Introduction
Thrombocytopenia has been known to be a manifestation as well as predictor of severe dengue. However, use of additional biomarkers like Aspartate Aminotransferase (AST)/Alanine Aminotransferase (ALT) alone or in conjunction with platelet count may help in early and better predictability of severe dengue cases.
Aim
To determine the correlation between transaminase elevation and severity of dengue fever.
Materials and Methods
This was a single centre, cross-sectional study conducted at a tertiary care centre of Western Maharashtra. Total 110 hospitalised patients with a diagnosis of suspected dengue fever, based on clinical signs and symptoms with a positive NS1 antigen test (non structural protein 1)/Immunoglobulin M (IgM) test using rapid test kits were taken as study population. The patients were clinically evaluated on daily basis for development of any warning signs and symptoms along with monitoring of haematological and biochemical parameters. For statistical analysis the technique of percentages, mean and Pearson ‘r’s were employed using IBM Statistical Package for the Social Sciences (SPSS 20.0) version for windows. The p-value of 0.05 was considered as significant value.
Results
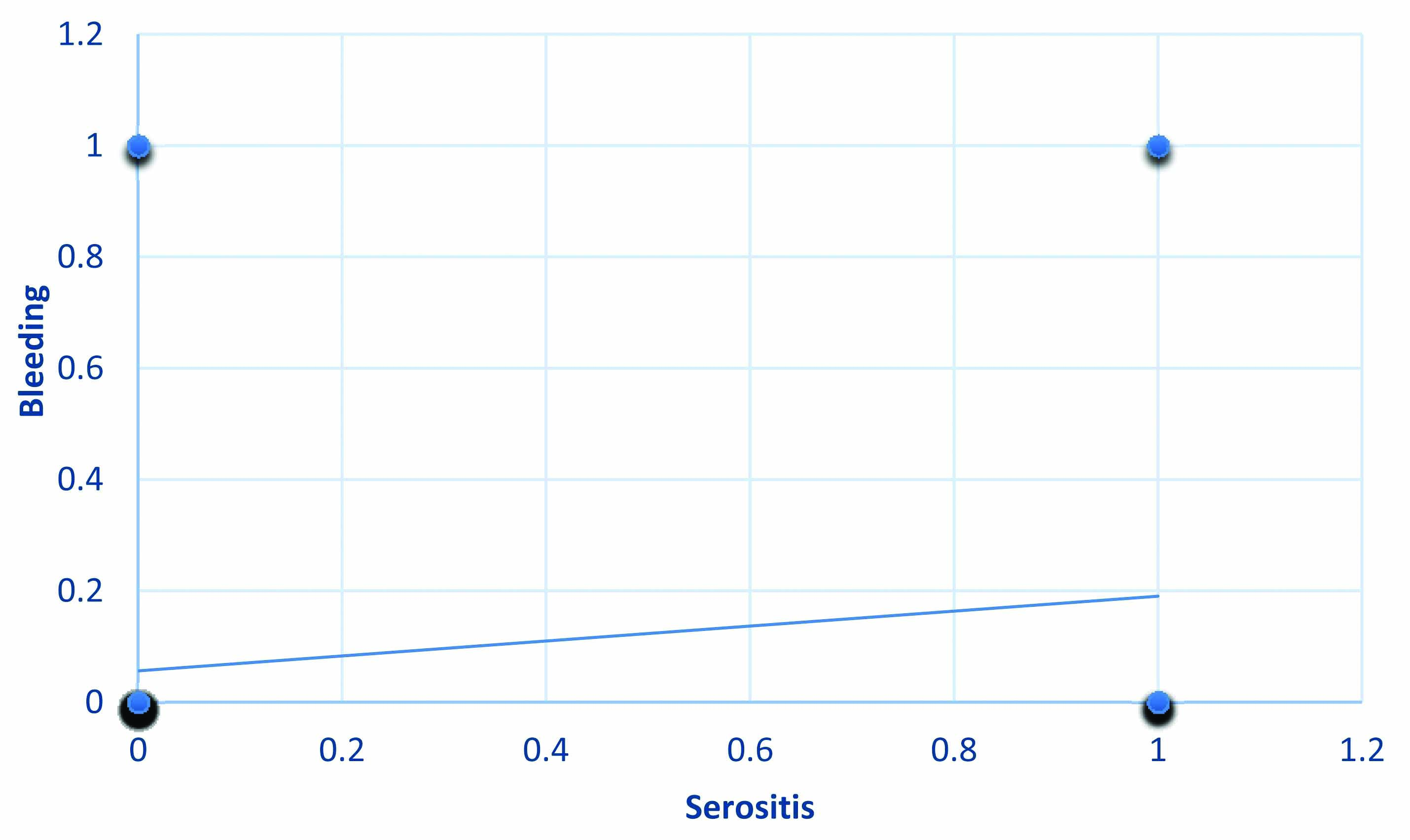
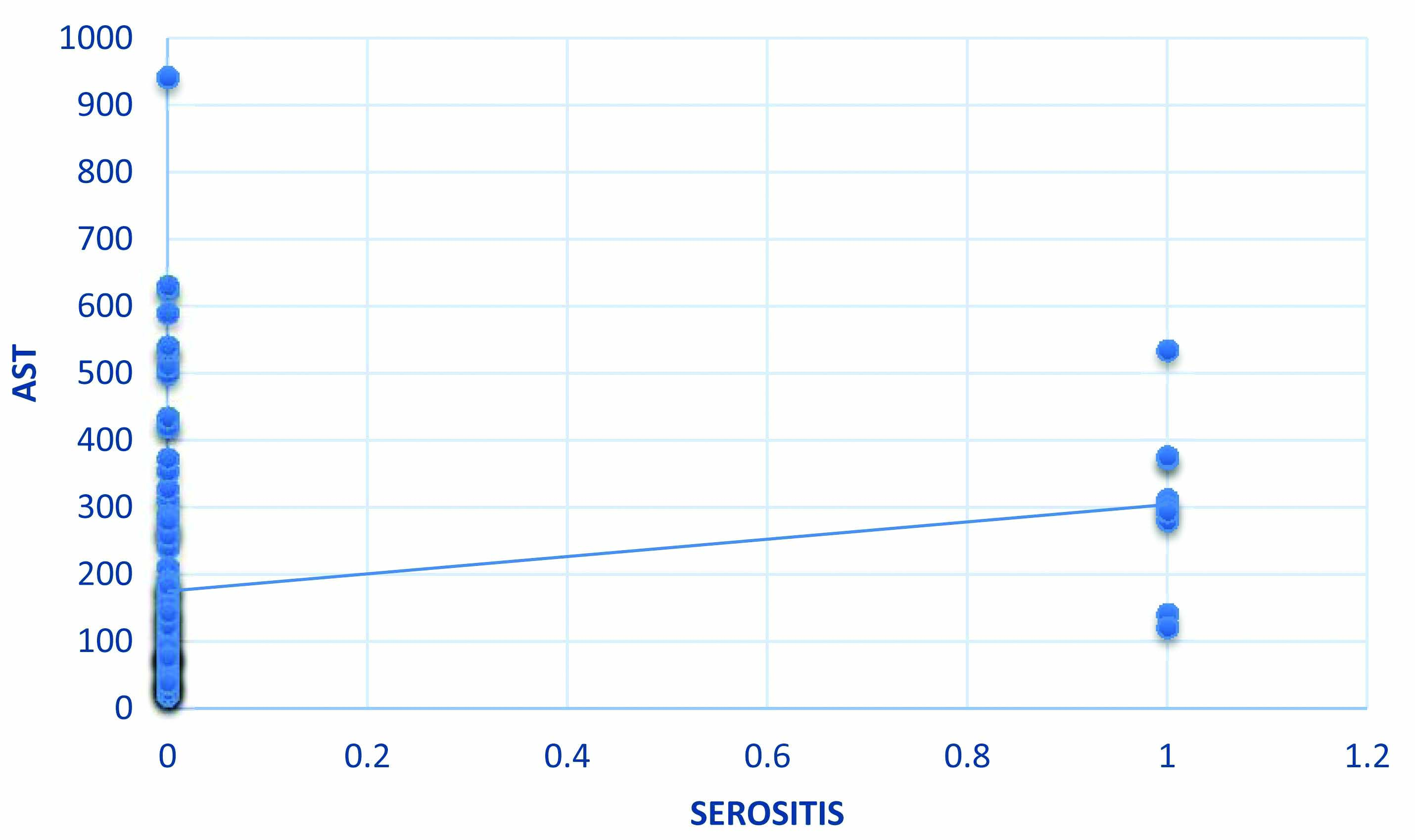
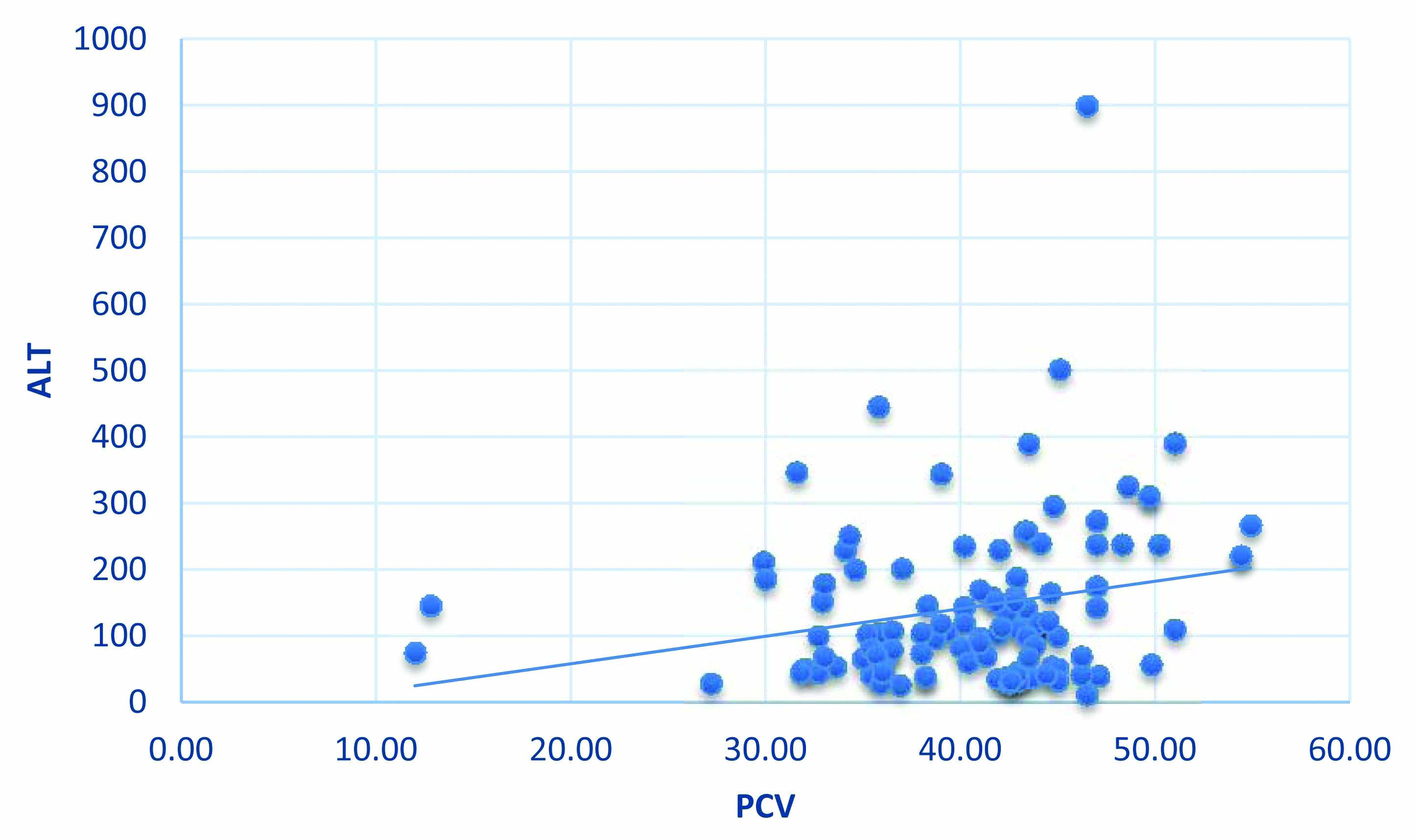
Out of 110 patients, 83 were males and 27 females. Clinical fluid accumulation was seen in 5 patients (4.5%), bleeding manifestations and fluid accumulation in 4 (3.6%) and bleeding manifestations in 17 (15.5%). Negative correlation was observed between thrombocytopenia with bleeding manifestations (r=-0.17, p=0.04), whereas positive correlation was seen in incidence of bleeding with serositis (r=0.19, p=0.04), AST with serositis (r=0.21, p=0.02) and ALT with Packed Cell Volume (PCV) (r=0.22, p=0.01).
Conclusion
Additional biomarkers like AST and ALT alone or in conjunction with platelet count can also help in early prediction of severity of dengue fever.
Severe dengue, Serositis, Thrombocytopenia, Transaminase elevation
Introduction
Dengue, caused by a flavivirus, is a tropical disease spread by the vector Aedes aegypti and Aedes albopictus. The etiological agent is a single stranded RNA virus of 30 nm diameter [1]. It is endemic in tropical regions where conditions for viral replication and transmission are ideal.
In the pathogenesis of dengue fever, both cell and antibody mediated immunity have an important role. The cell mediated immunity is the basis for the so called original antigenic sin hypothesis [2], which describes a skewed immune response to subsequent infection with different serotypes, resulting in severe disease.
The abnormalities in homeostasis seen in severe dengue include vasculopathy [3], thrombopathy, coagulopathy [4] and bone marrow changes. These bone marrow changes range from mild and transient suppression to dengue induced Hemophagocytic Lymphohistiocytosis (HLH) [5], dengue induced aplastic anaemia [6] and dengue related myelofibrosis [7].
