Introduction
Bouveret’s syndrome occurs when a gallstone enters by a bilioenteric fistula and gets impacted in stomach or small intestine causing gastric outlet or small intestinal obstruction. It is a rare type of gallstone ileus that typically occurs in elderly patients with background of multiple co-morbidities [1,2]. Incidence of Bouveret’s syndrome is higher in females, owing to the higher incidence of gallstones in females which is related to the cholestatic effects of female sex hormones [3]. Presence of co-morbidities increases the surgical risk and is associated with higher mortality rate [4]. Because of its rarity and atypical presentation, the diagnosis of Bouveret’s syndrome is often delayed or missed [5]. Diagnosis is made on the basis of clinical presentation, presence of pneumobilia, demonstration of bowel obstruction and visualisation of stones by abdominal imaging [6].
Common presentations are abdominal discomfort or pain associated with nausea and vomiting, anorexia, constipation, and can be uncommonly associated with features of upper gastrointestinal bleed [7]. Common signs are abdominal rigidity, tenderness, distension associated with features of dehydration, obstructive jaundice and fever [7]. Rigler’s triad is characteristic for Bouveret’s syndrome (small intestinal obstruction, ectopic presence of gallstones and pneumobilia) and is seen on plain abdominal radiograph or abdominal Computed Tomography (CT) scan [8]. Though, there has been a significant improvement in the prognosis in last few years, it still causes significant morbidity and mortality estimated at 60% and 12-30%, respectively, due to the older age and co-morbidities [8,9]. Various endoscopic and surgical techniques have been described in the last few years for the treatment of this entity. Here authors described three cases of bouveret’s syndrome with radiological findings and surgical treatment.
Case Series
Case 1
A 62-year-old male patient presented to the Emergency Department with history of midline upper abdominal pain associated with intermittent nausea and vomiting since two weeks. Patient was diabetic and hypertensive since last 10 years, for which he was under treatment. Patient had no significant past surgical history. He was non smoker and had history of occasional alcohol intake since last 25 years. On examination, abdomen was distended. There was generalised tenderness, with sluggish bowel sounds. Patient had taken over the counter oral analgesics. At the time of presentation, patient was dehydrated, his Blood Pressure (BP) was 94/60 mmHg, pulse rate was 110-120 beats per minutes. After resuscitation, patient was admitted in intensive care unit for monitoring and further evaluation. His blood investigations showed, haemoglobin was 11.2 gm%, Total Leucocyte Count (TLC) was 14200/cumm, Erythrocyte Sedimentation Rate (ESR) was 60 mm/hr, C-Reactive Protein Test (CRP) was 18 mg/dL. Nasogastric tube was inserted and gastric aspiration was done. Intravenous fluid and antibiotics were started. After stabilisation, contrast CT scan whole abdomen was done, which showed cholecystoduodenal fistula. Two calcified gall stones of size 6 cm and 2 cm were seen in the proximal jejunum [Table/Fig-1].
a) Computed Tomography (CT) scan abdomen (axial section). Arrow indicates presence of gall stone at proximal jejunum; b) Removed gall stones from jejunum of size 6 cm and 2 cm; c) Longitudinal incision over jejunum and retrieved stone intraoperatively.
