Scleroderma is a complex autoimmune rheumatic disease characterised by the widespread fibrosis of skin and visceral organs, dysregulation of immune system and vasculopathy. The aetiology of this disease remains unknown till now. It is known to exist in two forms namely localised and generalised/progressive. It is known to affect females more commonly than males, and also shows a wide range of oral and paraoral manifestations including xerostomia, periodontal disease, restricted mouth opening, burning mouth syndrome, dysphagia, gastroesophageal reflux. Here, authors presents a case of 76-year-old female patient presented with the chief complaint of dry mouth, restricted mouth opening, burning sensation in mouth and reduced taste perception for the past seven years. On the basis of gastrointestinal disorder, Raynaud’s phenomenon, fish mouth appearance and various other extraoral and intraoral features a diagnosis of Progressive Systemic Sclerosis (PSS) was made. The present case also emphasised upon the crucial role of a general dentist in diagnosing such rare systemic diseases. This disease is known to carry a significant burden in the form of pain and disability which potentially limits the proper functioning of major internal organs and results in various life limiting complications. Thus, early diagnosis with appropriate investigations followed by specialist and multidisciplinary approach to treatment, is the key for the successful management of disease.
Case Report
A 76-year-old female reported to the Department of Oral Medicine and Radiology, with the chief complaint of dry mouth, restricted mouth opening, burning sensation in mouth and reduced taste perception for the past seven years.
The physical examination revealed that patient’s fingers were fixed in a claw like position. The skin of the hands was shiny and sclerosed. Prominent sclerodactyly along with fusiform swelling of the thumb was also observed, an evidence of Raynaud’s Phenomenon, as shown in [Table/Fig-1]. Other extraoral features include decreased number of wrinkles giving the face a mask like appearance along with loss of expressions, constricted lips giving the appearance of a “fish mouth” as shown in [Table/Fig-2] and narrow nose that can be attributed to atrophy of ala nasi muscles.
Showing fusiform swelling of the fingers and thumb and Raynaud’s phenomenon.

Showing fish mouth appearance and atrophy of ala nasi.

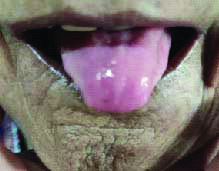
The intraoral manifestations of the patient include restricted mouth opening [Table/Fig-3a], interincisal opening of around 18 mm [Table/Fig-3b], hardening and loss of elasticity of the oral mucosa that may be due to underlying submucosal fibrosis and blanching on oral mucosa in the buccal region (buccal mucosa) [Table/Fig-4]. These features were further accompanied by marked depapillation and atrophy of the tongue [Table/Fig-5].
a) Restricted mouth opening; b) Interincisal opening of 18 mm.

Blenching of oral mucosa.

Depapillation and atrophy of the tongue.
The past medical history and documentation presented by the patient revealed a previous diagnosis of scleroderma for which she was under medication since seven years which included wysolone (in a decreasing dosage starting from 20 mg till present day dosage of 5 mg once a day), azoran (50 mg twice a day) and Risofos (150 mg, monthly once) tablets and is presently on omnacortil (5 mg once a day), azoran and risofos. Other symptoms included gastrointestinal disease in the form of substernal dysphagia with oesophageal dysmotility and heart burn {already diagnosed as Gastrointestinal Reflux Disorder (GERD)}. The small and large intestines were also affected due to smooth muscle atrophy of the bowel that was confirmed previously by a Gastroenterologist. This inturn has resulted in abnormal motility of the gut leading to alternating episodes of diarrhoea and constipation in the patient. The patient was under medications since seven years that included pantocid (once a day), ganaton (once a day), dyoflux (once a day) and moza (5 mg three times a day) but is presently continuing only on pantocid and ganaton. The family history was non contributory.
On systemic examination, Liver Function Test (LFT) (revealed Serum Glutamic Pyruvic Transaminase (SGPT) of 20 IU/L; Serum Glutamic Oxaloacetic Transaminase (SGOT) of 29 IU/L), Echocardiography (ECG) (revealed left ventricular ejection fraction was 60% and left ventricular dysfunction), serum C-Reactive Protein (CRP) was 2.5 mg/L and serum Creatinine Phosphokinase (CPK) was 76.9 units/L. The patient was diagnosed with Grade I diastolic dysfunction based on Electrocardiography (ECG) for which she was under ecosprin (75 mg once a day) and losar (50 mg once a day) for the past seven years and still continuing on the same medications. The patient was also reportedly suffering from fibrosis of lacrimal glands.
