Neck Pain (NP) is a major public health problem with a global prevalence of 288.7 million cases, 65.3 million incident cases [1]. NP is experienced by every individual once in a lifetime, and it affects the individual both at a personal and societal level [2]. In patients with NP, a specific pathoanatomical cause is generally unidentifiable, and this type of NP is commonly labeled as Mechanical Neck Pain (MNP) [3]. It can be defined as pain located in the cervical and shoulder region, with symptoms aggravating with neck movements, neck postures, or on palpation of the cervical musculature [4,5].
Chronic Mechanical Neck Pain (CMNP) patients present with pain, limited cervical range of motion, headache, dizziness, and/or alterations in the sensory-motor system, which affects the individual’s Postural Sway (PS) [6-12]. MNP is called chronic if it persists for more than three months in an individual. It is estimated that patients experiencing the first episode of NP have a 30% possibility of progressing to chronic symptoms [6]. It is reported that the patients who visit the healthcare departments with the first episode of NP have maximum recurring episodes of NP within a year [13].
PS can be measured by analysing oscillations in the Center of Pressure (COP); it represents the body’s ability to maintain balance in an upright position within the given base of support [6]. An altered PS in CMNP patients may be attributed to an altered somatosensory input from the cervical region [12]. Pain may also contribute to an altered PS. It may inhibit muscular input and a dysfunctional central sensory modulation of proprioceptive information from the neuromuscular spindle of cervical muscles [14].
Physiotherapists often use manipulations to improve pain and PS associated with MNP [6,15,16]. In literature, cervical, cervicothoracic junction and Thoracic Spine Manipulation (TSM) have been used to alter pain in patients with CMNP [4,17,18]. However, there have been limited studies that evaluated the effect of manipulation on PS. Few studies have used cervical manipulations for the improvement of PS [6,19,20]. Manipulation of the cervical spine is a high-risk procedure with associated complications like headaches, dizziness and nausea [21]. TSM is safer and is associated with fewer complications than cervical manipulations. It has been hypothesised that the thoracic spine has a biomechanical, anatomical and neural relationship with the cervical spine. Any change in the thoracic spine will bring a difference in the cervical spine [22,23].
Therefore, in the light of the present evidence, this study aimed to analyse the efficacy of multilevel TSM in improving pain and PS in CMNP patients.
Materials and Methods
The quasi-experimental study was carried out from June 2019 to February 2020 at the Outpatient Department (OPD), Department of Physiotherapy, Lovely Professional University, Phagwara, Punjab, India. The patients with age group of 18-29 years (both male and female), who reported in the OPD with a chief complaint of NP, were screened for inclusion and exclusion criteria.
The Institutional Ethics Committee (IEC) of Lovely Professional University approved the study protocol (LPU/IEC/2019/03/14). The patients were informed about the study’s objectives, and they signed a written informed consent before participating in the study. Ethical considerations of the study were as per the World Medical Association Declaration of Helsinki’s. The patients’ participation was entirely voluntary, and the patients could withdraw from the study at any point of time.
Inclusion criteria: The patients were included in the study if they had: (a) NP for more than three months; (b) Elevated pain with neck movements, postural difference of the neck or on palpation of the cervical musculature; and (c) Neck Disability Index (NDI) of ≥10% [24].
Exclusion criteria: Patients were excluded if they: (a) had a history of neurological symptoms; (b) tested positive on Wainner [25] criteria; (c) had a history of a whiplash injury or any cervicothoracic injuries; (d) have received manipulations in the last three months.
The patients were screened for potential red flags and contraindications for spinal manipulative therapy (e.g., vascular disorders, instability, previous history of vertebrobasilar insufficiency, and dizziness or vertigo) before the first manipulation.
Sample size calculation: The sample size was computed using g power software. It was based on F statistic assumption with an effect size of 0.25, alpha error=0.05, and the study power as 85% confidence interval with three measurements.
Primary author did a thorough assessment of study patients before the baseline documentation of the outcome measures. At the initial visit (Day 0), baseline readings were assessed. Interventions were applied on consecutive three days. The outcome measures were evaluated on each visit. Two outcome measures: (1) pain; and (2) PS were used and assessed by the primary author.