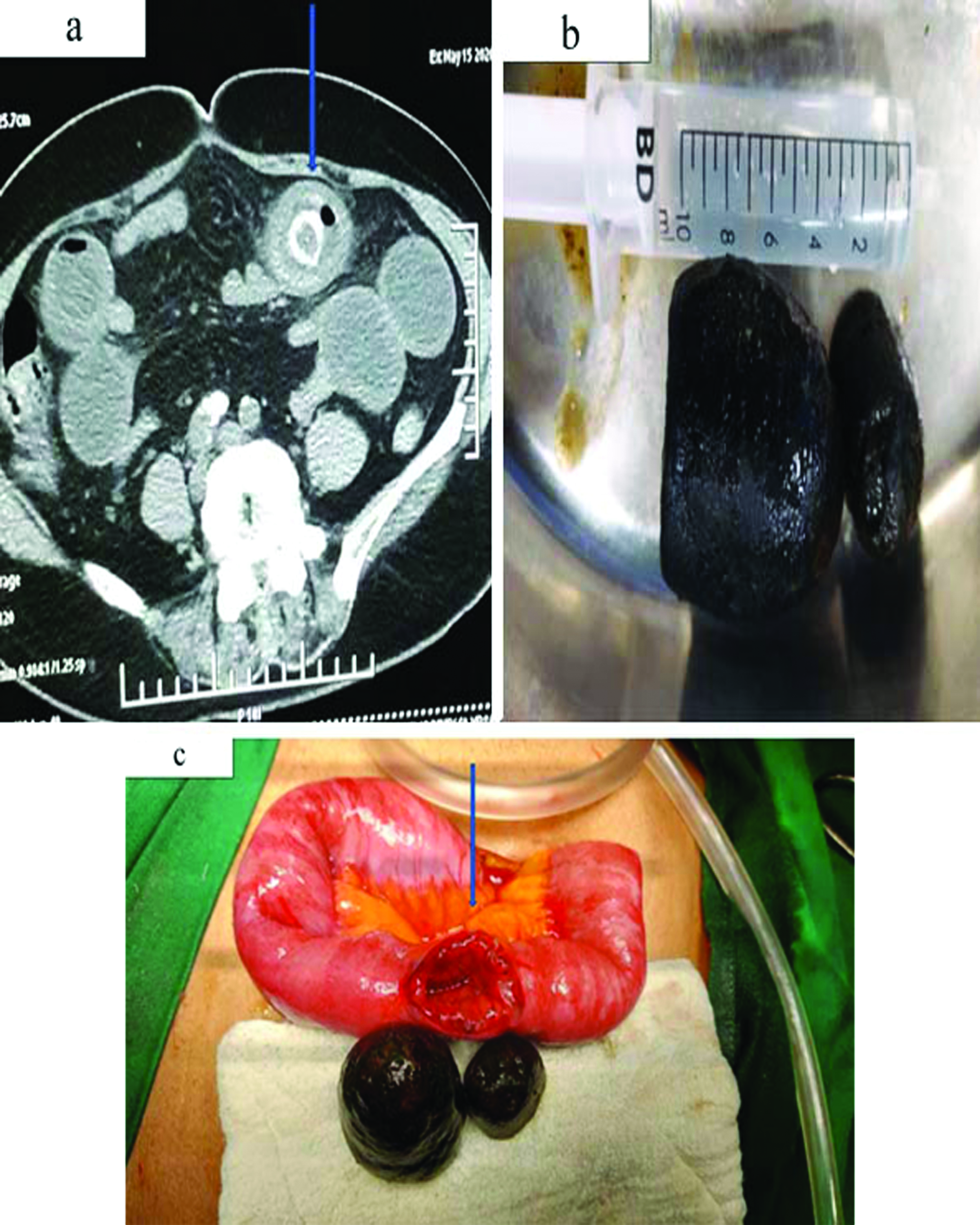
Laparotomy was done by vertical midline incision. Dense adhesions were encountered in the subhepatic space between the gall bladder, omentum and small bowel. Blunt dissection was carried out and cholecystoduodenal fistula was delineated. Lesser sac was opened and the site of jejunal obstruction and stone impaction was identified. Disimpaction of the impacted calculus was attempted by milking but failed. Longitudinal incision was made over the impacted calculus, retrieving both the calculi and the incision was closed transversely in two layers by (3,0) absorbable polyfilament interrupted sutures [Table/Fig-1b,c]. The gall bladder and the fistulous tract were left intact to avoid unnecessary complications. Rest of the viscera was examined for any other gross pathology. A 28 french drain was placed in the lesser sac and abdomen was closed in layers. In the postoperative phase, patient was shifted to ward, within next 24 hours. Oral feeding was started on second postoperative day. On the third postoperative day the inflammatory markers had improved and abdominal drain was removed. Antibiotics were continued for five postoperative days. Following which patient was discharged in apparently asymptomatic condition with uneventful recovery.
Case 2
A 70-year-old obese female patient presented to the department with history of recurrent upper midline and right sided upper abdominal pain since one year. Patient had a history of symptomatic gall bladder stone disease, but had not sought any surgical help for the same. Patient was hypertensive and had history of coronary artery disease since last 12 years, for which she was receiving antiplatelets and antihypertensive agents. This time patient attended the Emergency Department with complaints of recurrent postprandial vomiting associated with intermittent epigastric pain.
