Neck pain is a major musculoskeletal condition. Mechanical neck pain is commonly insidious in onset and multifactorial in its origin [1]. Causative factors for mechanical neck pain include weak neck muscles, neck strain, poor posture, depression and anxiety [2,3]. In about 50-80% cases of the neck pain, there is no determined underlying pathology involved [4]. Worldwide neck pain prevalence ranges from 16.7-75.1%. It has also been reported that females are more prone to neck pain as compared to men [5]. In India, higher prevalence of neck pain was found which was 6.8% among rural population [6].
A wide range of physiotherapeutic interventions are available for mechanical neck pain, however the most efficient intervention remains debatable. Both yoga and PNF technique for neck muscles are widely used form of therapeutics for neck pain. There is no such study on single yoga asana and its effect on bilateral subacute mechanical neck pain. However, one study has been published by Nagrale A and Desai P done on effect of Bhujangasana and Ardh Matsyendrasana on chronic neck pain cases [7].
The PNF is the stimulation of muscular and nervous system with the aim of achieving the highest level of functioning. To achieve this, therapists use motor learning principles and motor control. The PNF utilises positive approach that implies the activities which patient can do. Most efficient way to achieve effective therapeutic results is the functional approach is used by the physiotherapists [8]. The PNF treatment utilises neck pain general guidelines in which the main aim is to increase functional activities, ROM, strength and reduce pain [9].
OM chanting is comprised of three letters A, U and M where A denotes “Akaar” which indicates state of waking, U denotes “Ukaar” signifies state of dreaming and M denotes “Makaar” which is indicative of state of deep sleep [10]. OM is stated as controller of the life force in ancient yoga texts “yoga sutras” [11]. Previous researches stated that OM chanting causes deactivation of limbic system [12] whereas other literature suggested that OM chanting improved memory, physiological alertness [13-15]. Ardh Matsyendrasana or half spinal twist posture has the most beneficial effects on musculoskeletal systems including spinal deformities and back pain [16].
PHYOG© is combination of Physiotherapy (PNF), Ardh Matsyendrasana and OM Chanting (yoga). Phyog is a term coined by authors which represented combined application of physiotherapy and yoga approach for bilateral subacute mechanical neck pain [17].
The objective of this research was to evaluate the effectiveness of combined effect of Ardh Matsyendrasana along with OM Chanting and PNF neck patterns in the treatment of patients with sub-acute mechanical neck pain, especially their efficacy in increasing functionality, enhancing quality of life and improving neck ROM and also to determine which treatment method is best form in subacute mechanical neck pain. The present study is a part of a larger project, so authors included two outcome parameters in this present study: CROM and quality of life parameters.
Materials and Methods
This randomised controlled trial was conducted in Amity Institute of Physiotherapy OPD, Amity University, Noida, Uttar Pradesh, India, between January 2019 to January 2021. After receiving the ethical clearance from Institutional Ethical Committee of Amity University, Noida, UP, India (IEC no. AUUP/IEC/2018-AUG/05) prior to the data collection, and registered under Clinical Trial Registry of India (registration number CTRI/2019/01/016985), 122 patients were selected using consecutive convenient sampling method. The patients who were willing to participate in the study were screened on the basis of inclusion and exclusion criteria. Participants were informed about the study procedure and a written consent form was taken from them. Subjects were given intervention for four weeks.
Inclusion criteria: The inclusion criteria for this study were: patients with bilateral subacute mechanical neck pain for the duration of 6-12 weeks aged 18-30 years with Neck Disability Index (NDI) <40% [18,19], and those who have dull aching pain increased by sustained neck postures.
Exclusion criteria: The exclusion criteria included subjects with diagnosed spinal deformities (including poked neck deformity), cervical spondylitis with radiculopathy, diagnosed case of neoplasm or inflammatory disease of neck, history of cervical osteoporosis, fracture, whiplash injury, low back pain, cervicogenic headache, or cervical surgery.