The patient was referred to the Department of Oral Pathology for histopathological examination of buccal mucosa as well as salivary glands that revealed submucosal fibrosis as well as fibrosis of salivary glands. The fibrosis of salivary glands, resulted xerostomia or dry mouth in the patient leading to difficulty in chewing, speech and swallowing. Dry eyes occurred as a result of fibrosis of lacrimal glands. Due to inadequate salivary flow, the buffering capacity of saliva was also compromised that made the patient more prone to dental caries. Secondary manifestation such as candidiasis was also observed in the patient on the posterior region of hard palate and tongue. A provisional diagnosis of PSS was established for this patient and further laboratory and radiographic investigations were suggested to rule out other diseases.
Based on the patient’s intraoral findings, a differential diagnosis was given as Oral Submucous Fibrosis (OSMF) and iron deficiency anaemia. Laboratory investigations were carried out in the form of complete blood and urine profile as well as Antinuclear Antibody (ANA) profile. The ANA profile was carried out using immunoblot which revealed positive test for Scl 70 (a scleroderma marker) leading to confirmation of provisional diagnosis. The blood examination revealed haemoglobin levels to be 12.5 gm% and red blood cells count as 4.04 million/mm3, total white blood cells count as 10,200/mm3 and platelet count as 3.78 lacs/mm3. An abnormal high Erythrocyte Sedimentation Rate (ESR) value of 45 mm/hr was also revealed for which the patient was referred to concerned department for opinion and treatment. Also, radiographic investigation was carried out and an Orthopantomograph (OPG) was recorded for the patient as shown in [Table/Fig-6]. A slight widening of the Periodontal Ligament (PDL) space can be observed in the left posterior teeth region of the mandible.
Orthopantomograph (OPG) of the patient.

Based on the all the investigations carried out, a final diagnosis of PSS was established. Appropriate measures were taken to treat the dental implications in the patient. To treat the condition of dry mouth, the patient was prescribed pilocarpine 5 mg (once daily after meal). To begin with, the patient was demonstrated ice cream sticks and ballooning mouth opening exercises to reduce the discomfort from restricted mouth dilating. Patient was encouraged to do the exercise for one minute continuously and as many times as possible in a day. Patient was prescribed Mucofresh Mouthwash (Benzydamine 0.15%), 5-10 mL to swished and spit in undiluted form before each meal. The complaint of reduced taste perception was addressed by prescribing zinc supplements once daily and encouraged maintenance of proper oral hygiene. The patient was recalled after an interval of one week to review the medications and treatment plan but patients lost to follow-up.
All appropriate patient consent forms were obtained by the authors for publication of images and other clinical information required to be reported in the journal. The patient was also informed that the name and initials will not be published and due steps will be taken to conceal her identity.
Discussion
Scleroderma, currently termed as Progressive Systemic Sclerosis (PSS) (Goetz, 1945), is a chronic autoimmune disorder that derives its name from two Greek words scleros (hard) and derma (skin) [1,2]. The aetiology of this disease remains unknown till now. It exists in two forms namely localised and generalised/progressive with former being limited to the midline of the forehead in linear presentation. Morphea, a form of localised PSS, presents with localised indurated skin. An emotional upset or exposure to cold is known to trigger a vasoconstructive event termed as Raynaud’s Phenomenon, that may account for initial signs and symptoms in almost 70% of patients [3-5]. Certain immunological abnormalities such as ANA, anticentromere and anti Scl-70 have been reported in various studies [6]. Another noteworthy clinical feature is that of a hidebound skin that also gives it the name of “hidebound disease” [3].
PSS has been classified based on the extent of skin and internal organ involvement. It is generally divided into limited and diffuse cutaneous subtypes, the latter involving multiple organs like gastrointestinal system, lungs, heart and kidneys [5]. The blood supply to these organs is affected owing to fibrosis [3]. Patients with limited subtype present with typical features of skin sclerosis restricted to the hands with occasional involvement of face and neck, prominent vascular manifestations and frequently exhibit features of CREST syndrome (C=Calcinosis cutis, R=Raynaud’s Phenomenon, E=Esophageal dysmotility, S=Sclerodactyly, T=Telangiectasias) [5].