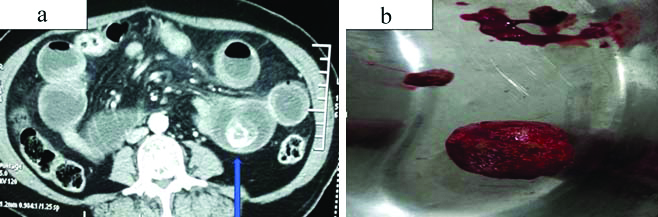
On presentation, patient was in hypovolemic shock (BP was 76/50 mmHg, pulse rate was 130-140 beats per minutes). After resuscitation, patient was shifted to intensive care unit for further evaluation and management. Patient was kept nil per mouth. Nasogastric tube insertion and gastric aspiration was done. Contrast Enhanced Computed Tomography (CECT) whole abdomen showed pneumobilia, signs of mechanical ileus (dilated stomach and proximal duodenum), cholecystoduodenal fistula, large stone of size 4 cm at mid jejunum and inflamed gall bladder [Table/Fig-2a]. Laparotomy was done. After lavage, adhesiolysis and exploration was done meticulously. Migrated stone was noticed at distal jejunum. Stone milked at around 20 cm from duodenojejunal flexure and a small opening was made with successful extraction of stone [Table/Fig-2b]. Primary repair of opening was done with vicryl 2.0. Due to poor general condition of patient, cholecystectomy and fistula repair was not performed. 28 French Romo ADK drain (Romsons abdominal drain) was placed at Hepatorenal Pouch of Morrison (HRPM) and pelvis. Sheath was closed with loop Polydioxanone (PDS) no. 1 and skin with monofilament 2.0. After surgery, patient required ventilation support for two days. Patient was extubated on postoperative day 2 and was shifted toward after 24 hours. Antibiotics were continued for seven days. Patient was discharged in apparently healthy condition on day 7 after removal of both drains.
a) Computed Tomography (CT) scan abdomen (axial section). Arrow indicates presence of gall stone at mid jejunum; b) Retrieved gallstone from jejunum surgically.
Case 3
A 55-year-old female patient presented with a history of midline and right side upper abdominal pain associated with recurrent bilious vomiting since 1-2 days. On examination, patient was pale, febrile (temperature 102o F), severely dehydrated and drowsy. The pulse was weak and thready (120-130 beats per minutes), and BP was 84/60 mmHg. Abdomen was mildly tender over epigastrium and bowel sounds were present. Patient had vast medical history of ischaemic stroke, coronary heart disease, diabetes and hypertension, for which she was taking medications.
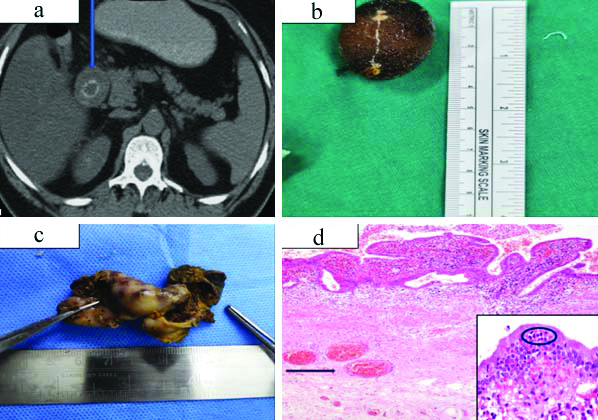
After admission, patient was resuscitated, intravenous fluids, antibiotics, antiemetics and inotropes were started. Blood investigations showed Haemoglobin was 11 gm%, Total Leucocytes Count (TLC) -11000/mm3, ESR was 90 mm/hr, CRP was 42 mg/dL. Urgent CT Abdomen was done, which showed dilated stomach and proximal duodenum with stone in 2nd part of duodenum [Table/Fig-3a]. Diagnosis of bouveret’s syndrome was made. Exploratory laparoscopy was planned. Pneumoperitoneum was done with veress needle and 10 mm trocar placed infraumbilically. Diagnostic laparoscopy revealed purulent collection in liver bed and dense adhesion. Meticulously adhesiolysis was done. Fistula connection noted between gall bladder and proximal duodenum. Gall bladder was resected from fistula and stone was extracted from duodenum using choledocoscope and basket [Table/Fig-3b,c] and was sent for histological examination, which showed features of chronic active cholecystitis [Table/Fig-3d]. On histopathological examination, dense inflammatory cell infiltrate with congestion in the lamina propria and congested blood vessels were observed. Neutrophilic aggregate was present in the lining epithelium.
a) Computed Tomography (CT) scan abdomen (axial section). Arrow indicates gallstone at proximal duodenum; b) Retrieved gallstone from duodenum surgically; c) Resected gall bladder specimen; d) Histopathological examination findings showing dense inflammatory cell infiltrate with congestion in the lamina propria. Arrow highlights congested blood vessels (H&E, 10X). Inset shows neutrophilic aggregate in the lining epithelium (H&E, 40X).