Selection of Patients and Randomisation
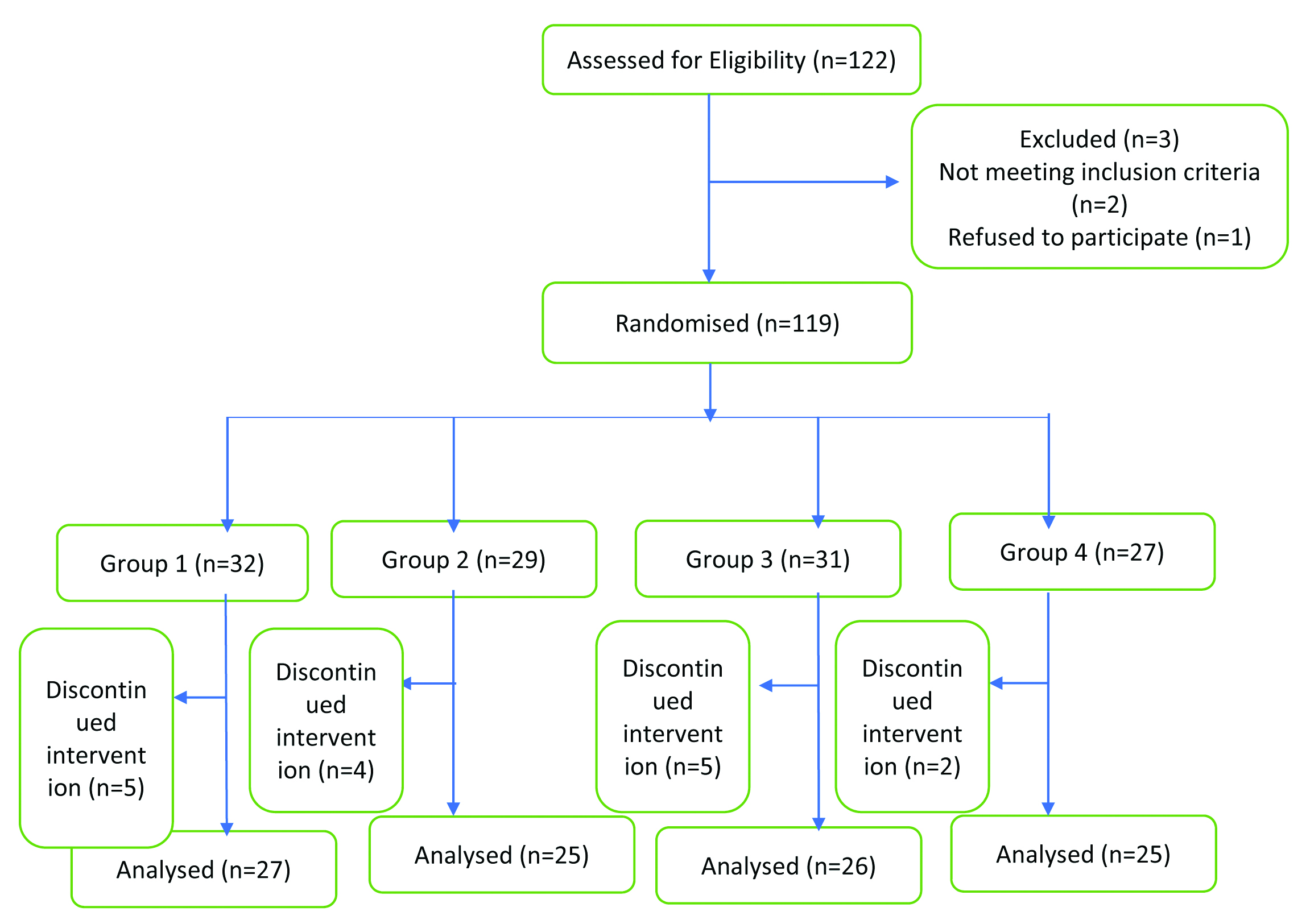
A total of 122 Subjects who met the inclusion criteria were selected. Among them, three patients were excluded as they did not meet the inclusion criteria and refused to participate. About 119 subjects were randomly allocated into four groups using computer software “research randomiser” after obtaining their baseline measurements. Baseline measurements included CROM assessed with digital goniometer and health related quality of life measurements using SF-36v2 tool. After randomisation, 103 subjects who completed their intervention till four weeks were analysed. Some patients discontinued the intervention and the total subjects analysed in these groups were: PNF group (n=27) performed bilateral PNF neck patterns, yoga group (n=25) performed Ardh Matsyendrasana along with OM Chanting, combined group (n=26) performed PNF, Ardh Matsyendrasana with OM Chanting combinedly and control group (n=25) performed bilateral active stretching of sternocleidomastoid and rhomboids muscles. All the groups received four week intervention program with five days per week with 15 minutes exercise per day. Fifteen minutes exercise for combined group included combined approach of both PNF neck patterns and Ardh Matsyendrasana alongwith OM chanting so it was sufficient and had similar time duration per day, like given in the other treatment groups. Hot packs were given for five minutes postexercise. Also, ergonomic advices were given to all the groups.