It is a connective tissue disorder with characteristic fibrosis and excess deposition of collagen fibres mainly type I and III within the skin, blood vessels and internal organs [7]. The fibrosis usually involves skin, mucosa, muscles, and internal organs such as the Gastrointestinal Tract (GI), lungs, blood vessels, and kidneys. Gastroesophageal Reflux Disease (GERD) is observed in most of the patients as the GI tract involvement. It is a rare disorder that presents with involvement of oral and paraoral structures that contribute to a distinct domain of clinical features in the patients [8-12]. These mostly present in the form of mask like facial appearance, microstomia, periodontal diseases, widened PDL space, xerostomia and osseous resorption. Depapillation, atrophy and stiffening of the tongue, constricted lips (fish mouth), oral ulcerations, candidiasis and dental caries are other accompanying orofacial features [3,5,10-12].
In around 80% of patients, symptoms of scleroderma present in the head and neck region. Diagnostic criteria have been recommended by the American College of Rheumatology according to which, truncal sclerosis forms the major criterion while sclerodactyly, digital pitting scars or digital pulp loss and bibasilar pulmonary fibrosis contribute to minor criteria. In the present case report, both the major and minor criteria were observed and recorded. Antinuclear Autoantibodies (ANA) such as antihistone, anti-topoisomerase, anti-U3-RNP, anti-Th, anti-fibrillin, antiphospholipid, can be highly useful in specific diagnosis of PSS [3,6,13,14].
In a case report by Sharma ML et al., extraoral and intraoral findings were similar to the present case report patient, like smooth shiny skin, swelling of the hands and feet, mask-like expressionless face, reduced mouth opening, depapillation of tongue have been reported in a 55-year-old female patient suffering from systemic sclerosis for past 19 years [7]. In another case series reported by Panchbhai A et al., clinical features similar to the present case were recorded like Raynaud’s phenomenon, taut shiny facial skin, reduced mouth opening, blanching of oral mucosa, mask like face, pursing of lips or microstomia with puckering [8]. Altan G et al., reported a case of scleroderma with similar extra and intraoral features to the present case [14]. In all the above case reports, widening of PDL space in OPG was observed in common.
In another case report by Derbi HA and Borromeo GL similar extraoral and intraoral findings were recorded such as interincisal opening of 21 mm which is very close to measurements in the present case [15]. Similar radiographic features to the present case were also recorded like the widening of PDL space i.r.t. 36, 37.
The current treatment protocol is focused on halting or limiting further progression as the fibrosis caused by PSS is irreversible. Medical treatment includes topical, intralesional, or systemic glucocorticoids, vitamin E, vitamin D3, retinoid, penicillin, griseofulvin, and interferon-alpha. In severe cases methotrexate corticosteroids, cyclophosphamide, and azathioprine have been suggested but the efficacy and benefits still remain questionable. Surgical intervention includes restorative plastic surgery using fat or silicone implants, soft tissue grafts or bone implants [16,17].
Various dental implications of the disease have been reported in the form of xerostomia, dental caries, reduced mouth opening, atrophy of tongue papillae and loss of dexterity to maintain oral hygiene leading to poor oral hygiene in these patients. Dentists face a great challenge in such patients when it comes to preservation or restoration of their dentition and treatment of oral mucosal lesions. Maintenance of oral hygiene and frequent counselling (to prevent depression) are key components of the dental treatment. Mouth dilating exercises have been suggested for increasing mouth opening and commissurotomy has been recommended in severe cases. To maintain oral hygiene and prevent caries due to xerostomia, waterpik flossers, flossing forks, artificial saliva, fluoride toothpaste and medications like pilocarpine or oral lubricants like carboxymethylcellulose are suggested for improving oral health. For patients with temporomandibular pain, muscle relaxants, physiotherapy and dental appliances are recommended [2,18].
Conclusion(s)
With the above case report, authors have attempted to emphasise upon the crucial role of general dental practitioners in early diagnosis of such rare ailments with appropriate knowledge and alertness. Timely management of PSS not only requires oral hygiene reinforcement, but also regular clinical and radiological examinations to meet the dental challenges.