Primary repair of opening done with vicryl 2.0. Gall bladder dissected out from gall bladder fossa and removed from epigastric port with endobag. Lavage was given and 14 French drain was placed in liver bed. Sheath was closed with vicryl no 1 and skin with monocryl 3.0. Postoperatively, patient was shifted to ward on 2nd postoperative day and started tolerating oral feed. Inflammatory markers improved. On 6th postoperative day, patient was discharged with oral antibiotics in asymptomatic state after removal of abdominal drain.
Discussion
Bouveret’s syndrome is a rare type of gallstone ileus caused by passage of gallstone into proximal small bowel by biliary-enteric fistula. Wickbom G notified that it was first reported in 1770 by Beaussier [10]. In 1896 the French physician Leon Bouveret published two cases of gastric outlet obstruction due to gallstone impaction in the duodenal bulb [10,11]. Migration of gallstone to small intestine is seen in less than 1% cases and only 1%-4% cases of small bowel obstruction are associated with gallstone ileus [12]. Most of the reported data suggests that the most common site for stone impaction and obstruction is the terminal ileum [12], although recent case reports and case series mentions proximal bowel as the most common site for stone impaction [Table/Fig-4] [13-17].
Previous publications showing age of presentation and site of stone impaction.
| Author | Type of study | Age of patient (years) | Site of stone impaction |
|---|
| Jin L and Naidu K (2021) [13] | Case report | 91 | Proximal duodenum |
| Kudaravalli P et al., (2020) [14] | Case report | 91 | Proximal duodenum |
| Caldwell K et al., (2018) [15] | Case report | 71 | Gastric antrum |
| Bhattarai M et al., (2016) [16] | Case report | 78 | Proximal duodenum |
| Qasaimeh GR et al., (2014) [17] | Case report | 70 | Proximal duodenum |
Obstruction at other sites is uncommon and occurs in distal jejunum in 9% of cases, colon in 4%, rectum in 4% and at the duodenum in only 1-3% [18]. Early diagnosis and treatment of Bouveret’s syndrome is crucial as the presence of co-morbidities and elderly age group are associated with higher morbidity and mortality [19,20]. Clinical presentation of bouveret’s syndrome is sometimes very non specific, therefore, it is important to consider it as a differential diagnosis in old age patients with history of gallstone disease. In the present case series, all the patients presented at advanced age ranging from fifth to seventh decade. This is in concordance with other case reports published in literature [Table/Fig-4].
Although uncommonly, it has also been reported in relatively younger age group [21]. Radiological evaluation plays a vital role in diagnosing bouveret’s syndrome. Abdominal X-ray is an initial screening tool, but not sufficient enough to diagnose most of the cases [22]. Rigler’s triad (evidence of intestinal obstruction, ectopic presence of gallstone and pneumobilia) is not easily visualised on X-ray in most of the patients. Abdominal sonography can show features of chronic cholecystitis, pneumobilia, dilated stomach and proximal bowel, but locating stone in bowel is difficult in most of the cases, due to presence of gas shadow [23,24]. Abdominal CT scan is diagnostic, as it gives detailed anatomical information about fistulous tract and location of stones in lumen [25]. In the present case series, CT scan was used as a primary diagnostic modality in all the three cases. Literature suggests that CT scan is the gold standard in detection of gallstone ileus [26].
In 15-20% of patients, stones can be isoattenuating and difficult to identify on CT scan. In these cases, Magnetic Resonance Cholangiopancreatography (MRCP) can help to locate stones. Most of the data suggests that endoscopic or percutaneous approach is the initial treatment modality, but success rate is limited because of large size of stone. Still it should be attempted before choosing surgical treatment [24,25]. Despite availability of data showing some success with endoscopic or percutaneous approach, most of the patients require surgery [27]. Most of the recent published data suggests that surgery is the treatment of choice with better success rate [13-17]. Enterolithotomy or gastrotomy is the main surgical treatment for Bouveret’s syndrome [8].