Intervention
PNF group intervention (Group 1): They performed diagonal neck pattern movement in sitting posture. The process of neck flexion along with right rotation and extension of neck with left rotation was repeated bilaterally (on both sides) with 10 seconds hold and 10 seconds relaxing. Movements were repeated as per following- nine times each side per set. Two sets of exercises were performed for six minutes each set, with three minutes rest in between the sets, completing total 15 minutes exercise per day [18,19]. Nine times each side per set was included because each set comprised of six minutes duration which includes both right and left side exercises. So, dividing six minutes for two sides gives three minutes (180 seconds) each side per set. And as per protocol 10 seconds contraction and 10 seconds relaxation yielded nine times each side per set (180 seconds for right side and 180 seconds for left side).
Yoga group (Group 2): They performed Ardh Matsyendrasana with OM chanting. OM chanting was played using prerecorded tape with headphones and the subject was advised to rhyme OM chanting along with it while performing the asana. While performing the Ardh Matsyendrasana, subject was advised to inhale deeply, rotate trunk to one side in asana position and while exhaling chant OM and maintain that position for 10 seconds, then come back to neutral position and rest for 10 seconds. This process was repeated for nine times each side per set with two sets of six minutes each with three minutes rest in between the both sets.
Asana position: In sitting posture, rotate neck and upper trunk along with abdomen. The right arm is pressed against the left knee and the left arm is wrapped behind the back. Right leg and knee stay on floor. This position opens up chest [20,21]. The process of yoga with OM chanting was detailed to the patient on the very first day of the session.
Phyog group (Group 3): This group performed the combination of Ardh Matsyendrasana along with OM chanting and PNF technique. In this, the subject attains Ardh Matsyendrasana yoga posture along with OM chanting with diagonal neck pattern movements including flexion of neck with right rotation and extension of neck with left rotation. This process was done on both sides with two sets and three minute rest in between both sets. Each set was of six minutes. Position of Ardh Matsyendrasana along with PNF neck movement was held for 10 seconds and OM chanting was played using headphones.
Control Group (Group 4): This group performed bilateral active stretching of rhomboids and sternocleidomastoid muscles. For rhomboids stretching, patient was in sitting posture and moved his right arm across the chest with right elbow extended and held the right elbow with left hand and stretched it by applying pressure with left hand over right elbow. In this posture, trunk was in erect neutral position. Stretching was maintained for 10 seconds with 10 seconds relaxation.
For sternocleidomastoid stretching, patient was in sitting position, with left hand holding chair and right hand over head. Patient laterally flexed the neck to right and rotated to left while pulling with the right hand. This process was also repeated bilaterally with 10 sec hold and 10 seconds relaxation, nine times each side per set followed by three minutes rest in between the both sets.
(Treatment duration for all four groups was 15 minutes of exercise. Only Ardh matsyendrasana was included, as authors intended to check efficacy of the single asana).
Outcome Measures
Outcome was measured for CROM with digital goniometer and health related quality of life parameter using SF-36v2 [22]. Both the outcome measures were assessed at the baseline and after the end of intervention (four weeks).