The spinal manipulation was applied in three sessions on alternate days with a maximum of three attempts in a session. The intervention was used in a separate room (Physiotherapy OPD) with proper light, and the patients’ privacy was taken into consideration. The primary author performed TSM on the patients. The therapist administering manipulation had four years of experience in treating patients with musculoskeletal conditions. The therapist was a certified manual therapist from the Manual Therapy Foundation of India (MTFI).
The screw thrust technique was used to manipulate the thoracic spine at multiple levels. The method is widely reported in the literature [21,26-28]. The patients were asked to lie in a prone position for the application of the manipulation with their head in the hole of the treatment couch. The therapist stood on the patient’s side in a standing position with crossed hands at the respective zygapophyseal joints. Individuals were asked to perform deep inhalation followed by exhalation; the therapist then applied thoracic thrust at the end of the exhalation at one level, followed by multiple thoracic spine levels. A pop sound was considered a successful thrust, and if a pop sound was not obtained on the first attempt, the technique was repeated for a maximum of three tries in a session.
Outcome Measures
Outcome measures were assessed at four different points of time, i.e., at the baseline (D0), after the first intervention (D1), second intervention (D2), and after the third intervention (D3).
Pain: Pain intensity was assessed using the Numeric Pain Rating Scale (NRS). NRS is an 11-point rating ranging from 0 to 10. Patients were asked to rate their pain on a scale that is in line with the intensity of their current pain level. The Minimally Clinically Important Difference (MCID) for NRS in NP patients was reported to be 1.3 points, and the Minimum Detectable Change (MDC) was reported as 2.5 points; any difference more than these values can be attributed to effects of treatment [29].
Postural Sway (PS): PS is the body’s ability to maintain the Centre of Foot Pressure (COFP) over the given base of support. PS was measured using a WinTrack platform (Win-Track, company-Medicapteurs, n0-12k0022, France). It calculates the sway velocity in millimeters/seconds (i.e., the movement of the COFP) in the anteroposterior (X) and side-to-side (Y) directions. The foot size of the patients were measured before the data acquisition on the force plate. The patients stood quietly on the force platform for 30 seconds with their eyes closed. A bipedal stance was maintained during the recording. The data collected for 30 seconds was recorded at a sample rate of 1200 Hz using monitor data acquisition software (WinTrack Software) [30]. WinTrack is a reliable tool for the measurement of PS and other gait related parameters [31]. The measurement of PS is illustrated in [Table/Fig-1].
Measurement of Postural Sway (PS) on WinTrack force platform (Patients eyes are closed during the testing procedure).

Statistical Analysis
Data analysis was performed with the Statistical Package for the Social Sciences (SPSS) version 25.0 statistical software package. Repeated measures ANOVA was used to analyse the within subject variability for the measured outcome measures. Post-Hoc test was used to assess whether the variations were significant. The significant level was set as 0.05.