The disease is clinically characterised by fever, myalgia, joint pain, mucosal bleed, clinical fluid accumulation and as already discussed, thrombocytopenia. Third space fluid loss and bleeding manifestations may cause serious complications or death [8]. The rate of fall of platelets has been linked to various serious manifestations in dengue such as (including but not limited to) acute respiratory distress syndrome, dengue encephalitis and dengue related acute liver failure. The utility of monitoring the patient for warning signs has been corroborated by multiple studies and consensus statements [9]. As a result of the same, platelet monitoring has been extensively used in dengue fever management across the globe. The same serves as basis for both diagnostic (fever with thrombocytopenia is a clinical clue for possibility of dengue fever) and therapeutic intervention (Component support therapy).
In 2016, an attempt was made to develop a risk score for severe dengue based on the above mentioned parameters for disease prognosis and identification of patients at risk for severe dengue in the course of illness [10].
The course of dengue fever is characterised not only by alteration in haematological parameters (thrombocytopenia, leucopenia, haemoconcentration) but also includes biochemical alterations in form on early liver injury manifested by transaminase elevation [11]. The trend of transaminase elevation is usually characterised by AST/ALT ratio >1 [12]. The pattern is contrary to the one seen in viral hepatitis which is characterised by predominant ALT elevations (ALT/AST >1) as ALT is specific marker for hepatocyte injury. AST on the other hand has multiple sources (Red blood cells, monocytes, hepatocytes etc.,). This typical pattern can aid in differentiating dengue related liver injury from that of viral hepatitis [13]. The liver injury can have varied manifestations ranging from asymptomatic transaminase elevation to acute liver failure. The spectrum of these manifestations may be altered by use of hepatotoxic NSAIDs during the febrile phase of dengue fever, pre-existing liver disease or co-infection with hepatotropic viruses [14]. The occurrence of transaminase elevation and its correlation with worse outcome has been evaluated in the past, wherein higher AST/ALT ratio was not only related with poor outcome but also helped in predicting early complication and higher incidence of plasma leakage in conjunction with thrombocytopenia [15].
In this study, an attempt has been made to study the role of altered liver parameters like AST/ALT apart from routinely used platelet count in predicting the severity of dengue. The current study also aimed at understanding any existing intrinsic correlation between haematological and biochemical parameters used to define dengue severity. A positive correlation between these elements can help in predicting the onset of shock, third space fluid loss which may further facilitate prognostication and early intervention rather than depending on platelet count which usually follows the trend of white blood cells, has nadir value during the critical phase where in high chances of landing in shock or multiorgan dysfunction syndrome may be present.
Materials and Methods
This single centre, cross-sectional study was conducted at a tertiary care centre of Armed Forces Medical College, Pune, Maharashtra, India from March 2019 to October 2019. Institutional Ethical Committee approval was taken (IEC/2018/169) prior to conduct of the study.
Inclusion criteria: A total of 110 hospitalised patients with a diagnosis of suspected dengue fever, based on clinical signs and symptoms with a positive NS1 antigen test/IgM test using rapid test kits were taken as study population.
Exclusion criteria: Patients with dual infections (dengue and malaria) and the recently described triple infection (dengue, malaria and scrub typhus) were excluded as these are likely to cause an independent and confounding rise in transaminases. Patients with a previously diagnosed cause of low platelets (immune thrombocytopenia, haematological malignancies, aplastic anaemia) were also excluded due to obvious confounding.
Study Procedure
The profile of warning signs and associated clinical manifestations (common symptoms) were studied. The haematological and biochemical alterations were studied during the course of hospitalisation along with onset of either of the warning signs, namely, clinical fluid accumulation (ascites, pleural effusion or pedal oedema) and mucosal bleed (clinically detected wet or dry petechiae or purpura).
The patients were clinically evaluated for development of any warning signs and symptoms and were monitored for haematological and biochemical parameters. The monitoring of complete blood count and biochemical parameters were done on daily basis apart from sampling on the day of admission, which served as baseline parameters for platelet count, Haematocrit (HCT) and AST/ALT levels during the course of hospitalisation. Platelet count was evaluated using five-part differential auto haematology analyser along with correlation with manual platelet count on peripheral blood smear. The platelet count reported on the peripheral blood smear was utilised to record nadir platelet count in order to prevent false reporting as anticipated with five-part differential in cases of platelet clumping. Pleural effusion was assessed using a chest radiograph (on clinical suspicion of effusion) along with daily clinical examination to look for effusion and baseline chest radiograph on admission. Similarly, ascites was assessed through clinical examination on daily basis and confirmed by abdominal ultrasound. The individuals during the evaluation of transaminase elevation were subjected to abdominal ultrasound and serositis, if any during the same examination was also documented for clinical fluid accumulation.