The CROM was evaluated in three planes right and left lateral flexion in coronal plane, flexion and extension in sagittal plane and right and left rotation in horizontal plane. The CROM was assessed with digital goniometer ATRIUM 200 mm digital electronic angle finder goniometer.
The SF-36v2 is a tool which is used to assess health related quality of life. It includes eight subscales to evaluate quality of life parameter {Role-Emotional (RE), General Health (GH), Role-Physical (RP), Vitality (VT), Bodily Pain (BP), Physical Functioning (PF), Social Functioning (SF), and Mental Health (MH)} [22]. All health domains are scored in such a way that higher scores interpret better health. The SF-36v2 is a revised version of SF-36® Health Survey. Licence was obtained for the present study with licence number QM054639. Physical component correlates with three scales (RP, PF and BP) and contribute to scoring of the Physical Component Summary (PCS) measure. Subscales RE, MH, and SF correlates with the mental component, which contribute to the scoring of the Mental Component Summary (MCS) measure.
The improvement scores (%) for CROM and SF-36v2 were calculated using the following formula:

Statistical Analysis
The analysis of data scored was done in IBM Statistical Package for the Social Sciences (SPSS) software version 26.0. Both baseline and four week postintervention data were collected and analysed. Within group, paired t-test was applied. A p-value <0.05 was considered statistically significant for all outcome measures.
Results
A total of 122 patients were assessed for eligibility, out of which three excluded due to their unwillingness to participate and not meeting inclusion criteria. Further dropouts lead to total of 103 subjects whose complete analysis was done, in which 27 subjects were in the group 1, 25 subjects in group 2, 26 subjects in group 3 and 25 subjects were in the group 4 were analysed. These dropouts have been depicted in CONSORT flowchart in [Table/Fig-1]. Age of the subjects ranged from 18-30 years. Female subjects were in more percentage as compared to males in all the groups except in group 3 where males were more than females. Baseline characteristics as outlined in [Table/Fig-2], mean and standard deviation of age in the group 1 was 25.1±3.6, group 2 was 26.6±3, group 3 was 27.3±2.6 whereas group 4 was 26.5±3. Baseline characteristics including age, gender, duration of symptoms and baseline NDI are shown in [Table/Fig-2]. The CROM is shown in [Table/Fig-3] and quality of Life parameter with SF-36v2 questionnaire is depicted in [Table/Fig-4].
CONSORT flow diagram of study.
Baseline clinical characteristics of 103 patients with mechanical neck pain in four groups.
| Variables | Group 1 | Group 2 | Group 3 | Group 4 |
|---|
| Age in years (Mean±SD) | 25.1±3.6 | 26.6±3 | 27.3±2.6 | 26.5±3 |
| Sex (F/M), n (%) | 18/9 (66.7/33.3)% | 15/10 (60/40)% | 10/16 (38.5/61.5)% | 17/8 (68/32)% |
| Duration of pain in weeks, (Mean±SD) | 8.1±1.9 | 7.9±1.9 | 8.3±2.1 | 8.4±1.7 |
| NDI (baseline) (Mean±SD) | 26.9±4.3 | 25.4±3.6 | 28.4±5.3 | 27±4.7 |
Comparison of Cervical Range Of Motion (CROM) (within group analysis).
