Introduction
The MecC Methicillin Resistant Staphylococcus aureus (MRSA) after its initial recovery in 2007 has been reported with varying frequency from different parts of the world. These isolates assume importance due to the fact that with routine testing platforms available for the detection of MRSA they can be misidentified as being methicillin sensitive which can adversely affect the treatment and outcome of infections due to MRSA harbouring the mecC gene.
Aim
To evaluate mecC gene carrying MRSA in clinical isolates.
Materials and Methods
This retrospective study was conducted in the Department of Microbiology, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India for a period of three months (May-July 2020). A total of 102 laboratory confirmed isolates of MRSA (based on biochemical tests and cefoxitin disc diffusion results) were subjected to screening for the presence of mecA and mecC gene by Polymerase Chain Reaction (PCR). Deoxyribonucleic Acid (DNA) was extracted using an in house extraction method following which mecA and mecC were amplified in a total reaction volume of 25 μL using 2x PCR master mix, 5 μL of template and 1 μL (0.4 μM final concentration) each of reverse and forward primers specific for the above mentioned genes. Statistical analysis was done using Statistical Package for the Social Sciences (SPSS) software v24.0.
Results
All the isolates were confirmed as being methicillin resistant with 96.1% isolates carrying the mecA gene and 3.9% carrying the mecC gene. The mecC MRSA were recovered from pus, swab and endotracheal tip in middle aged men. One of the patient from whose sample mecC MRSA was recovered was suffering from hypertension, diabetes and renal faliure. MRSA exhibited high resistance to all the antimicrobial agents tested however all of them were sensitive to vancomycin and linezolid.
Conclusion
The presence of mecC gene in clinical isolates of MRSA is a cause of concern and calls for an extensive and continuous surveillance of such isolates as they can in future be implicated in causing severe human infections.
Introduction
Staphylococcus aureus a versatile Gram positive pathogen endowed with the capacity to adapt to diverse environmental conditions is responsible for causing a multitude of illnesses in human beings that affect the blood stream, skin and soft tissues, respiratory tract as well as toxin mediated illnesses etc., [1]. The emergence and worldwide dissemination of Methicillin-Resistant S. aureus (MRSA) has posed a major challenge in the treatment of infections caused by this organism. Resistance to methicillin in S. aureus is conferred by the acquisition of one of several staphylococcal cassette chromosome mec (SCCmec) elements, carrying the mecA gene that codes for a penicillin-binding protein homologue (PBP2a) with reduced affinity for beta-lactam antibiotics [2]. In 2007, a novel mecA homologue, initially named mecA LGA251, encoded in a new SCCmec element designated type XI, having ccr type 8, divergent mecA regulatory genes (mecI and mecR), and no joining region J3, was reported from human and bovine MRSA isolates in UK and Denmark [3]. This mecA homologue; subsequently named as mecC in 2012, exhibited only 69% identity at the DNA level and 63% identity at the protein level to the previously described mecA/PBP2a. Its affinity towards oxacillin was shown to be four fold that of PBP2a [3].
The mecC MRSA isolates assume importance given the fact that PCR as well as antigen assays carried out to detect either PBP2a or its parent gene mecA fail to detect them and are thus misidentified as being methicillin sensitive. This can have adverse consequences in terms of patient management and MRSA surveillance. As regards the phenotypic Antimicrobial Susceptibility Testing (AST) methods, cefoxitin has been reported to be more reliable than oxacillin in identifying the mecC carrying MRSA isolates [4]. Automated methods like Vitek-2 were shown to detect only 11.3% of 62 mecC positive isolates as resistant to both cefoxitin and oxacillin, whereas it could detect 88.7% of strains with an oxacillin susceptible/cefoxitin resistant profile [5].
