trial version) and the results of preoperative Lachman Test and postoperative Lachman test were statistically evaluated and the preoperative mean was 2.78±0.41 while the postoperative mean was 0.38±0.53 with significant p-value <0.001. Similarly the results of preoperative Pivot Shift Test (PST) and postoperative PST were statistically analysed. The results of lysholm score were statistically analysed using the unpaired t-test. The result was highly significant with p-value <0.001.
Lysholm score was also used to grade the patients, 88% (44 cases) in this series were excellent (≥95), 10% (5 cases) were good (93-84), 2% (1 case) fair (84-65) and no case was found with poor (<65) result. The mean preoperative subjective IKDC was 38.33±11.00. The mean postoperative subjective IKDC was 88.84±6.37. The results of IKDC score were statistically analysed using the unpaired t-test. The result was highly significant with p-value <0.001 [Table/Fig-9].
Functional outcome of patients (unpaired t-test used for evaluation of results).
| Parameters | Preoperative (Mean±SD) | Postoperative at minimum follow-up 12 months (Mean±SD) | p-value |
|---|
| Lysholm score | 42.26±13.73 | 96.04±4.35 | <0.001 |
| IKDC score | 38.33±11.00 | 88.84±6.37 | <0.001 |
| Lachman test | 2.78±0.41 | 0.38±0.53 | <0.001 |
| Pivot shift | 1.96±0.53 | 0.04±0.19 | <0.05 |
| Anterior drawer test | 1.3±0.05 | 0.17±0.04 | <0.05 |
On grading of IKDC score preoperatively, 1 (2%) cases were in group C (abnormal) and 49 (98%) cases were in group D (severely abnormal) and none of the cases were in group A (normal) or group B (nearly normal). Postoperatively 12 (24%) participants described their knees normal while 29 (58%) participants described their knees as nearly normal. Only 9 (18%) participants described their knees as abnormal and no patients described their knees as severely abnormal.
There were eight cases with tunnel position at more than 50% from anterior, as seen on lateral view with maximum being 56.33%. Only two cases out of these were associated with abnormal IKDC score. Two of the patients with IKDC score “severely abnormal” had femoral tunnel position in the average 50-60% on Blumensaat’s line from posterior. Other patients had good IKDC score as well as no loss of flexion and no graft tear after minimal follow up of one year.
Discussion
The goal of ACL reconstruction is to provide an isometric, anatomic, impingement free graft placement for injured ligament. Correct positioning of the tibial and femoral tunnels is one of the crucial points for achieving good results from ACL reconstruction [11]. Various studies have described the arthroscopic and anatomic landmarks for successful placements of femoral and tibial tunnels [12,13]. Studies have shown that incorrect positioning of tunnels in coronal and sagittal planes causes complications that modify the clinical results [5,8,14], as well as being the most common cause of lack of success in ACL reconstructions [Table/Fig-10] [8,15-17].
Comparison with previous studies [8,15-17].
| Authors | Year of study | Position of femoral tunnel On Blumensaat’s line (%), from posterior | Coronal femoral angle | Sagittal tibial tunnel position (%), from anterior | Coronal tibial angle | Coronal tibial tunnel position (%), from medial |
|---|
| Present study | | 35.19±6.09 | 42.52±6.34 | 41.35±7.3 | 69.46±7.57 | 45.48±2.55 |
| Khalfayan EE et al., [8] | 1996 | 29 (1 to 65) | --- | 26 (range 13 to 39) | ---- | 43 (range 35 to 50) |
| Nema SK et al., [15] | 2017 | 30.59±10.77 | 41.97±8.58 | 35.17±7.41 | 67.56±8.9 | 44.16±3.98 |
| Padua R et al., [16] | 2016 | 30±10 | 27±11 | 44±6 | 29.7±11.6 | --- |
| de Melo Silva Júnior O et al., [17] | 2015 | --- | 67.68 | --- | 64.81 | --- |
In present study the average position of femoral tunnel along the blumansaat’s line was 35.19±6.09% from posterior. Other studies have recommended placing femoral tunnels 20-40% from posterior aspect [14,18]. Good L et al., studied the radiological location of the native ACL in cadavers and observed that the ligament originates in femur at mean of 66% of anterior limit of Blumensaat’s line on lateral x-rays [19].
In the present study, coronal femoral angle had an average of 42.52±6.34 degrees. And none of the patient had angle more than 60 degrees. Various studies were suggestive of coronal femoral angle between 70-80 degrees associated with decreased flexion and impact against PCL [20,21]. Positioning that is more vertical in the coronal plane may cause graft to impact on the lateral part of the PCL, thus generating loss of flexion and also increased anterior weakness [22,23]. A femoral tunnel placed obliquely in coronal plane is most important for rotational stability of knee [24,25]. Biomechanical studies have shown that constructing femoral tunnel at an angle of 60 degrees in the coronal plane minimises the impact of the graft against PCL [20].
In the present study, the footprint of ACL was marked on femoral side with radiofrequency ablation, which helped us to guide the position of femoral tunnel. Also, an accessory anteromedial portal was made to create femoral tunnel with knee in 100-110 degrees flexion to create a less vertical tunnel.
The position of tibial tunnel in coronal plane in present study was 69.46±7.57. Studies have shown that a tunnel of more than 75 degrees is associated with increased tension and impingement on PCL [20,21]. It was observed that there were good results with tunnel upto 80 degrees. There were 5 patients (10%) with tibial tunnel ≥80 degrees associated with abnormal IKDC score (<85). To reduce the tension on the graft in the coronal plane it should be attempted to position the tibial tunnel at 60 degrees [21].
The tibial tunnel, if more anterior in the sagittal plane, can cause impingement on intercondyler roof, thereby limiting extension, joint effusion and anterior knee pain [22,26]. On the other hand, more posterior tibial tunnel placement is associated with loss of flexion and graft tear [27]. In this study, the position of tibial tunnel in sagittal plane was 41.35±7.3% from anterior edge of tibial plateau. The graft was positioned ≤50% from anterior in 84% cases.
Also, the tibial tunnel in AP radiograph should be slightly medial in the range of 35-50% from medial edge [13,27, 28]. In the present study, the average position of tibial tunnel when calculating from medial edge of tibial plateau was 45.48±2.55. In a recent study by de Paula Leite Cury R et al., it was concluded that this anteromedial position is best to avoid revision after ACL reconstruction [29]. Tunnel expansion also occurs after ACL reconstruction, which primarily occurs early at tunnel apertures [30].
Limitation(s)
Limitations of this study were that it was the short period study with one year follow-up and a small numbers of patients were included. Also, tunnel positions were not measured on 3D Computed Tomography (CT) scan. Also tunnel position may not be the only error associated with poor outcome, as other technical errors may also contribute to poor results like poor graft harvesting, improper tensioning and weak fixation to bone. It was a subjective study based on the Lysholm and IKDC scores and was not objectively based, as it required KT 1000 to quantify our results. Long term follow-up studies are required in future to know long term outcomes of this procedure.
Conclusion(s)
Correct positioning of tunnels is necessary for good functional outcome as proved by abnormal results in patients who had less accurate tunnel positioning. This was proved by good IKDC, Lysholm score, good subjective outcome in patients with a good tunnel position. The statistical analysis comparing the preoperative and postoperative anterior drawer test and PST were highly significant suggesting that ACL reconstruction with quadrupled hamstring autograft provides anterior and rotational stability. Also, ACL reconstruction with quadrupled hamstring filled with button with continuous loop on the femoral side and bio-interference screw in the tibial is a reliable, effective and reproducible technique.
RTA: Road traffic accidents