The individuals with dengue fever were divided into three groups as per the presence/ absence of warning signs and symptoms (dengue with no warning signs and symptoms, dengue with warning signs and symptoms, and severe dengue). Severity of dengue was defined as per the World Health Organisation (WHO) 2009 guidelines [12] wherein severe dengue was defined as one or more of the following: (i) plasma leakage that may lead to shock (dengue shock) and/or fluid accumulation, with or without respiratory distress, and/or; (ii) severe bleeding, and/or; (iii) severe organ impairment. Warning signs include abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleed, lethargy, restlessness, liver enlargement >2 cm and the laboratory parameters include increase in HCT concurrent with rapid decrease in platelet count. Every patient received treatment according to the existing standards of care during the course of hospitalisation.
Statistical Analysis
For statistical analysis the technique of percentages, mean and Pearson ‘r’s were employed using IBM Statistical Package for the Social Sciences (SPSS 20.0) version for windows. The variables, bleeding manifestation and serositis were classified into two categories which were thought of as concentrated at two distinct points along a graduated scale or continuum. A score of ‘1’ was assigned to subjects having the incidence of bleeding manifestations or serositis whereas a score of ‘0’ was assigned to subjects having no incidence of bleeding manifestations or serositis. Subsequently, Pearson ‘r’s were computed for studying the relationship of these variables with other variables. The p-value of 0.05 was considered as significant value.
Results
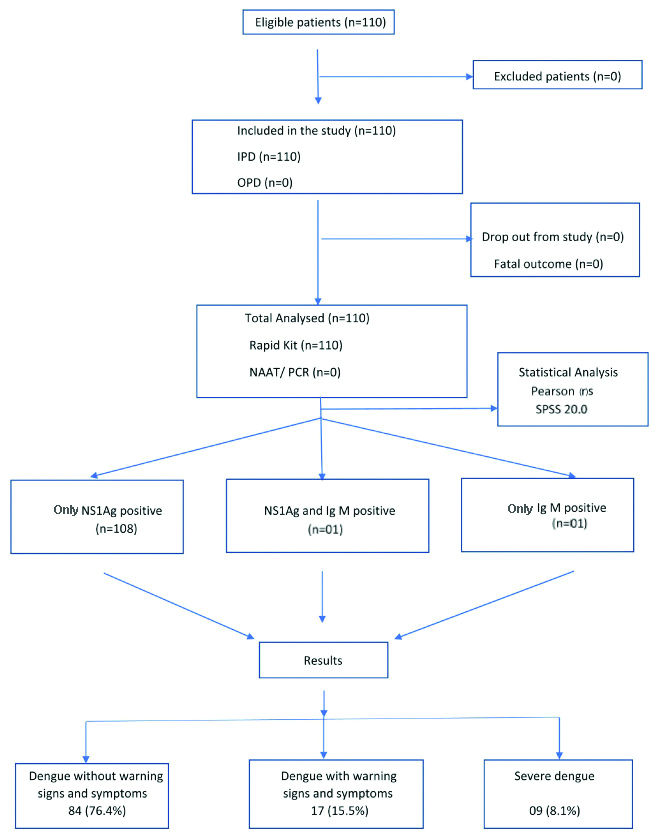
Out of the enrolled population, 83 were males and 27 females; with majority cases in the age group of 31-40 years in both the genders [Table/Fig-1]. There were 108 individuals who had only NS1Ag positive status. One individual had only Ig M positive status, while one individual had both NS1Ag as well as Ig M positive status [Table/Fig-2]. Majority of the individuals were admitted to this centre on third day of illness (85%) as they were referred from lower echelons for further management once they tested positive for dengue fever. The mean hospital duration stay was six days. The most common initial presentation was fever with headache (58%). At the time of admission, 83.6% (92/110) of the individuals had platelet count <1.5 lac/cumm which reduced to 39.1% (43/110) at the time of discharge, with a mean platelet count of 87727/cumm and nadir value of 10000/cumm [Table/Fig-3]. Among the dengue subjects, 19.1% (21/110) of the individuals experienced bleeding manifestations (wet purpura/mucocutaneous bleeding). On the contrary, 39.1% (43/110) had leucopenia on admission which reduced to 8.1% (9/110) on discharge [Table/Fig-3]. The AST and ALT peak value was 900 IU and 942 IU, respectively [Table/Fig-4]. Clinical fluid accumulation was reported in 4.5% (5/110) patients, bleeding manifestations with fluid accumulation in 3.6% (4/110) and only bleeding manifestations in 15.5 % (17/110) [Table/Fig-5]. There was a negative correlation of platelet count with bleeding manifestations (r=-0.17, p=0.04). Platelet values on correlation with serositis revealed negative correlation (r=-0.10, p=0.26). Platelet values also negatively correlated with AST levels (r=-0.23, p=0.01). Bleeding manifestations and serositis showed positive correlation with each other (r=0.19, p=0.04) [Table/Fig-6]. AST and ALT revealed positive correlation with incidence of serositis (r=0.21, p=0.02 and r=0.11, p=0.24), respectively [Table/Fig-7]. The ALT and Packed Cell Volume (PCV) values also showed positive correlation with each other (r=0.22, p=0.01) [Table/Fig-8].