Although mecC MRSA, was recovered in 2007, a retrospective search for such isolates in UK and Denmark went on to prove their causative role in causing infections in animals and humans way before their formal discovery [3]. The Republic of Ireland described mecC in human MRSA strains in 2010 [6]. In Denmark the prevalence of mecC MRSA among all MRSA was found to be 1.9% in 2010 that increased to 2.8% in 2011 [7]. In Germany however the prevalence of mecC MRSA was found to be 0.06% with no significant change between 2004-05 and 2010-11 [8]. A study in England during 2011-2012, found the prevalence of mecC MRSA to be 0.45% [1], whereas screening of 565 S. aureus isolates collected between 2005 and 2011 in western Switzerland did not identify any mecC carrying MRSA isolates [9]. Recently, a study from Pakistan reported the isolation of mecC MRSA (3%) alone and in combination with mecA from human samples [10]. Data on the prevalence of mecC carrying MRSA isolates from India is scarce which could either be due to the low prevalence of this resistance mechanism and/or problems with methods employed for mecC detection. An Indian study carried out to find the virulence genes of S. aureus isolated from pork meat in retail outlets found that the prevalence of MRSA carrying mecA and mecC gene was 94.3 and 5.7%, respectively [11]. The present study was carried out with an aim to evaluate the existence of mecC in clinical isolates of S. aureus from a tertiary care centre in Northern India.
Materials and Methods
This retrospective study was conducted in the Department of Microbiology, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India for a period of three months from 1st May-31st July 2020 with the preliminary aim to screen isolates of S. aureus for the presence of mecC gene. The demographic data from July 2018-December 2019 was retrieved from the medical records section of the hospital whereas the microbiological data was taken from the patient registers maintained in the laboratory. The study did not involve any patients and hence under Helsinki guidelines was exempted from ethical clearance.
S.aureus isolates were preserved as a matter of routine and were revived by inoculating into nutrient broth which was incubated overnight. These were then subcultured onto blood and nutrient agar the next day. Out of a total of 182 isolates only 102 grew and were included in the study. The samples from which these isolates had been recovered initially included blood, pus and other body fluids and respiratory samples like sputum and Bronchoalveolar Lavage (BAL) fluid. The colonies on blood and nutrient agar were identified as S.aureus by their characteristic morphology, gram staining, catalase and tube coagulase test [12].
Susceptibility test of the isolates was done on Muller Hinton agar by Kirby Bauer disc diffusion method. Antibiotics used were penicillin G, vancomycin, linezolid, erythromycin, clindamycin, cotrimoxazole, ciprofloxacin, cefoxitin (as a surrogate marker for methicillin resistance) and amikacin. Minimum Inhibitory Concentration (MICs) for vancomycin were noted from Vitek-2. The zones of inhibition were measured and the results interpreted according to the guidelines of Clinical Laboratory Standard Institute (CLSI) 2020 [13].
Isolates resistant to cefoxitin were presumptively identified as MRSA and further confirmed by PCR amplification of mecA and/or mecC genes.
Polymerase Chain Reaction (PCR) for the Confirmation of mecC and mecA
A total of 102 retrospective laboratory confirmed isolates of MRSA, were subjected to screening for the presence of mecA and mecC gene by PCR [11,14].
DNA extraction: An in-house method of extraction of nucleic acid combined with spin-column extraction and purification method was used. In brief, 200 μL overnight Brain Heart Infusion (BHI) broth culture of S. aureus was transferred to 1.5 mL Eppendorf tubes and boiled in a water bath for 15 minutes. The samples were immediately chilled in ice for five minutes and subjected to high speed centrifuge at 10,000 × g for five minutes. For removal of protein contamination and purification of the bacterial DNA, the chilled lysates were again extracted with a commercial nucleic acid extraction kit in an automated nucleic acid extraction system (QIAcube HT system, QIAGEN, GmBH, Germany) as per manufacture’s protocol.
Amplification of mecA: Amplification of mecA was performed using forward primer sequence mecA-FP- AAAATCGATGGTAAAGGTTGGC and reverse primer sequence mecA-RP- AGTTCTGCAGTACCGGATTTGC, as described by Merlino J et al., [14]. PCR was performed as per the protocol described with minor modification with the following thermal cycling conditions: Initial denaturation at 95°C for 5 minutes followed by 35 cycles of amplification at 95°C for 30 seconds, 52°C for 60 seconds, 72°C for 60 seconds and final extension at 72°C for 10 minutes. PCR was performed in a total reaction volume of 25 μL using 2x PCR master mix (Promega, Madison, USA), 5 μL of template and 1 μL (0.4 μM final concentration) each of reverse and forward primers. PCR amplified a 533 bp fragment of the mecA specific for the PBP2 or PBP2a.