[1]. Goetz RH, The pathology of progressive systemic sclerosis with special reference to changes in the visceraClin Proc 1945 4:337-92. [Google Scholar]
[2]. Bali V, Dabra S, Behl AB, Bali R, A rare case of hidebound disease with dental implicationsDent Res J (Isfahan) 2013 10(4):556-61. [Google Scholar]
[3]. Dixit S, Kalkur C, Sattur AP, Bornstein MM, Melton F, Scleroderma and dentistry: Two case reportsJ Med Case Rep 2016 10(1):29710.1186/s13256-016-1086-127776552 [Google Scholar] [CrossRef] [PubMed]
[4]. Ahathya RS, Deepa Lakshmi D, Emmadi P, Systemic sclerosisIndian J Dent Res 2007 18:207-30.10.4103/0970-9290.3091917347542 [Google Scholar] [CrossRef] [PubMed]
[5]. Albilia JB, Lam DK, Blanas N, Clokie CM, Sándor GK, Small mouths. Big problems? A review of scleroderma and its oral health implicationsJ Can Dent Assoc 2007 73:831-36. [Google Scholar]
[6]. Lauritano D, Bussolati A, Baldoni M, Leonida A, Scleroderma and CREST syndrome: A case report in dentistryMinerva Stomatol 2011 60(9):443-65. [Google Scholar]
[7]. Sharma ML, Mehrotra G, Sharma K, Suman S, Tail of the whale appearance: A pathognomonic feature of sclerodermaJ Indian Acad Oral Med Radiol 2020 32:55-59.10.4103/jiaomr.jiaomr_188_19 [Google Scholar] [CrossRef]
[8]. Panchbhai A, Pawar S, Barad A, Kazi Z, Review of orofacial considerations of systemic sclerosis or scleroderma with report of analysis of 3 casesIndian J Dent 2016 7:134-39.10.4103/0975-962X.18670227795648 [Google Scholar] [CrossRef] [PubMed]
[9]. Mayes MD, Lacey JV Jr, Beebe Dimmer J, Gillespie BW, Cooper B, Laing TJ, Prevalence, incidence, survival, and disease characteristics of systemic sclerosis in a large US populationArthritis Rheum 2003 48:2246-55.10.1002/art.1107312905479 [Google Scholar] [CrossRef] [PubMed]
[10]. Chung L, Lin J, Furst DE, Fiorentino D, Systemic and localised sclerodermaClin Dermatol 2006 24:374-92.10.1016/j.clindermatol.2006.07.00416966019 [Google Scholar] [CrossRef] [PubMed]
[11]. White SC, Pharoah MJ, Oral Radiology: Principles and Interpretation 2009 6th edSaint LouisMosby:467 [Google Scholar]
[12]. Greenberg MS, Glick M, Burket’s Oral Medicine Diagnosis and Treatment 2003 10th edIndiaBC Decker Inc., Elsevier:478-502. [Google Scholar]
[13]. Dedic A, Pasalic A, Hodzic M, Basovic S, Avdic M, Pasic E, Scleroderma—from the aspect of dental medicineMed Arh 2011 65(6):368-70.10.5455/medarh.2011.65.368-37022299302 [Google Scholar] [CrossRef] [PubMed]
[14]. Altan G, Kose TE, Erdem TL, Ozcan I, Scleroderma: A case reportJ Istanbul Univ Fac Dent 2015 49(2):31-34.10.17096/jiufd.6805828955533 [Google Scholar] [CrossRef] [PubMed]
[15]. Derbi HA, Borromeo GL, Scleroderma and the oral health implicationsAdv Dent & Oral Health 2018 7(4):55571610.19080/ADOH.2018.07.555716 [Google Scholar] [CrossRef]
[16]. Hunzelmann N, Management of localised sclerodermaSemin Cutan Med Surg 1998 17:31-34.10.1016/S1085-5629(98)80060-6 [Google Scholar] [CrossRef]
[17]. Stone J, Parry-Romberg syndromePract Neurol 2006 6:185-88.10.1136/jnnp.2006.089037 [Google Scholar] [CrossRef]
[18]. Johns FR, Sandler NA, Ochs MW, The use of a triangular pedicle flap for oral commissuroplasty: Report of a caseJ Oral Maxillofac Surg 1998 56:228-31.10.1016/S0278-2391(98)90874-6 [Google Scholar] [CrossRef]