| Parameters | Variables | Group 1 (n=27) Mean±SD | Group 2 (n=25) Mean±SD | Group 3 (n=26) Mean±SD | Group 4 (n=25) Mean±SD |
|---|
| Cervical flexion, (degrees) | Baseline | 66.4±7.5 | 62.1±7.5 | 59.3±7.7 | 61±6 |
| Post 4-week intervention | 72.9±6.1 | 69±7.2 | 65.7±7.7 | 64.2±6 |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 |
| Improvement score (%) | 9.72 | 11.16 | 10.72 | 5.15 |
| Cervical extension (degrees) | Baseline | 58.8±7.5 | 52.6±6 | 50.9±6.1 | 51.5±6.6 |
| Post 4-week intervention | 65.9±6.5 | 61.3±4.7 | 58.3±6.8 | 54.7±6.6 |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 |
| Improvement score (%) | 12.13 | 16.52 | 14.57 | 6.23 |
| Cervical right lateral flexion (degrees) | Baseline | 26.4±6.6 | 28.1±6.2 | 25.9±4.6 | 27.2±5 |
| Post 4-week intervention | 30±6.6 | 34.9±6.9 | 32.4±5 | 30.7±5.5 |
| p-value | 0.007 | 0.001 | 0.001 | 0.001 |
| Improvement score (%) | 13.55 | 24.11 | 25.12 | 12.97 |
| Cervical left lateral flexion (degrees) | Baseline | 28.7±6.7 | 27.7±6.4 | 27.6±5.5 | 26.6±5.2 |
| Post 4-week intervention | 32±6.6 | 35.2±4.6 | 31.4±6.9 | 31.2±5.1 |
| p-value | 0.029 | 0 | 0 | 0 |
| Improvement score (%) | 11.56 | 27.10 | 13.81 | 17.08 |
| Cervical right rotation (degrees) | Baseline | 68.6±8.1 | 59.1±7.6 | 58.9±5.5 | 55.8±7.1 |
| Post 4-week intervention | 75.1±5.6 | 66.7±9.3 | 66.2±6.2 | 61.5±6.4 |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 |
| Improvement score (%) | 9.38 | 12.81 | 12.29 | 10.15 |
| Cervical left rotation (degrees) | Baseline | 69±8.8 | 60.8±8.2 | 57.6±6 | 55.9±7.4 |
| Post 4-week intervention | 72.6±9.5 | 67.7±6.8 | 64.8±7.1 | 60.7±5.7 |
| p-value | 0.034 | 0.001 | 0.001 | 0.001 |
| Improvement score (%) | 5.20 | 11.48 | 12.54 | 8.67 |
All p-values <0.05 so all values were significant; Test applied for within group analysis was paired t-test
Comparison of Short Form 36 (SF-36v2) questionnaire (within group analysis) SF-36v2 questionnaire software provided us with the data analysis done with the software and the values were obtained and those values/results were interpreted using within group analysis with paired t-tests using mean±SD.
| Parameters | Variables | Group 1 (n=27) Mean±SD | Group 2 (n=25) Mean±SD | Group 3 (n=26) Mean±SD | Group 4 (n=25) Mean±SD |
|---|
| Physical Component Summary (PCS) | Baseline | 43±4 | 42.6±3.6 | 44.2±3.3 | 45.3±3.2 |
| Post 4-week intervention | 48.2±4.7 | 48.2±4 | 48.5±3.4 | 50.2±3.7 |
| p-value | 0.001 | 0.001 | 0.001 | 0.002 |
| Improvement score (%) | 12.13 | 13.30 | 9.89 | 10.85 |
| Mental Component Summary (MCS) | Baseline | 35.7±2.5 | 35.3±2.9 | 35.4±3.6 | 35.1±1.9 |
| Post 4-week intervention | 39.7±3.7 | 41±4.7 | 42.3±3 | 40.7±4.6 |
| p-value | 0.001 | 0.001 | 0.001 | 0.001 |
| Improvement score (%) | 11.39 | 16.16 | 19.28 | 15.73 |
All p-values <0.05 so all values were significant. Test applied for within group analysis was paired t-test
The CROM measurements within group analysis showed statistically significant results for all groups from baseline to four weeks postintervention (p<0.05) which interprets that active CROM for all neck ROM were improved with treatment.
The SF-36v2 scores within group analysis showed improvements in all sub scores of the questionnaire in all the four groups (p<0.05) after four weeks of intervention.
Discussion
This study investigates the effect of Ardh Matsyendrasana along with OM chanting and PNF technique on neck ROM and quality of life in bilateral subacute mechanical neck pain cases. The major findings of this study suggests that with the techniques of neck PNF patterns, Ardh Matsyendrasana with OM chanting and active stretching of sternocleidomastoid and rhomboids muscles, there is increase in neck ROM and quality of life after 4-weeks of intervention in all study groups as well as control group demonstrated statistically significant improvement in both the outcome measurement (p<0.05 for all study groups).