Amplification of mecC: For mecC, PCR amplification was performed using forward primer sequence mecC-FP- GAAAAAAAGGCTTAGAACGCCTC and reverse primer sequence mecC-RP- GAAGATCTTTTCCGTTTTCAGC as described previously [11]. PCR was performed in 25 μL using 5 μL of extracted DNA template, 2x PCR master mix, 1 μL of each forward and reverse primers (0.4 μM) with thermal cycling profile of initial denaturation at 95°C for 5 minutes followed by 35 cycles of amplification at 95°C for 30 seconds, 59°C for 60 seconds, 72°C for 60 seconds and final extension at 72°C for 10 minutes. PCR amplified a specific 138 bp fragment of mecC gene.
Control strains of S.aureus American Type Culture Collection (ATCC) 43300 for mecA positive and ATCC 25923 for mecA negative were used for quality control of all tests. Both mecA and mecC PCR amplified products were electrophoresed using 2% agarose gel in a horizontal electrophoresis system and visualised in a gel documentation imager (myECL imager, ThermoFisher Scientific, Waltham, USA).
Hospital record files for the 102 isolates were screened and parameters like age, gender, diagnosis at the time of admission, sample submitted, antibiotics received, duration of hospital stay and outcome in terms of death or discharge from the hospital were noted.
Statistical Analysis
Statistical analysis was done using SPSS software v24.0. The data was shown in the form of frequency and percentage.
Results
A total of 102 laboratory confirmed clinical isolates of MRSA that could be revived were a part of the present study. Demographic parameters, diagnosis at the time of hospital admission, duration of hospital stay, antibiotics received and outcome of the patients from whose samples MRSA were recovered is shown in [Table/Fig-1]. Out of these isolates of MRSA, mecA gene was found in 98 (96.1%) isolates whereas, mecC gene was found in 4 (3.9%) isolates as confirmed by PCR [Table/Fig-2].
Demographic profile and other parameters of the patients from whom MRSA were recovered.
| Demographic and clinical parameters | mecA Positive MRSA n=98 | mecC Positive MRSA n=4 |
|---|
| Age (years) |
| 0-20 | 2 (2.1%) | 0 |
| 21-40 | 31 (31.6%) | 2 (50%) |
| 41-60 | 36 (36.7%) | 2 (50%) |
| >60 | 29 (29.6%) | 0 |
| Gender |
| Males | 63 (64.3%) | 4 (100%) |