Limited resection is sometimes required, when involved bowel is irreversibly damaged. Cholecystectomy should be done in cases of retained stone to prevent recurrence. Laparoscopic approach should be attempted first, although high conversion rate seen in complicated cases. If the general condition of patient permits, fistula repair and cholecystectomy should be done in the same sitting. In cases with higher expected perioperative morbidity and mortality, fistula repair and cholecystectomy can be planned as a second stage procedure. According to Lowe A et al., in approximately thirty five percent of cases, one stage procedure was performed and fistula repair with cholecystectomy was done at same sitting [28]. Although this approach should be attempted only in patients with good general condition. Till date, no conclusive data is available to compare outcome for both approaches, but most of the recent case reports suggests good outcome of one stage procedure [13-17]. Therefore, if the patient’s general condition permits, cholecystectomy and fistula repair should be done at same sitting. Early presentation in younger age tends to develop more complications postoperatively due to persistent biliaryenteric fistula. Therefore, it is particularly advisable to perform fistula repair in same sitting in younger patients. Authors suggest that surgical treatment (preferably laparoscopic approach) is a preferable and effective treatment strategy for treatment of bouveret’s syndrome, when endoscopic treatment is not available or unsuccessful.
Conclusion(s)
Bouveret’s syndrome is a rare type of mechanical small bowel obstruction secondary to migration of gallstone, which can be fatal if not diagnosed and treated timely. Sometimes diagnosis may be delayed at times due to non specific presentation in a subset of patients. CT scan of abdomen is the investigation of choice in most of the patients. Endoscopic and percutaneous approach is the first line of treatment with limited success. Most of the patients require surgery for stone extraction. Prognosis largely depends on timing of presentation, age of the patient and presence of co-morbidities.
[1]. Koulaouzidis A, Moschos J, Bouveret’s syndrome. Narrative reviewAnn Hepatol 2007 6(2):89-91.10.1016/S1665-2681(19)31937-4 [Google Scholar] [CrossRef]
[2]. Doycheva I, Limaye A, Suman A, Forsmark CE, Sultan S, Bouveret’s syndrome: Case report and review of the literatureGastroenterol Res Pract 2009 2009:91495110.1155/2009/91495119360112 [Google Scholar] [CrossRef] [PubMed]
[3]. Novacek G, Gender and gallstone diseaseWien Med Wochenschr 2006 20:527-33.10.1007/s10354-006-0346-x17103289 [Google Scholar] [CrossRef] [PubMed]
[4]. Doko M, Zovak M, Kopljar M, Glavan E, Ljubicic N, Hochstadter H, Comparison of surgical treatments of gallstone ileus: Preliminary reportWorld J Surg 2003 27(4):400-04.10.1007/s00268-002-6569-012658481 [Google Scholar] [CrossRef] [PubMed]
[5]. Lawther RE, Diamond T, Bouveret’s syndrome: Gallstone ileus causing gastric outlet obstructionUlster Med J 2000 69(1):69-70. [Google Scholar]
[6]. Sans M, Feu F, Panes J, Pique JM, Teres J, Duodenal obstruction by biliary lithiasis (Bouveret’s syndrome)Gastroenterol Hepatol 1996 19(10):519-20. [Google Scholar]
[7]. Jones TA, Davis ME, Glantz AI, Bouveret’s syndrome presenting as upper gastrointestinal haemorrhage without hematemesisAm Surg 2001 67:786-89. [Google Scholar]
[8]. Pickhardt PJ, Bhalla S, Balfe DM, Acquired gastrointestinal fistulas: Classification, aetiologies, and imaging evaluationRadiology 2002 224:09-23.10.1148/radiol.224101118512091657 [Google Scholar] [CrossRef] [PubMed]
[9]. Shah D, Deka H, Chilbule P, Bouveret’s Syndrome: A rare case presentationJournal of Clinical and Diagnostic Research 2018 12(9):PD03-04.10.7860/JCDR/2018/34662.12008 [Google Scholar] [CrossRef]