Age Group and Gender distribution of study population.
| Age group (Years) | Female n (%) | Male n (%) | Total (N=110) |
|---|
| 0-20 | 4 (3.6) | 3 (2.7) | 07 |
| 21-30 | 6 (5.5) | 29 (26.4) | 35 |
| 31-40 | 8 (7.3) | 34 (30.9) | 42 |
| 41-50 | 5 (4.5) | 14 (12.7) | 19 |
| >50 | 4 (3.6) | 3 (2.7) | 07 |
Haematological profile (Platelet count, Total Leucocyte Count, Haematocrit).
| S. No. | Variables | Number of patients at the time of admission (%) | Number of patients at the time of discharge (%) |
|---|
| A) Platelet count (mm3): |
| 1. | <50000 | 38 (34.6) | 2 (1.8) |
| 2 | 50000-99999 | 36 (32.7) | 6 (5.5) |
| 3. | 100000-149999 | 18 (16.4) | 35 (31.8) |
| 4. | 150000-199999 | 15 (13.6) | 23 (20.9) |
| 5. | 200000-499999 | 2 (1.8) | 44 (40.0) |
| 6. | ≥500000 | 1 (0.9) | - |
| B) Leucocyte count (mm3): |
| 1. | <4000 | 43 (39.1) | 9 (8.2) |
| 2 | 4000-5999 | 46 (41.8) | 44 (40.0) |
| 3. | 6000-7999 | 14 (12.7) | 43 (39.1) |
| 4. | 8000-12000 | 5 (4.6) | 14 (12.7) |
| 5. | >12000 | 2 (1.8) | - |
| C) Haematocrit: |
| 1. | 9-19 | 2 (1.8) | 1 (1.0) |
| 2 | 20-29 | 2 (1.8) | 3 (2.7) |
| 3. | 30-39 | 38 (34.5) | 44 (40.0) |
| 4. | 40-49 | 62 (56.4) | 59 (53.6) |
| 5. | 50-59 | 6 (5.5) | 3 (2.7) |
| S. No. | Variables | Number of patients at the time of admission (%) | Number of patients at the time of discharge (%) |
|---|
| A) AST (IU/L): |
| 1. | 10-99 | 46 (41.8) | 62 (56.4) |
| 2 | 100-199 | 31 (28.2) | 38 (34.5) |
| 3. | 200-299 | 11(10.0) | 6 (5.5) |
| 4. | 300-399 | 9 (8.2) | 2 (1.8) |
| 5. | 400-499 | 3 (2.7) | 2 (1.8) |
| 6. | 500-599 | 7 (6.4) | - |
| 7. | ≥600 | 3 (2.7) | - |
| B) ALT (IU/L): |
| 1. | 10-99 | 48 (43.6) | 56 (50.9) |
| 2 | 100-199 | 34 (30.9) | 43 (39.1) |
| 3. | 200-299 | 18 (16.4) | 8 (7.3) |
| 4. | 300-399 | 7 (6.4) | 2 (1.8) |
| 5. | 400-499 | 1 (0.9) | 1 (0.9) |
| 6. | 500-599 | 1 (0.9) | - |
| 7. | ≥600 | 1 (0.9) | - |
Dengue severity classification (WHO).
| S. No. | Clinical manifestations | Number of patients (%) |
|---|
| 1. | Dengue without warning signs and symptoms | 84 (76.4) |
| 2. | Dengue with warning signs and symptoms | 17 (15.5) |
| 3. | Severe dengue | 9 (8.1) |
| a. Only serositis | 5 (4.5) |
| b. Bleeding and serositis (present) | 4 (3.6) |
Correlation between bleeding manifestations and serositis (r=0.19, p=0.04).
Correlation between AST levels and serositis (r=0.21, p=0.02).
Correlation between ALT levels and PCV (r=0.22, p=0.01).
Discussion
Dengue infection is characterised by thrombocytopenia leading to bleeding manifestations in severe cases which may lead to fatality. Hence, fall in platelets has been the focus of medical management and therapeutic intervention target. But, an important aspect of disease that is often overlooked is plasma leakage leading to fluid accumulation (pleural effusion, ascites) which may or may not be elicitable clinically, depending upon the amount of the same. Hence, pathogenesis of dengue not only entails thrombocytopenia but also includes plasma leakage that is responsible for clinical manifestations of dengue in the form of postural symptoms, supine hypotension, poor organ perfusion leading to prerenal acute kidney injury and contributing to transaminase elevation (multifactorial-rise in AST).