| Females | 35 (35.7%) | 0 |
| Diagnosis at the time of hospital admission |
| Gastrointestinal tract infection | 3 (3.1%) | 0 |
| Respiratory tract infection | 27 (27.5%) | 0 |
| Sepsis | 13 (13.3%) | 0 |
| Renal failure/Liver failure | 16 (16.3%) | 1 (25%) |
| Malignancy | 21 (21.4%) | 0 |
| Trauma | 18 (18.4%) | 3 (75%) |
| Duration of hospital stay |
| More than 10 days | 66 (67.3%) | 4 (100%) |
| Less than 10 days | 32 (32.7%) | 0 |
| Antibiotics received |
| Penicillins | 0 | 0 |
| Cepahalosporins | 34 (34.7%) | 0 |
| Penicillins+inhibitor combinations | 51 (52.0%) | 4 (100%) |
| Aminoglycosides | 48 (48.9%) | 4 (100%) |
| Tetracyclines | 12 (12.2%) | 0 |
| Carbapenems | 46 (46.9%) | 2 (50%) |
| Others | 21 (21.4%) | 0 |
| Outcome |
| Death | 2 (2.1%) | 0 |
| Discharged from the hospital | 96 (97.9%) | 4 (100%) |
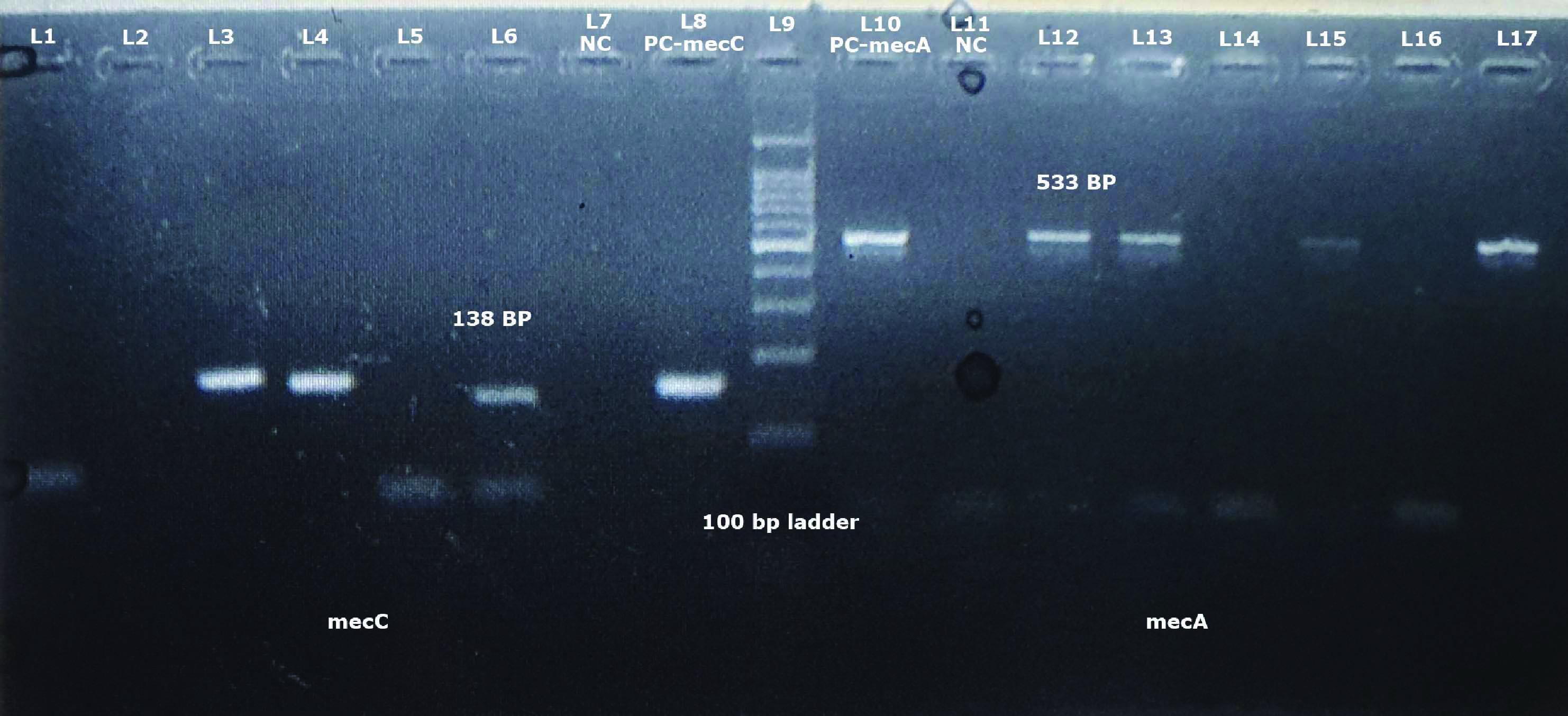
PCR confirmation of S. aureus isolates carrying the mecA and mecC genes. Lane 3, 4 and 6 are the mecC positive isolates (133bp) and lanes 12, 13, 15, 17 are representative mecA positive isolates (533bp). Lane 9 represents the 100 bp ladder, Lane 8 carries the positive control for mecC and Lane 10 carries the positive control of mecA. Lane 11 is negative control.
Two of the four mecC positive MRSA isolates were recovered from wound swabs that belonged to burn patients and one isolate was recovered from endotracheal tip of a patient of road traffic accident admitted in the Surgical Intensive Care Unit (SICU) of the hospital whereas one isolate was recovered from pus sample of a patient of chronic renal failure undergoing peritoneal dialysis. Samples from which MRSA isolates were recovered are shown in [Table/Fig-3]. All the mecC carrying MRSA were recovered from male patients in the age group of 30-49 years. Chronic renal failure patient (47-year-old male) was on peritoneal dialysis from the last five years and was suffering from hypertension and Type II diabetes mellitus. Rest of the patients did not have any co-morbidities. Road traffic accident patient was a 34-year-old male who was admitted in the SICU after undergoing surgery for his head injury. The other two patients were 39 and 42-year-old males with burn injuries to the face and chest and left thigh respectively.