[10]. Wickbom G, The man behind the syndrome: Leon Bouveret. The internist who supported surgeryLakartidningen 1993 90(3):162-165. [Google Scholar]
[11]. Bouveret L, Pyloric stenosis adherent to a calculusRev Med (Paris) 1896 16:01-16. [Google Scholar]
[12]. O’Neill C, Colquhoun P, Schlachta C, Etemad-Rezai R, Jayaraman S, Gastric outlet obstruction secondary to biliary calculi: 2 cases of Bouveret SyndromeCanadian Journal of Surgery 2009 52(1):E16-18. [Google Scholar]
[13]. Jin L, Naidu K, Bouveret syndrome-A rare form of gastric outlet obstructionJournal of Surgical Case Reports 2021 5:01-03.10.1093/jscr/rjab18334040753 [Google Scholar] [CrossRef] [PubMed]
[14]. Kudaravalli P, Saleem S, Goodman A, Bouveret syndrome as a rare cause of gastric outlet obstructionPROC (BAYL UNIV MED CENT) 2020 33(2):235-23.10.1080/08998280.2019.170884132313470 [Google Scholar] [CrossRef] [PubMed]
[15]. Caldwell K, Lee S, Leggett P, Bouveret syndrome: Current management strategiesClin Exp Gastroenterol 2018 11:69-75.10.2147/CEG.S13206929497323 [Google Scholar] [CrossRef] [PubMed]
[16]. Bhattarai M, Bansal P, Patel B, Lalos A, Exploring the diagnosis and management of Bouveret’s syndromeJNMA J Nepal Med Assoc 2016 54(201):33-35.10.31729/jnma.281427935909 [Google Scholar] [CrossRef] [PubMed]
[17]. Qasaimeh GR, Bakkar S, Jadallah K, Bouveret’s syndrome: An overlooked diagnosis: A case report and review of literatureInt Surg 2014 99:819-23.10.9738/INTSURG-D-14-00087.125437593 [Google Scholar] [CrossRef] [PubMed]
[18]. Reisner R, Cohen J, Gallstone ileus: A review of 1001 reported casesAm Surg 1994 60:441-46. [Google Scholar]
[19]. Frattaroli FM, Reggio D, Guadalaxara A, Illomei G, Lomanto D, Pappalardo G, Bouveret’s syndrome: Case report and review of the literatureHepatogastroenterology 1997 44(16):1019-22. [Google Scholar]
[20]. Joshi D, Vosough A, Raymond TM, Fox C, Dhiman A, Bouveret’s syndrome as an unusual cause of gastric outlet obstruction: A case reportJ Med Case Rep 2007 1:7310.1186/1752-1947-1-7317760995 [Google Scholar] [CrossRef] [PubMed]
[21]. Yang K, Chang C, Bouveret Syndrome: A rare case of instance and treatment in a younger patientHindawi Case Reports in Gastrointestinal Medicine 2020 2020:183738710.1155/2020/183738732257465 [Google Scholar] [CrossRef] [PubMed]
[22]. Trubek S, Bhama JK, Lamkin N, Radiological findings in Bouveret’s syndromeEmerg Radiol 2001 8:335-37.10.1007/PL00011935 [Google Scholar] [CrossRef]
[23]. Lobo DN, Jobling JC, Balfour TW, Gallstone ileus: Diagnostic pitfalls and therapeutic successesJ Clin Gastroenterol 2000 30(1):72-76.10.1097/00004836-200001000-0001410636215 [Google Scholar] [CrossRef] [PubMed]
[24]. Ripollés T, Miguel-Dasit A, Errando J, Morote V, Gómez-Abril SA, Richart J, Gallstone ileus: Increased diagnostic sensitivity by combining plain film and ultrasoundAbdom Imaging 2001 26:40110.1007/s00261000019011441553 [Google Scholar] [CrossRef] [PubMed]
[25]. Pickhardt PJ, Friedland JA, Hruza DS, Fisher AJ, CT, MR cholangiopancreatography, and endoscopy findings in Bouveret’s syndromeAJR Am J Roentgenol 2000 180(4):1033-35.10.2214/ajr.180.4.180103312646450 [Google Scholar] [CrossRef] [PubMed]
[26]. Haddad F, Mansour W, Deeb L, Bouveret’s Syndrome: Literature reviewCureus10(3):e229910.7759/cureus.2299 [Google Scholar] [CrossRef]
[27]. Dumonceau JM, Endoscopic treatment of gastric outlet obstruction caused by a gallstone (Bouveret’s syndrome) after extracorporal shockwave lithotripsyEndoscopy 1997 29(4):319-21.10.1055/s-2007-10041979255539 [Google Scholar] [CrossRef] [PubMed]
[28]. Lowe A, Stephenson S, Kay C, Duodenal obstruction by gallstones. A review of literatureEndoscopy 2005 37:82-87.10.1055/s-2004-82610015657864 [Google Scholar] [CrossRef] [PubMed]