Results
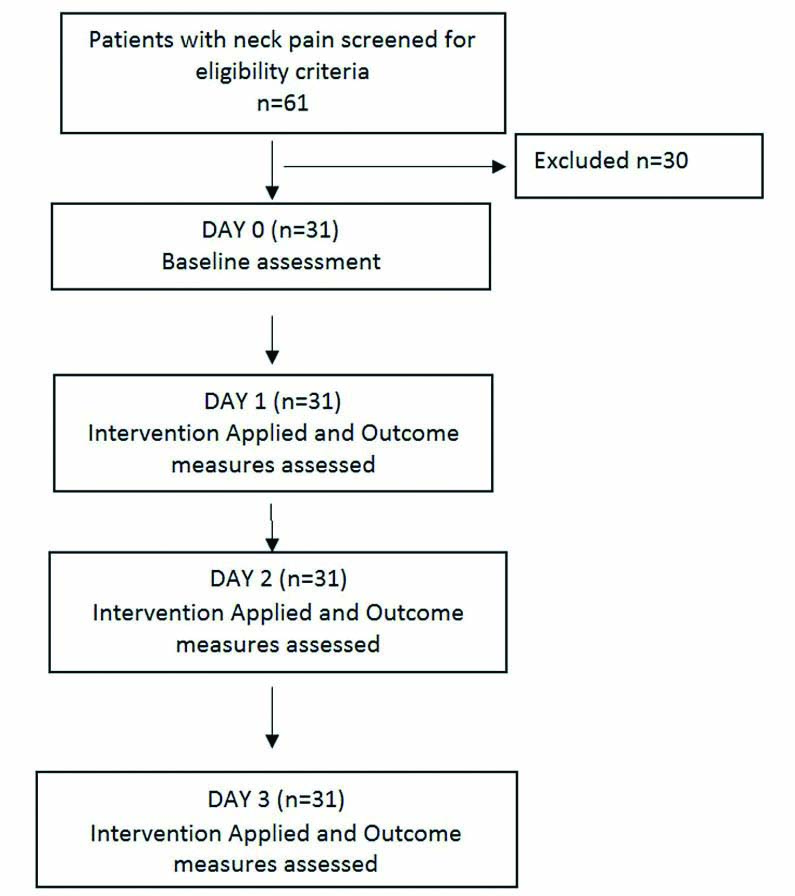
Sixty-one patients with NP were screened for inclusion in the study, out of which 31 patients were selected based on the inclusion criteria. The study’s recruitment and assessment procedure is highlighted in [Table/Fig-2]. Eleven patients were excluded as they had headaches associated with NP, nine patients were excluded as they had radiculopathy, three patients had Temporomandibular Joint (TMJ) dysfunction, and seven individuals declined to receive the treatment. Therefore, 31 patients received TSM, and their data were analysed and reported.
Flow diagram of the study.
The mean age of the patients was 22.23 years (SD=2.667). Nineteen patients were female (61.3%), and 12 were males (38.7%). The mean duration of pain (months) was 19.19 (SD=11.8). The other baseline characteristics are highlighted in [Table/Fig-3].
Baseline demographic characteristics of the included patients.
| Baseline characteristics (n=31) | Mean (SD) |
|---|
| Age (in years) | 22.2 (2.6) |
| Height (in cm) | 160.5 (7.7) |
| Weight (in kg) | 62.1 (13.6) |
| BMI (in kg/cm2) | 24.7 (6.8) |
| Pain duration (in months) | 19.19 (11.8) |
| Foot size (in cm) | 23.5 (1.7) |
| NRS | 6.2 (1.2) |
| Postural Sway (Anteroposterior direction) | 14.3 (5.7) |
| Postural Sway (Mediolateral direction) | 19.3 (10.5) |
BMI: Body mass index; NRS: Numeric pain rating scale
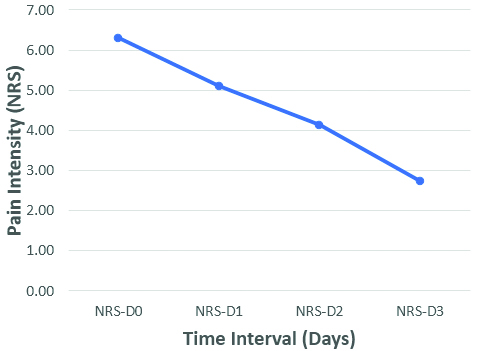
Pain: The repeated measures ANOVA test showed that pain scores were significantly different during atleast one point of time, F (3, 90)=105.8, p<0.05. The post-hoc test revealed that pain intensity decreased significantly from day 0 (baseline) (mean=6.29) compared with day 1 (mean=5.10). NRS scores changed considerably from day 0 to day 2 (mean=4.13). There was also a significant difference from day 0 to day 3 (mean=2.74). The difference in NPRS scores is depicted in [Table/Fig-4].
Graphical representation of mean pain intensity measured using Numerical Rating Scale (NRS: rated from score 0 to 10), x-axis represents the time from baseline to day three and y-axis represents the mean pain intensity.
There were no adverse reaction reported by the patients like “increased pain”, “headache”, “tenderness”, and “dizziness”.