Samples from which MRSA isolates were recovered.
| Location | mecA MRSA n=98 (96.1%) | mecC MRSA n=4 (3.9%) |
|---|
| Blood | 22 (22.4%) | - |
| Pus | 31 (31.6%) | 1 (25%) |
| Swab | 16 (16.4%) | 2 (50%) |
| Sputum | 8 (8.2%) | - |
| ET aspirate | 11 (11.2%) | 1 (25%) |
| Peritoneal fluid | 6 (6.1%) | - |
| CSF | 1 (1.0%) | - |
| Urine | 3 (3.1%) | - |
All the patients were discharged from the hospital after completion of their treatment. The antimicrobial resistance profile of all the MRSA isolates is shown in [Table/Fig-4]. All the isolates of MRSA were resistant to penicillin G and cefoxitin whereas none of the isolates were resistant to vancomycin and linezolid with variable susceptibility to other antibiotics as shown in [Table/Fig-4].
Antimicrobial resistance profile of MRSA isolates harbouring the mecA and mecC genes.
| Antibiotic agents | mecA Positive MRSA n=98 (96.1%) | mecC Positive MRSA n=4 (3.9%) |
|---|
| Penicillin G | 97 (99%) | 4 (100%) |
| Cefoxitin | 98 (100%) | 4 (100%) |
| Erythromycin | 83 (84.7%) | 1 (25%) |
| Clindamycin | 69 (70.4%) | 0 |
| Vancomycin | 0 | 0 |
| Linezolid | 0 | 0 |
| Ciprofloxacin | 86 (87.8%) | 1 (25%) |
| Amikacin | 64 (65.3%) | 0 |
| Cotrimoxazole | 77 (78.6%) | 0 |
Discussion
In this study, the authors report for the first time the presence of mecC gene (3.9%) in clinical isolates of MRSA recovered from a tertiary care hospital in Jammu and Kashmir, India. The results of this study were in accordance with those reported by Khan AA et al., wherein 3% of MRSA isolates were found to harbour mecC gene [10]. The percentage of mecC MRSA that was seen in this study was however slightly more than what has been reported from various European countries so far i.e., 0.45% in England, 0.06% in Germany and 2.8% in Denmark [1,6-8]. The total number of MRSA isolates was less in the present study which could have resulted in the higher percentage of mecC MRSA compared to a recent meta-analysis where the prevalence of mecC MRSA in human subgroup was estimated to be 0.004% only [15]. The mecC positive MRSA isolates have been identified from different hosts across the globe with varying frequency, with most of the human case reports being described from European subcontinent, a fact that can be attributed to a robust surveillance system for the recovery of such strains [16]. In most of the case reports, mecC MRSA were recovered from skin and soft tissue infections [17-20]. Apart from these, mecC MRSA have also been recovered from blood, urine and sputum, albeit in small numbers [16]. In this study also, all the mecC positive MRSA isolates were recovered from pus and body fluids of patients. Two isolates were from swabs, one from ET tube and one from pus.
The patients in this study from whom mecC MRSA were isolated were middle aged men (30-49 years). Most of the patients described in earlier case reports were also middle-aged or elderly [6,9,17,19,20-23] except two patients: one of whom was a 34-year-old farm worker with a history of contact with animals [20], and the other a three-year-old child [17]. MRSA isolates were recovered more from male patients in a study from Pakistan with dominant age group of 18-35 years [10]. The average age of patients with mecC MRSA in Denmark during 2007-11 was 51 years [7] whereas in Sweden in 2005-14 it was 60 years [18].
Most of the patients in the Swedish study had some kind of underlying co-morbidity or an existing skin lesion [18]. In a study from Austria, mecC MRSA infections were identified in patients with primary pathologies like diabetes mellitus, myelodysplastic syndrome, peripheral arterial occlusion disease etc., [24]. Likewise in Spain mecC MRSA was recovered from the blood sample of a patient with urothelial carcinoma [25]. In the present study, only one patient had diabetes mellitus and hypertension. He was suffering from chronic renal failure and undergoing dialysis for the same.
All the mecC MRSA isolates in this study were resistant to penicillin G and cefoxitin whereas one isolate was resistant to ciprofloxacin and erythromycin each. However, the number of these isolates was too small to deduce any statistical significance. The mecA MRSA isolates on the other hand showed high level resistance to all the antimicrobial agents tested. All S. aureus isolates were uniformly sensitive to vancomycin and linezolid. Most of the mecC MRSA isolates recovered form humans have shown good susceptibility for non beta-lactam antibiotics even though resistance to these antimicrobial agents has been reported in various studies [16]. Fluoroquinolone resistance was detected in two isolates in Germany [26] and in one isolate in Denmark [7] whereas macrolide and lincosamide resistance was detected in UK [27] and Sweden [18]. Norfloxacin resistance encoded by the sdrM gene and tetracycline resistance due to tet efflux was identified in one and two mecC MRSA CC130 isolates, respectively in Ireland [6,28].