In this study, 8.1% (9/110) of the study population was classified as severe dengue as per WHO 2009 classification. In order to understand the relation between platelet count and transaminase elevation the two parameters were correlated. Out of AST and ALT, AST levels showed statistically significant negative correlation with platelet values and statistically significant positive correlation with evidence of serositis. On the other hand, ALT levels showed statistically significant positive correlation with PCV values, thereby acting as potential indirect marker for predicting plasma leakage (HCT starts rising once plasma leakage sets in and the same has been used as a surrogate marker of fluid hydration). Individuals with higher levels of AST had severe illness as compared to the individuals with normal or slightly raised levels of transaminases. This finding is important in utilising AST levels as early marker of predicting dengue severity, rather than waiting for the platelet nadir in the critical phase to predict dengue severity [16]. The same has been highlighted in previously conducted studies by Bhushan D and Kumar R and Mahmuduzzaman M et.al., wherein higher levels of transaminase elevation were observed in cases with severe dengue [17,18]. The study conducted by Premaratna R et al., had highlighted the correlation of transaminase elevation with serositis [19]. In a recent meta-analysis conducted by Wang XJ et al., AST levels were found to correlate with severe manifestations of dengue fever, i.e., higher AST levels were seen in severe dengue as compared to dengue without warning signs and symptoms [20]. As per the natural course of dengue fever, thrombocytopenia follows leukopenia, which usually precedes critical phase (24-48 hours prior to onset of critical phase). The same may be associated with delay by almost 2-3 days (depending upon the onset of symptoms, days into illness and day of hospitalisation since the onset of symptoms) in the intensive fluid resuscitation. Haemoconcentration secondary to plasma leakage may also interfere with actual platelet count and the actual platelet count may be erroneous in some cases. Contrary to the same, early AST/ALT peak in the course of illness (earlier compared to development of thrombocytopenia) may act as an early predictive marker for severe dengue.
The advantage of these surrogate markers may be highlighted by the fact that, early AST/ALT peak in the course of illness can be better utilised as early severity marker for dengue fever, as compared to conventional approach of platelet nadir which usually occurs in the mid to latter half of natural course of disease when the individual lands in critical phase of the disease. Also, the correlation of AST levels with incidence of serositis strengthens the future prospects of this biomarker being utilised for predicting dengue severity as fluid accumulation has been used by WHO 2009 guidelines [12] to define severe dengue.
Limitation(s)
The study was carried out in a tertiary care centre with a small sample size and was limited by the fact that cases referred from lower echelons (majority being admitted on third day of illness) constituted the major proportion of the study with majority of the patients belonging to the male gender. This does not define any gender predilection to dengue, nor does it point at increased risk of severe dengue in male gender. The same along with significant percentage of population being classified as severe dengue is just contributed to sampling variability due to data collection in a tertiary care centre.
Conclusion(s)
Apart from re-establishing the fact that serial monitoring of platelet count is important for the prediction of severe dengue, our study highlights the importance of biomarkers like AST/ALT for correlating dengue severity. The same stresses upon the use of multiple biomarkers for better correlation and early prediction of severity of dengue, rather than dependency on a single haematological parameter.
The development of dengue severity prediction scores utilising AST/ALT alone, or in conjunction with platelet count and other biomarkers will aid in better management of dengue fever cases. The same would be beneficial in primary or secondary healthcare levels, wherein early utilisation of such scoring systems will help in early prediction of severe dengue. This will help in early fluid resuscitative measures along with institution of early intensive monitoring/ early referrals to tertiary care setup rather than waiting for age old concept of bleeding and severe thrombocytopenia in critical phase of illness. Hence, such predictive models can aid in reducing the morbidity and mortality associated with dengue fever, especially in countries where tropical infections are common.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Apr 24, 2021