Within group analysis showed statistically significant improvement in all CROM i.e., flexion, extension, right and left lateral flexion and right and left rotations, in all the four groups. The improvement scores showed that the group performing Ardh Matsyendrasana with OM chanting and combined PNF neck patterns with Ardh Matsyendrasana and OM chanting showed better improvement in neck flexion, extension, right and left lateral flexion and right and left rotation ROM as well improved mental and physical component scores of quality of life parameter for bilateral subacute mechanical neck pain cases.
This may be due to the reason that PNF utilises rotational and multi-dimensional pattern of movement which improves neuromuscular mechanism of neck muscles. Also, Ardh Matsyendrasana involves stretching as well as strengthening of upper and lower neck muscles along with stretching of upper trunk muscles which in turn improves neck ROM.
In support of the present study, Rezasoltani A et al., reported that the efficacy of PNF for improving neck ROM is due to combination of stretches and contractions in alternating pattern whose main target is the facilitation of agonist muscle which leads to increase in the motor neuron excitability and hence improves joint ROM [23]. Vallath N in support of our claim reported in their study that parasympathetic system activates through yoga asana by increasing the blood flow which affects nerve plexuses and endocrine system which in turn affects neuronal flow [24]. Relaxation response is initiated by yoga asana and OM chanting in the neuroendocrinal system that combines with the physiological system which in turn leads to decrease in myofascial tension and thereby improves joint ROM [25]. In the present study, we have found statistically significant improvement of CROM in active stretching of neck muscles (p<0.05). In a similar study, it has been observed that joint ROM increases due to static stretching as it causes increase in muscle extensibility [26] as well as increment of stretch tolerance [27,28].
In the assessment of quality of life, within group analysis, demonstrated statistically significant improvement in all four groups post 4-weeks of treatment (p<0.05). Improvements within the group might be attributed to involvement of holistic mind and body coordination through yoga posture and OM chanting which enhances mental component of our body.
Iyengar BKS stated that yogasana posture induces psychological and physical improvement in mechanical neck pain because it principally involves isometric muscle strengthening as well as stretching of neck and upper trunk muscles and along with OM chanting it focuses on mindfulness of body movements and regulation of breathing patterns [29]. People with neck pain also prefer complimentary or alternative methods for relief of pain and neck pain related anxiety [30]. OM chanting has been found to be an important exercise for exhalation [31]. In a similar study, it was found that OM chanting also has an effect on autonomic functions which causes significant decrease in the blood pressure and also decrease stress, depression and anxiety scores [32].
In contrast to the present study, Jadeja T et al., showed that 4-weeks PNF intervention on chronic low back pain did not show any improvement in quality-of-life parameter [33]. No study has been designed till date on the combined approach of physiotherapy and yoga on subacute mechanical neck pain.
Limitation(s)
The limitations of this study was that it was limited by its small sample size. Also, follow-up was not there which can be incorporated in further studies to assess whether these beneficial effects on outcomes persist even postintervention or do they decline with time.
Conclusion(s)
In conclusion, supervised 4-weeks intervention program of PNF neck pattern, Ardh Matsyendrasana with OM chanting, active stretching exercises of neck muscles and combined Ardh Matsyendrasana with OM chanting and neck PNF all provides significant improvement in CROM and in health-related quality of life of patients with bilateral sub-acute mechanical neck pain. But Improvement scores showed that the group performing Ardh Matsyendrasana with OM chanting and combined PNF neck patterns with Ardh Matsyendrasana and OM chanting showed better improvement in neck flexion, extension, right and left lateral flexion and right and left rotation ROM as well improved mental and physical component scores of quality-of-life parameters for bilateral subacute mechanical neck pain cases when compared with other study groups. Yoga group combined with PNF pattern proved to be a beneficial treatment for subacute mechanical neck pain.
All p-values <0.05 so all values were significant; Test applied for within group analysis was paired t-test
All p-values <0.05 so all values were significant. Test applied for within group analysis was paired t-test