Leiomyosarcoma: A Rare Cause of Colocolic Intussusception
Prashanth Puvvada1, Nain Singh2, Om Prakash Pathania3, Raghav Yelamanchi4
1 Senior Resident, Department of Surgery, Lady Hardinge Medical College, New Delhi, India.
2 Professor, Department of Surgery, Lady Hardinge Medical College, New Delhi, India.
3 Professor, Department of Surgery, Lady Hardinge Medical College, New Delhi, India.
4 Senior Resident, Department of Surgery, Atal Bihari Vajpayee Institute of Medical Sciences and Dr. Ram Manohar Lohia Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghav Yelamanchi, Ward 17, Atal Bihari Vajpayee Institute of Medical Sciences and Dr. Ram Manohar Lohia Hospital, New Delhi, India.
E-mail: raghavyelamanchi@gmail.com
Intussusception is an infrequent presentation in adult patients and accounts for less than 1% of all cases of adult bowel obstruction. Colon is most commonly involved site and in 56% cases, the underlying cause is a malignant neoplasm. Leiomyosarcoma of colon is an extremely rare tumour. A 30-year-old male patient presented to the Surgery Department with chief complaints of dull, diffuse and colicky abdominal pain associated with abdominal distension and vomiting for 15 days. On abdominal examination, abdomen was distended with generalised tenderness and rigidity. X-ray abdomen showed features suggestive of bowel obstruction. Contrast Enhanced Computed Tomography (CECT) revealed bowel within bowel appearance of a segment of descending colon suggestive of colocolic intussusception. Exploratory laparotomy revealed colocolic intussusception with a large obstructing growth in the descending colon acting as a lead point. Left hemicolectomy with colocolic anastomosis was done. Final histopathological report confirmed epithelioid leiomyosarcoma. Adjuvant chemotherapy was administered and the patient is disease free at one year of follow-up. Present case report was a rare case of colonic leiomyosarcoma presenting with intussusception. The rarity of this disease and the rare presentation makes this an interesting case. Surgical management remains the mainstay of treatment of these cases.
Abdominal distension, Bowel obstruction, Colonic malignancy, Hemicolectomy, Soft tissue sarcoma
Case Report
A 30-year-old male patient presented with chief complaints of dull, diffuse and colicky abdominal pain which was associated with abdominal distension for 15 days. Pain was initially intermittent to start with and later continuous. There were no aggravating or relieving factors. Patient also gave history of multiple episodes of non projectile bilious vomiting for 10 days and history of loose stools with melena for five days. He had history of significant weight loss with anorexia over the past one month. There was no past history of similar complaints. There was no significant personal and family history. No history of any co-morbidities.
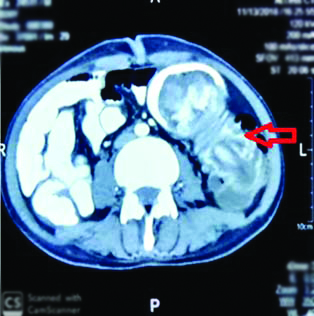
On examination, his blood pressure was 108/70 mmHg with pulse rate of 110 beats per minute. On general examination, he was poorly nourished and pallor was present. On abdominal examination, abdomen was distended with generalised tenderness and rigidity. Bowel sounds were absent. Rest of the systemic examination was normal. X-ray abdomen showed features suggestive of bowel obstruction. Ultrasound scan of the abdomen revealed a heteroechoic lesion with intermingled bowel loops and mild free fluid in the peritoneal cavity. Contrast Enhanced Computed Tomography (CECT) showed bowel within bowel appearance of a segment of descending colon suggestive of colocolic intussusception [Table/Fig-1]. A provisional diagnosis of colocolic intussusception was made. In view of the age of the patient and history, malignancy was strongly considered as an aetiology of intussusception. Other differential diagnosis considered were benign polyps, haematoma due to angiodysplasia and other mass lesions of colon. These were ruled out by the absence of chronic symptoms and absence of lower gastrointestinal bleeding. Patient was taken up for emergency laparotomy.
Contrast Enhanced Computed Tomography (CECT) image showing intussusception of the bowel.