Even though the origin of mecC MRSA is unclear, the mecC gene has also been detected in Staphylococcus stepanovicii, Staphylococcus xylosus and Staphylococcus sciuri suggesting that coagulase negative staphylococci could be the source of this resistance gene as was suggested for mecA [29]. The clinical microbiology laboratories should therefore be aware not only of mecC MRSA but of the possible occurrence of mecC in CONS as well. The mecC MRSA represents a relatively new form of MRSA that can colonise and cause severe fatal disease in human beings as well as wide range of other host species. For the confirmation of MRSA, molecular detection of either mecA by PCR or of PBP2a/PBP2′, by antibody detection test using slide agglutination assays is considered as the gold standard [30]. Clinical laboratories using cefoxitin while performing antimicrobial susceptibility tests by disc diffusion or broth/agar dilution tests for MRSA will correctly identify strains carrying the mecC gene. However, problem is where either PCR targeting mecA or slide agglutination assays for mecA-encoded PBP2a are used to identify or confirm MRSA. They will misidentify mecC MRSA as being methicillin sensitive. The laboratories thus need to incorporate universal mec gene primers that are able to amplify both mecA and mecC or use mecC specific primers when looking for such strains.
Limitation(s)
The study was limited by its small number of mecC MRSA isolates, which made the comparison of various demographic and clinical parameters difficult. Differences in methodology in the studies conducted so far worldwide complicates the understanding of the true magnitude of the problem posed by mecC MRSA. Furthermore in the present study a detailed analysis of mecC MRSA isolates to delineate the clonal complexes they belong to is missing. This can better our understanding of their origin, nature and evolution in this part of the world.
Conclusion(s)
This was a first formal study that confirms the presence of mecC MRSA (3.9%) among human isolates in India. The data provides a baseline for future study and surveillance of these microorganisms. Even though the number of human mecC MRSA infections is low, continuous monitoring of these isolates is highly warranted given the great potential of transmissibility among different hosts which could increase the number of infection in humans due to mecC MRSA.
[1]. Paterson GK, Morgan FJE, Harrison EM, Cartwright EJP, Török ME, Zadoks RN, Prevalence and characterization of human mecC methicillin-resistant Staphylococcus aureus isolates in EnglandJ Antimicrob Chemother 2014 69:907-10.10.1093/jac/dkt46224284779 [Google Scholar] [CrossRef] [PubMed]
[2]. Ito T, Hiramatsu K, Tomasz A, Lencastre H, Perreten V, Holden MTG, Guidelines for reporting novel mecA gene homologuesAntimicrob Agents Chemother 2012 56:4997-99.10.1128/AAC.01199-1222869575 [Google Scholar] [CrossRef] [PubMed]
[3]. Garcia-Alvarez L, Holden MTG, Lindsay H, Webb CR, Brown DFJ, Curran MD, Meticillin-resistant Staphylococcus aureus with a novel mecA homologue in human and bovine populations in the UK and Denmark: A descriptive studyLancet Infect Dis 2011 11:595-603.10.1016/S1473-3099(11)70126-8 [Google Scholar] [CrossRef]
[4]. Skov R, Larsen AR, Kearns A, Holmes M, Teale C, Edwards G, Phenotypic detection of mecC-MRSA: Cefoxitin is more reliable than oxacillinJ Antimicrob Chemother 2014 69:133-35.https://doi.org/10.1093/jac/dkt34110.1093/jac/dkt34124038776 [Google Scholar] [CrossRef] [PubMed]