Manual Googling: Sep 09, 2021
iThenticate Software: Sep 17, 2021 (5%)
[1]. de Borba L, Villordo SM, Marsico FL, Carballeda JM, Filomatori CV, Gevhard LG, RNA Structure Duplication in the Dengue Virus 3’ UTR: Redundancy or Host Specificity?MBio 2019 10(1):e02506-18.10.1128/mBio.02506-1830622191 [Google Scholar] [CrossRef] [PubMed]
[2]. Beers NR, Ciupe SM, Modelling original antigenic sin in dengue viral infectionMath Med Biol 2018 35(2):257-72.10.1093/imammb/dqx00228339786 [Google Scholar] [CrossRef] [PubMed]
[3]. Nascimento EJ, Hottz ED, Garcia-Bates TM, Bozza F, Marques ETA, Boyes SMB, Emerging concepts in dengue pathogenesis: interplay between plasmablasts, platelets, and complement in triggering vasculopathyCrit Rev Immunol 2014 34(3):227-40.10.1615/CritRevImmunol.201401021224941075 [Google Scholar] [CrossRef] [PubMed]
[4]. Rachman A, Rinaldi I, Coagulopathy in dengue infection and the role of interleukin-6Acta Med Indones 2006 38(2):105-08. [Google Scholar]
[5]. Hein N, Bergara GH, Moura NB, Cardoso DM, Hirose M, Ferronato AE, Dengue fever as a cause of hemophagocytic lymphohistiocytosisAutops Case Rep 2015 5(3):33-36.10.4322/acr.2015.01626558245 [Google Scholar] [CrossRef] [PubMed]
[6]. Ramzan M, Yadav PS, Sachdeva A, Post-dengue fever severe aplastic anaemia: A rare associationHematol Oncol Stem Cell Ther 2012 5(2):122-24.10.5144/1658-3876.2012.12222828377 [Google Scholar] [CrossRef] [PubMed]
[7]. Qing X, Sun N, Yeh J, Yue C, Cai J, Dengue fever and bone marrow myelofibrosisExp Mol Pathol 2014 97(2):208-10.10.1016/j.yexmp.2014.07.00425016180 [Google Scholar] [CrossRef] [PubMed]
[8]. Dellamonica P, Dengue fever: clinical featuresArch Pediatr 2009 16(Suppl 2):S80-84.10.1016/S0929-693X(09)75306-0 [Google Scholar] [CrossRef]
[9]. Morra ME, Altibi AMA, Iqtadar S, Minh LHN, Elawady SS, Hallab A, Definitions for warning signs and signs of severe dengue according to the WHO 2009 classification: Systematic review of literatureRev Med Virol 2018 28(4):e197910.1002/rmv.197929691914 [Google Scholar] [CrossRef] [PubMed]
[10]. Lee IK, Liu JW, Chen YH, Chen YC, Tsai CY, Huang SY, Development of a simple clinical risk score for early prediction of severe dengue in adult patientsPLoS One 2016 11(5):e015477210.1371/journal.pone.015477227138448 [Google Scholar] [CrossRef] [PubMed]
[11]. Kularatnam GAM, Jasinge E, Gunasena S, Samaranayake D, Senanayake D, Wickramasinghe VP, Evaluation of biochemical and haematological changes in dengue fever and dengue hemorrhagic fever in Sri Lankan children: A prospective follow up studyBMC Pediaterics 2019 19(87):01-09.10.1186/s12887-019-1451-530935373 [Google Scholar] [CrossRef] [PubMed]
[12]. WHO. Dengue guidelines for diagnosis, treatment, preventiona and control New Edition 2009. https://www.who.int [Google Scholar]
[13]. Srikiatkhachorn A, Krautrachue A, Ratanaprakarn W, Wongtapradit L, Nithipanya N, Kalayanarooj S, Natural history of plasma leakage in dengue hemorrhagic fever: A serial ultrasonographic studyPediatr Infect Dis J 2007 26:283-90.10.1097/01.inf.0000258612.26743.1017414388 [Google Scholar] [CrossRef] [PubMed]
[14]. Shah D, Rathi P, Dengue-induced hepatic injuryJournal of The Association of Physicians of India 2017 65:79-82. [Google Scholar]
[15]. Yeh CY, Lu BZ, Liang WJ, Shu YC, Chuang KT, Chen PL, Trajectories of hepatic and coagulation dysfunctions related to a rapidly fatal outcome among hospitalised patients with dengue fever in Tainan, 2015PLoS Neglected Tropical Diseases 2019 13(12):01-11.10.1371/journal.pntd.000781731805088 [Google Scholar] [CrossRef] [PubMed]
[16]. Suleman M, Faryal R, Alam MM, Sharif S, Shaukat S, Aamir UB, NS1 antigen: A new beam of light in the early diagnosis of dengue infectionAsian Pac J Trop Med 2016 9(12):1212-14.10.1016/j.apjtm.2016.10.00727955749 [Google Scholar] [CrossRef] [PubMed]
[17]. Bhushan D, Kumar R, Clinical profile, hepatic dysfunctions, and outcome of dengue patients in a tertiary care hospital of eastern IndiaJournal of the Association of Physicians of India 2018 66(3):52-54. [Google Scholar]
[18]. Mahmuduzzaman M, Chowdhury AS, Ghosh DK, Kabir IM, Rahman MA, Ali MS, Serum transaminase level changes in dengue fever and its correlation with disease severityMymensingh Medical Journal 2011 20(3):349-55. [Google Scholar]
[19]. Premratna R, Raghupathy A, Miththinda JKND, de Silva HJ, Timing, predictors, and progress of third space fluid accumulation during preliminary phase fluid resuscitation in adult patients with dengueInternational Journal of Infectious Diseases 2012 17:505-09.10.1016/j.ijid.2012.12.02123391708 [Google Scholar] [CrossRef] [PubMed]
[20]. Wanga XJ, Weib HX, Jiangb SC, He C, Xu XJ, Peng HJ, Evaluation of aminotransferase abnormality in dengue patients: A meta-analysisActa Tropica 2016 156:130-36.10.1016/j.actatropica.2015.12.01326739659 [Google Scholar] [CrossRef] [PubMed]