Postural Sway (Anteroposterior Direction)
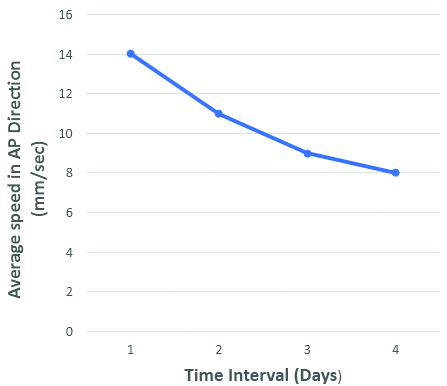
The repeated measure ANOVA indicated a significant difference between the different sway scores in anteroposterior direction, F (3, 90)=3.55, p=0.02. The post-hoc test suggests that there was no significant difference in PS from Day 0 (baseline) (mean=14.33) compared with day 1 (mean=10.73). However, there was a significant difference in PS from day 0 to day 2 (mean= 9.41). Scores were also significantly changed from day 0 to day 3 (mean=8.89) [Table/Fig-5] highlights differences among mean for all the days.
Graphical representation of the Postural Sway (PS) in anteroposterior direction, x-axis represents the time from baseline to day three and y-axis represents the average speed of PS in antero-posterior direction.
Postural Sway (PS) (Mediolateral Direction)
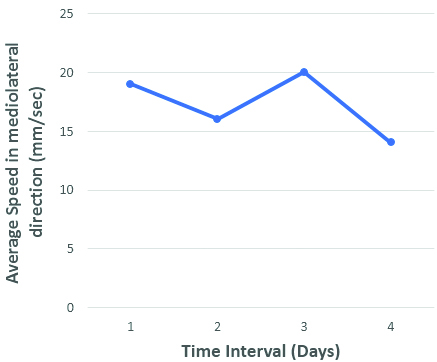
Repeated measures ANOVA showed that there was a significant difference in mediolateral sway during different days of treatment, (F3, 90)=5.10, p=0.03. Post-hoc analysis revealed that there was no significant difference between PS on baseline (day 0) (mean=19.32) and day 1 (mean=16.04). Even between day 0 and day two, there was no significant difference for ML sway among the patients. However, there was a substantial difference between day 0 and day 3 (mean=14.43). Different timeline changes are depicted in [Table/Fig-6].
Graphical repesentation of the Postural Sway (PS) in medio-lateral direction, x-axis represents the time from baseline to day three and y-axis represents the average speed of PS in mediolateral direction.
Discussion
The main findings of the study depict that multilevel TSM results in short-term improvements in self-reported pain and PS among patients with chronic MNP. The results of the study suggest significant reductions in self-reported pain intensity measured on NRS. There was a mean difference of 3.5 (54%) change in NRS scores post intervention. The change in self-reported pain intensity in the present study exceeded the reported MDC of 2.5 and MCID of 1.3 in NP patients [29]. The current study results of decreased pain intensity is homogenous with previous studies done in patients with MNP [4,17,18,21,23,32].
Saavedra-Hernández M et al., demonstrated similar reductions in pain intensity post TSM manipulation among CMNP patients [18]. They suggested that the addition of cervical manipulations to TSM can induce an additional effect on pain relief. They used a supine thrust maneuver whereas the prone multilevel screw thrust technique was used in the current study. Despite different manipulation methods, reductions in pain in both the studies may be due to the neurophysiological mechanisms produced by the manipulation techniques.
Lau HMC et al., observed that TSM was effective in reducing NP [23]. They also used a supine manipulation method and a more extended dosage for TSM. Another report studied the acute effects of TSM on pain and disability among CMNP patients and found a significant reduction of pain at 24 hours and one-week post manipulation by using screw thrust method [21]. The current research has yielded similar results too. However, no additional treatment was administered in this study. The findings may directly be attributed to TSM.