[5]. Cartwright EJP, Paterson GK, Raven KE, Harrison EM, Gouliouris T, Kearns A, Use of Vitek 2 antimicrobial susceptibility profile to identify mecC in methicillin-resistant Staphylococcus aureusJ Clin Microbiol 2013 51:2732-34.https://doi.org/10.1128/JCM.00847-1310.1128/JCM.00847-1323720794 [Google Scholar] [CrossRef] [PubMed]
[6]. Shore AC, Deasy EC, Slickers P, Brennan G, O’Connell B, Monecke S, Detection of staphylococcal cassette chromosome mec type XI carrying highly divergent mecA, mecI, mecR1, blaZ, and ccr genes in human clinical isolates of clonal complex 130 methicillin-resistant S. aureusAntimicrob Agents Chemother 2011 55:3765-73.10.1128/AAC.00187-11 [Google Scholar] [CrossRef]
[7]. Petersen A, Stegger M, Heltberg O, Christensen J, Zeuthen A, Knudsen LK, Epidemiology of methicillin-resistant Staphylococcus aureus carrying the novel mecC gene in Denmark corroborates a zoonotic reservoir with transmission to humansClin Microbiol Infect 2013 19:16-22.10.1111/1469-0691.1203623078039 [Google Scholar] [CrossRef] [PubMed]
[8]. Schaumburg F, Köck R, Mellmann A, Richter L, Hasenberg F, Kriegeskorte A, Population dynamics among methicillin-resistant Staphylococcus aureus isolates in Germany during a 6-year periodJ Clin Microbiol 2012 50:3186-92.10.1128/JCM.01174-1222814464 [Google Scholar] [CrossRef] [PubMed]
[9]. Basset P, Prod’hom G, Senn L, Greub G, Blanc DS, Very low prevalence of meticillin-resistant Staphylococcus aureus carrying the mecC gene in western SwitzerlandJ Hosp Infect 2013 83:257-59.10.1016/j.jhin.2012.12.00423384824 [Google Scholar] [CrossRef] [PubMed]
[10]. Khan AA, Alia A, Tharmalingamb N, Mylonakis E, Zahra R, First report of mecC gene in clinical methicillin resistant S. aureus (MRSA) from tertiary care hospital Islamabad, PakistanJournal of Infection and Public Health 2020 13:1501-07.10.1016/j.jiph.2020.05.01732517997 [Google Scholar] [CrossRef] [PubMed]
[11]. Savariraj WR, Ravindran NB, Kannan P, Paramasivam R, Senthilkumar TMA, Kumarasamy P, Prevalence, antimicrobial susceptibility and virulence genes of Staphylococcus aureus isolated from pork meat in retail outlets in IndiaJ Food Saf 2018 2018:e1258910.1111/jfs.12589 [Google Scholar] [CrossRef]
[12]. Koneman EW, Allen SD, Janda WM, Schreckenberger PC, Winn WC Jr, Staphylococcus aureusIn: Colour Atlas and Textbook of the Diagnostic Microbiology 2017 7 ednLippincott Williams and Wilkins:670-719. [Google Scholar]
[13]. Performance Standards for Antimicrobial Susceptibility Testing. 30th ed. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute. 2020 [Google Scholar]
[14]. Merlino J, Watson J, Rose B, Pegler BM, Gottlieb T, Bradbury R, Detection and expression of methicillin/oxacillin resistance in multidrug-resistant and non multidrug-resistant Staphylococcus aureus in Central Sydney, AustraliaJ Antimicrob Chemother 2002 49:793-901.10.1093/jac/dkf02112003973 [Google Scholar] [CrossRef] [PubMed]
[15]. Diaz R, Ramalheira E, Afreixo V, Gago B, Methicillin-resistant Staphylococcus aureus carrying the new mecC gene–A meta-analysisDiagn Microbiol Infect Dis 2016 84:135-40.10.1016/j.diagmicrobio.2015.10.01426652130 [Google Scholar] [CrossRef] [PubMed]
[16]. Lozano C, Fernández R, Ruiz-Ripa L, Gómez P, Zarazaga M, Torres C, Human mecC-Carrying MRSA: Clinical implications and risk factorsMicroorganisms 2020 10.3390/microorganisms810161533092294 [Google Scholar] [CrossRef] [PubMed]
[17]. García-Garrote F, Cercenado E, Marín M, Bal M, Trincado P, Corredoira J, Methicillin-resistant Staphylococcus aureus carrying the mecC gene: Emergence in Spain and report of a fatal case of bacteraemiaJ. Antimicrob Chemother 2014 69:45-50.10.1093/jac/dkt32723975743 [Google Scholar] [CrossRef] [PubMed]
