Differing High Resolution Computed Tomography Patterns of COVID-19 Disease
Ramakrishna Narra1, Kaniti Sruthi2
1 Professor, Department of Radiology, Katuri Medical College, Guntur, Andhra Pradesh, India.
2 Junior Resident, Department of Radiology, Katuri Medical College, Guntur, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ramakrishna Narra, Professor, Department of Radiology, Katuri Medical College, Guntur, Andhra Pradesh, India.
E-mail: narra.ramki29@gmail.com
Coronavirus disease 2019, Crazy paving pattern, Ground glass opacities
Dear Editor,
Coronavirus Disease-2019 (COVID-19) disease is a severe acute respiratory syndrome caused by the coronavirus. The first human case of COVID-19 was reported in Wuhan, China, in December 2019. The imaging findings of the chest in patients with COVID-19 infection were first published in January 2020 and in majority of patients, ground-glass opacities involving bilateral lung fields were noted [1].
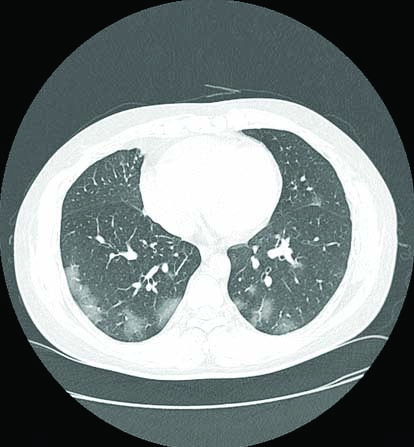
In August 2020, during the first wave of the COVID-19 pandemic, a 41-year-old male patient who had no co-morbidities and presented with fever, chills, myalgia, and dry cough for four days was admitted to our tertiary care centre. The real-time Reverse Transcription-Polymerase Chain Reaction (RT-PCR) for COVID-19 was performed and was positive. The High-Resolution Computed Tomography (HRCT) of the chest performed [Table/Fig-1] on the same day demonstrated bilateral multifocal subpleural ground-glass opacities, predominantly in the lower lobes. The Computed Tomography (CT) severity score index as per study by Li K et al., was 10, indicating that the disease was moderate in severity [2]. The patient was treated with Tab Ivermectin 200 mcg/kg once daily, Tab Doxycycline 100 mg twice daily, and Tab paracetamol 650 mg thrice daily for five days. Following which he recovered completely after 10 days from the date of admission to the hospital.
Axial HRCT chest in lung window demonstrating bilateral multifocal subpleural ground-glass opacities.
In April 2021, during the second wave of COVID-19 pandemic, a 47-year-old male patient with no co-morbidities and presented with fever since four days and gradually developed dry cough and shortness of breath since two days was admitted to our tertiary care COVID-19 centre. On examination at admission, the patient’s oxygen saturation was 81% on room air, and heart rate was 120 beats per minute. RT-PCR was performed which tested positive for coronavirus disease (COVID-19). HRCT chest was performed [Table/Fig-2], showing diffuse ground-glass opacities with thickening of the interlobular and intralobular septa, with a typical ‘crazy paving pattern’ in the bilateral lung fields. CT severity score was 17, which is indicative of severe disease. The patient was treated with methylprednisolone 1-2 mg/kg IV in two divided doses and enoxaparin 0.5 mg/kg subcutaneously twice daily for 10 days. He was also supported with five litres of oxygen to maintain oxygen saturation. However, four days following the treatment, the symptoms of patients worsened and the patient needed respiratory support. He succumbed due to cardiac arrest secondary to respiratory failure.
Axial HRCT chest lung window demonstrating diffuse ground-glass opacities with typical ‘crazy-paving pattern’ in the bilateral lungs.

From April 2020 to September 2020, during the first wave of the pandemic, HRCT was performed in 22 RTPCR confirmed COVID-19 patients of age group 40-50 years with no co-morbidities. HRCT severity score in (six cases) of patients was moderate, and (four cases) of patients was severe. Only (five cases) of patients require mechanical ventilation, and (two cases) of these patients succumbed. In (13 cases) of patients, bilateral multifocal subpleural ground-glass opacities was the most common pattern and the prognosis of these patients was good.
From March 2021 to June 2021, during the second wave of pandemic, the HRCT patterns in 19 RT-PCR positive patients with no co-morbidities were studied. The age group of patients was 40-50 years. HRCT severity score in (five cases) of these patients was moderate and (seven cases) was severe. Among these patients, (eight cases) required mechanical ventilation and (six cases) of patients have succumbed. The majority of patients (12 cases) demonstrated diffuse ground-glass opacities with ‘crazy paving pattern’ on HRCT showed poor prognosis.
These varying HRCT patterns observed during different phases of COVID-19 pandemic among the same age groups patients with no co-morbidities could be attributed to difference in the variance in the virulence and pathogenicity of the coronavirus disease in addition to various other possible contributing factors. However, large scale multicentric studies need to be performed to corroborate the same.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 24, 2021
Manual Googling: Sep 13, 2021
iThenticate Software: Sep 18, 2021 (7%)
[1]. Kwee TC, Kwee RM, Chest CT in COVID-19: What the Radiologist Needs to KnowRadioGraphics 2020 40(7):1848-65.10.1148/rg.202020015933095680 [Google Scholar] [CrossRef] [PubMed]
[2]. Li K, Wu J, Wu F, Guo D, Chen L, Fang Z, Li C, The clinical and chest CT features associated with severe and critical COVID-19 pneumoniaInvest Radiol 2020 55(6):327-31.10.1097/RLI.000000000000067232118615 [Google Scholar] [CrossRef] [PubMed]