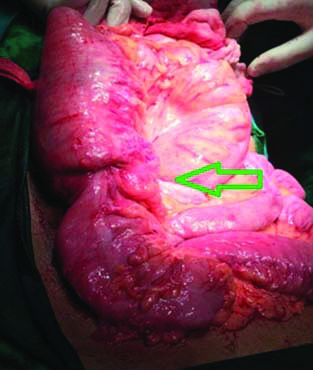
On preanaesthetic evaluation, haemoglobin was 9.6 gm/dL. The total leukocyte count and platelet count were normal. Serum creatinine was 1.5 mg/dL. Liver function tests and serum electrolytes were normal. After thorough resuscitation laparotomy was performed. On laparotomy, there was a colocolic intussusception involving the descending colon [Table/Fig-2] with large obstructing growth in the descending colon acting as a lead point [Table/Fig-3]. Left hemicolectomy was done removing the distal transverse colon and descending colon. Left ureter and gonadal vessels were identified and preserved. Intestinal continuity was restored by a stapler anastomosis between the transverse and remaining descending colon with a proximal diversion loop ileostomy. Patient had an uneventful postoperative recovery. Injection ceftriaxone 1000 mg twice a day and injection metronidazole 500 mg thrice a day were administered intravenously postoperatively.
Intraoperative image of bowel intussusception.
Intraoperative image of the lead point.

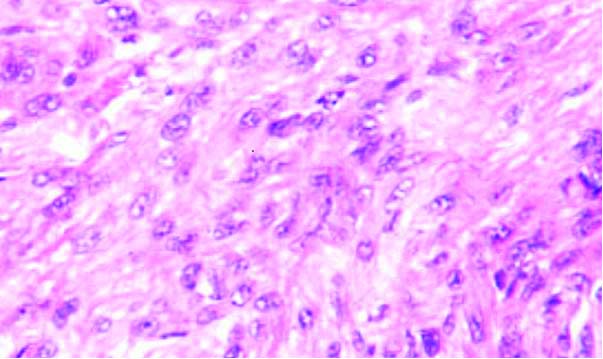
The stoma was functional from the 2nd postoperative day and the patient was discharged on 7th postoperative day. Final histopathological report was suggestive of epithelioid leiomyosarcoma of high grade and poor differentiation T2, N0, grade 3 (Fédération Nationale des Centres de Lutte Contre Le Cancer grading) [Table/Fig-4]. All margins were free of tumour. There was no lymphovascular invasion. CECT chest was done in the postoperative period did not reveal any metastasis. The final stage was IIIA. Six cycles of vincristine, cyclophosphamide and adriamycin chemotherapy were administered at three weekly intervals after discussing the case with multidisciplinary cancer team. Six weeks after the last chemotherapy cycle, proximal loop ileostomy was closed. At one year of follow-up, patient is doing well with CECT showing no signs of recurrence.
Histopathological image of the leiomyosarcoma (400X).
Discussion
Intussusception occurs when a proximal portion of bowel (intussusceptum) invaginates into the distal portion (intussuscipiens). Intussusception is responsible for less than one percent of the causes of bowel obstruction [1]. In adults 56%, of the cases of colonic intussusception are due to a gastrointestinal neoplastic lesion which acts as lead point. Most of these patients have a history of intermittent bowel obstruction occurring over days to years [2]. The present case report was a rare case of leiomyosarcoma of colon leading to intussusception.
Preoperative diagnosis of intussusception often missed due to vague abdominal complaints and operative findings are diagnostic. Endoscopy may diagnose the lesion preoperatively. However, endoscopy is often not performed fearing the complication of bowel perforation in the acute setting. Surgery is the mainstay of treatment for adult intussusception given the high probability of malignancy as the underlying aetiology [3]. Resection allows the removal of potentially malignant lesion and prevents the recurrence of intussusception [4].
Leiomyosarcoma is an extremely rare tumour arising from the smooth muscle of the muscularis mucosa of the bowel wall. It commonly arises in the retroperitoneal space, female genital tract and soft tissues of the extremities. The tumours are negative for CD 117 and CD 34 immunohistochemical markers but positive for desmin and smooth muscle actin. Only 0.1-3% of all leiomyosarcomas arises in the gastrointestinal tract. Increasing size, irregularity of cells, foci of necrosis and heterogenous echogenicity have shown to be associated with high malignant nature of the tumour [5]. High grade leiomyosarcomas are resected with a safe margin of atleast five centimetres [6]. Adjuvant radiotherapy and/or chemotherapy with vincristine, adriamycin and cyclophosphamide are advised in poorly differentiated, high grade tumours with lymphovascular invasion and positive surgical margins based on the experience of chemotherapy in uterine leiomyosarcomas [7].