[18]. Lindgren AK, Gustafsson E, Petersson AC, Melander E, Methicillin-resistant Staphylococcus aureus with mecC: A description of 45 human cases in southern SwedenEur J Clin Microbiol Infect Dis 2016 35:971-75.10.1007/s10096-016-2624-x27010813 [Google Scholar] [CrossRef] [PubMed]
[19]. García MEC, Cimiano IM, Encinas PM, Álvarez CO, Methicillin-resistant Staphylococcus aureus carrying the mecC gene in a patient with a wound infectionEnferm Infecc Microbiol Clin 2015 33:287-88.10.1016/j.eimc.2014.06.01125200213 [Google Scholar] [CrossRef] [PubMed]
[20]. Benito D, Gómez P, Aspiroz C, Zarazaga M, Lozano C, Torres C, Molecular characterization of Staphylococcus aureus isolated from humans related to a livestock farm in Spain, with detection of MRSA-CC130 carrying mecC gene: A zoonotic case?Enferm Infecc Microbiol Clin 2016 34:280-85.10.1016/j.eimc.2015.03.00825976751 [Google Scholar] [CrossRef] [PubMed]
[21]. Dermota U, Zdovc I, Strumbelj I, Kosnik IG, Ribic H, Rupnik M, Detection of methicillin-resistant Staphylococcus aureus carrying the mecC gene in, human samples in SloveniaEpidemiol Infect 2015 143:1105-08.10.1017/S095026881400186125036113 [Google Scholar] [CrossRef] [PubMed]
[22]. Laurent F, Chardon H, Haenni M, Michele Bes, Reverdy ME, Madec JY, MRSA harboring mecA variant gene mecC, FranceEmerg Infect Dis 2012 18:1465-67.10.3201/eid1809.11192022932400 [Google Scholar] [CrossRef] [PubMed]
[23]. Barraud O, Laurent F, François B, Bes M, Vignon P, Ploy MC, Severe human bone infection due to methicillin-resistant Staphylococcus aureus carrying the novel mecC variantJ Antimicrob Chemother 2013 68:2949-50.10.1093/jac/dkt27423833187 [Google Scholar] [CrossRef] [PubMed]
[24]. Kerschner H, Harrison EM, Hartl R, Holmes MA, Apfalter P, First report of mecC MRSA in human samples from Austria: Molecular characteristics and clinical dataNew Microbes New Infect 2014 3:04-09.10.1016/j.nmni.2014.11.00125755883 [Google Scholar] [CrossRef] [PubMed]
[25]. Romero-Gómez MP, Mora-Rillo M, Lazaro-Perona F, Gómez-Gil MR, Mingorance J, Bacteraemia due to meticillin-resistant Staphylococcus aureus carrying the mecC gene in a patient with urothelial carcinomaJ Med Microbiol 2013 62:1914-16.10.1099/jmm.0.064683-024072763 [Google Scholar] [CrossRef] [PubMed]
[26]. Cuny C, Layer F, Strommenger B, Witte W, Rare occurrence of methicillin-resistant Staphylococcus aureus CC130 with a novel mecA homologue in humans in GermanyPLoS ONE 2011 6:e2436010.1371/journal.pone.002436021931689 [Google Scholar] [CrossRef] [PubMed]
[27]. Harrison EM, Coll F, Toleman MS, Blane B, Brown NB, Török ME, Genomic surveillance reveals low prevalence of livestock-associated methicillin-resistant Staphylococcus aureus in the East of EnglandSci Rep 2017 7:740610.1038/s41598-017-07662-228785112 [Google Scholar] [CrossRef] [PubMed]
[28]. Kinnevey PM, Shore AC, Brennan GI, Sullivan DJ, Ehricht R, Monecke S, Extensive genetic diversity identified among sporadic methicillin-resistant Staphylococcus aureus isolates recovered in Irish hospitals between 2000 and 2012Antimicrob Agents Chemother 2014 58:1907-17.10.1128/AAC.02653-1324395241 [Google Scholar] [CrossRef] [PubMed]
[29]. Lakhundi S, Zhang K, Methicillin-resistant Staphylococcus aureus: Molecular characterization, evolution, and epidemiologyClin Microbiol Rev 2018 31:e00020-18.10.1128/CMR.00020-1830209034 [Google Scholar] [CrossRef] [PubMed]
[30]. Paterson GK, Harrison EM, Holmes MA, The emergence of mecC methicillin-resistant Staphylococcus aureusTrends Microbiol 2014 22(1):42-47.10.1016/j.tim.2013.11.00324331435 [Google Scholar] [CrossRef] [PubMed]