While an exhaustive analysis of the mechanism of the TSM effect on pain is beyond the paper’s scope but some of the aspects are highlighted here. Traditionally, it is believed that manipulation-related results are due to biomechanical alterations. However, recent literature challenges the biomechanical model. The new model suggests that the mechanism by which manipulation modulates pain might be neurophysiological [33,34]. Bialosky JE et al., proposed a new model where they indicated that mechanical force-induced from manual therapy begins a cascade of neurophysiological responses from the peripheral and central nervous system responsible for pain relief [34]. It has been reported that spinal manipulation reduces inflammatory cytokines and expand endorphins release [35]. The other aspect of understanding the pain relief in present study was that authors gave thrust at a distant site from the pain.
There have been various studies reporting reduced pain intensity and sensitivity distant from the site of manipulation [5,22,36-39]. These studies report improvement in pain in sites remote from the area of manipulation. Although the mechanism of TSM resulting in pain reduction in CMNP patients remains unclear, Cleland JA et al., suggested that this could be due to normalisation of biomechanics leading to reduce load and improvements in joint force distribution in the cervical spine. The other plausible mechanism can be that zygapophyseal joints of the cervical and upper thoracic spine have similar pain referral patterns. The activation of mechanoreceptors in the thoracic region might alleviate pain through these pain referrals patterns [3].
The data demonstrates a significant reduction in sway velocity among the patients. The anteroposterior PS improved immediately post-thrust and had a constant decrease on subsequent days. However, mediolateral PS did not show significant change during the first two days, but significant changes were observed on the final day. Although the literature is rich in analysing the role of manipulation on pain, limited studies evaluate the effect of spinal manipulation on PS in CMNP patients.
Romero del Rey R et al., studied the efficacy of manipulating the upper cervical spine and combining the lower cervical spine and TSM on pain and PS [6]. They reported a significant reduction in PS in patients receiving upper CSM. They could not demonstrate an improvement in PS in patients who received a combination of manipulation techniques. Contrastingly, manipulations were applied at every thoracic level and a different technique was used in this study. The other possible reason can be a regular short-term monitoring of the PS, whereas they measured it on only two occasions. Most of the studies have evaluated cervical manipulation effect on PS [6,19,20]. On the contrary, the current study uses a thoracic manipulation that could explain the difference in results from previous studies. Earlier literature demonstrates a reduction in sway velocity after manipulating the peripheral joints [40,41].
The mechanism responsible for improved sway velocity post manipulation in present study can be attributed to three reasons: 1) reduction in pain; 2) improved sensory-motor integration; 3) enhanced proprioception. Haavik H and Murphy B suggest that spinal pain or dysfunction represents a state of altered afferent input responsible for ongoing central plastic changes, resulting in dysfunction and pain [7]. Spinal manipulation is advocated to correct the altered afferent information; this improvement modifies sensorimotor integration that can be considered a reason for changes in the PS post TSM manipulation [7,42]. A significant improvement in sway velocity in the study population is observed.
Present study uses TSM as an intervention. Because of the anatomical relationship of the thoracic spine and the sympathetic chain ganglion, it seems conceivable that intervention may influence peripheral sympathetic outpouring to both the upper and lower quarters [43]. It has been estimated that the thoracic spine and rib cage’s unfriendly neurodynamic versatility and mechanical hypomobility are connected to across-the-board substantial musculoskeletal complaints. The thoracic spine is referred to as the “Cinderella area” of the spine; this may explain results obtained from distant site manipulations away from the site of pain [44]. Objective measurement of PS was the strength of the study.
Limitation(s)
Primarily, the study did not use any additional outcome measures such as range of motion, pain pressure threshold, and pain sensitivity, which would have enabled us to justify the results more comprehensively. The patients were not blinded, which may have resulted to the introduction of bias in the study, although that may have been neutralised as PS was objectively measured. This study had only a single group and thus no comparison was made.
Conclusion(s)
The study demonstrates significant reductions in the pain and PS in CMNP patients. Sway velocity significantly reduced in the present study, indicating that TSM can be used in the patients with CMNP to minimise PS provided there are no contraindications present against manipulation. There were no adverse reactions to the manipulation in the patients. TSM can be used as an alternative to cervical manipulations as it has less risk and adverse events.
BMI: Body mass index; NRS: Numeric pain rating scale