Two cases of colocolic intussusception caused by intraluminal lipoma of colon were reported by Yoldas T et al., [8]. In both the cases the presentation was sub acute onset intestinal obstruction. Another case of sub acute onset colocolic intussusception caused by intraluminal lipoma was reported by Ravi SJC [9]. Hamilton AE et al., reported a rare case of large bowel obstruction caused by co-presenting colocolic intussusception due to colonic polyp and caecal bascule [10]. The presentation was of acute onset. Wilson A et al., reported a rare case of chronic colocolic intussusception caused by adenocarcinoma of colon [11].
Conclusion(s)
This was a rare case of colonic leiomyosarcoma presenting with intussusception. The rarity of this disease and the rare presentation makes this an interesting case. It should be considered as a differential diagnosis in large bowel obstruction. Surgical management remains the mainstay of treatment of these cases. The role of chemotherapy is controversial with no strong recommendations. The existing treatment protocols are based on the response of uterine leiomyosarcomas to chemotherapy.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 10, 2021
Manual Googling: Aug 25, 2021
iThenticate Software: Sep 14, 2021 (10%)
[1]. Zubaidi A, Al-Saif F, Silverman R, Adult intussusception: A retrospective reviewDis Colon Rectum 2006 49(10):1546-51.10.1007/s10350-006-0664-516990978 [Google Scholar] [CrossRef] [PubMed]
[2]. Weilbaecher D, Bolin JA, Hearn D, Ogden W 2nd, Intussusception in adults. Review of 160 casesAm J Surg 1971 121(5):531-35.10.1016/0002-9610(71)90133-4 [Google Scholar] [CrossRef]
[3]. Takeuchi K, Tsuzuki Y, Ando T, Sekihara M, Hara T, Kori T, The diagnosis and treatment of adult intussusceptionJ Clin Gastroenterol 2003 36(1):18-21.10.1097/00004836-200301000-0000712488701 [Google Scholar] [CrossRef] [PubMed]
[4]. Azar T, Berger DL, Adult intussusceptionAnn Surg 1997 226(2):134-38.10.1097/00000658-199708000-000039296505 [Google Scholar] [CrossRef] [PubMed]
[5]. Lee SH, Ha HK, Byun JY, Kim AY, Cho KS, Lee YR, Radiological features of leiomyomatous tumours of the colon and rectumJ Comput Assist Tomogr 2000 24(3):407-12.10.1097/00004728-200005000-0000910864076 [Google Scholar] [CrossRef] [PubMed]
[6]. Yeh CY, Chen HH, Tang R, Tasi WS, Lin PY, Wang JY, Surgical outcome after curative resection of rectal leiomyosarcomaDis Colon Rectum 2000 43(11):1517-21.10.1007/BF0223673011089585 [Google Scholar] [CrossRef] [PubMed]
[7]. Momtahen S, Curtin J, Mittal K, Current chemotherapy and potential new targets in uterine leiomyosarcomaJ Clin Med Res 2016 8(3):181-89.10.14740/jocmr2419w26858789 [Google Scholar] [CrossRef] [PubMed]
[8]. Yoldas T, Karaca AC, Ozturk S, Unver M, Calıskan C, Korkut MA, A rare cause of colonic obstruction “colonic intussusception”: Report of two casesCase Rep Surg 2015 2015:46537410.1155/2015/46537425861510 [Google Scholar] [CrossRef] [PubMed]
[9]. Ravi SJC, Adult intussusception- a rare diagnostic and therapeutic dilemmaWorld Journal of Medical and Surgical Case Reports 2017 6:5 [Google Scholar]
[10]. Hamilton AE, Singh A, Austin KK, Shin J, Hong JS, A rare pathological couplet of colocolic intussusception plus cecal bascule in a young adult: A case reportCureus 2018 10(10):e343010.7759/cureus.3430 [Google Scholar] [CrossRef]
[11]. Wilson A, Elias G, Dupiton R, Adult colocolic intussusception and literature reviewCase Rep Gastroenterol 2013 7(3):381-87.10.1159/00035515524163649 [Google Scholar] [CrossRef] [PubMed]