Gold enamel tattooing is a customary practice seen in various clans of Asia and the Indian subcontinent, for ages. The incidence of such cases is very low; hence they can be used as identification marks in forensic sciences and symbols of some tribes and clans. In India, these tattoos or chomps are frequently done by amateurish creatures, making gross harm to the physiology of the tooth and causing consequences like pulp involvement and periapical infection. Here, authors presents a case of 32-year-old male presented with chief complaint of dull, intermittent pain which aggravates with hot stimulus, particularly on taking hot tea and broken upper front teeth because of biting on a hard nut five days back. Patient also complaint of pus discharge over his front teeth for three days. The patient gave the history of gold inking his two maxillary central incisors, ten years back. Pulp damage and periapical lesion was noticed due to enamel inking in upper central incisors. A periapical abscess was resulted due to violation of enamel thickness of the tooth during tooth preparation. In dental clinics, traditional gold tattoos can be done with minimal invasive cavity preparation. Enamel thickness estimation in such cases plays a very important role to safeguard a healthy tooth from the consequences of structural damage.
Dental pulp, Enamel chomps, Enamel thickness, Periapical abscess, Quackery
Case Report
A 32-year-old male patient presented to the Department of Conservative Dentistry and Endodontics, with chief complaint of dull, intermittent pain which aggravated with hot stimulus, particularly on taking hot tea and broken upper front teeth because of biting on a hard nut five days back. Patient also complains of pus discharge over his front teeth since three days.
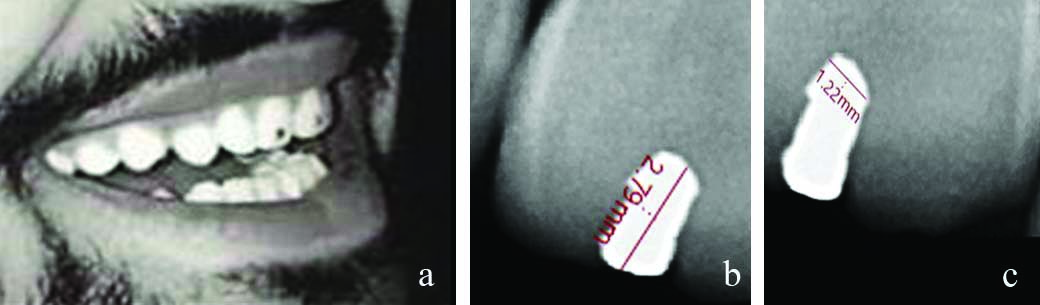
The patient gave the history of gold inking his two maxillary central incisors, 10 years back. Patient had experienced sensitivity to thermal changes and pain for about a month which was relieved on taking medicines when the procedure was done ten years back. For this situation, the father of the patient, who was a goldsmith of the town, also had this tattoo. The grandparents of the patients had also suffered tooth damage due to this practice in past. An enamel chomps was seen on the right central incisor, patient revealed that the left central incisor was also gold inked, which has been dislodged along with his broken tooth fragment, a few days ago. He showed his old photograph with two enamel gold tattoos, which was taken 10 years ago [Table/Fig-1a]. Enamel chomp was seen in the radiograph of the right central incisor. The dimensions of the gold polish tattoo were with depth of 2.79 mm and width of 1.22 mm [Table/Fig-1b,c].
a) Old photograph of the patient with gold enamel tattoos (ten-year-ago); b and c) dimensions of the gold tattoo in right central incisor with depth of 2.79 mm and width of 1.22 mm.
On clinical examination, a small (0.5 mm) nick point was seen along with slightly discolouration (bluish hue) on left central incisor. No extraoral swelling was observed. Pulp vitality test for the left central incisor showed infected and non vital pulp. The left central incisor was tender on percussion and sensitive to hot test done using hot gutta percha point. The periodontal probing was done which revealed no attachment loss. Both the central incisors were firm, with no detectable mobility. The provisional diagnoses of apical periodontitis, periapical granuloma or periapical abscess was made.
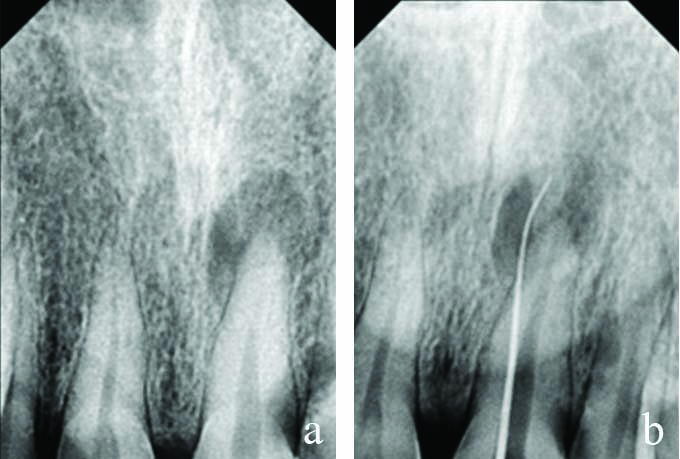
For tracing dental sinus, a sterile gutta percha point was taken and inserted in the sinus tract opening followed by taking an Intraoral Periapical (IOPA) X-ray. On radiograph analysis showed gutta percha points pointed towards the apex of left central incisor. A round localised radiolucency, periapical lesion (2 mm diameter) was observed on the root apex of the left central incisor [Table/Fig-2a,b] (21) along with Ellis class III fracture involving the pulp. Differential diagnosis was made as acute periapical abscess with Ellis class III fracture.
Preoperative Intraoral periapical (IOPA) X-ray of left central incisor showing a) periapical abcess; b) abcess tracking in with gutta percha point.
Root canal treatment was started with isolation of tooth using rubber dam under local anesthesia (lignocaine-1:80,000). Systemic antibiotics were given amoxiclav 625 mg twice a day for 5 days and non steroid anti-inflammatory (tab. ketorolac dt twice a day for 5 days). Metrogyl gel IP 2 % w/w to be applied with an cotton bud locally at the abscess point for 5 days. Expulsion of the gold remnants was done. A triangular shaped access opening was done using round bur on the lingual side of the tooth (placing it at 45° angle). A triangular-shaped canal orifice was refined using a tapered and Endo Z bur. A glide path was created using 6k, 8k, and 10 k files using Ethylene Diamine Tetraacetic acid (EDTA) gel followed by a 15 K file. Pus was drained and the canal was irrigated with normal saline and 3% Sodium hypochlorite (NaOCl), using a side vent irrigation needle. The working length was taken using radiographs and an apex locator (E-Pex Pro, eigtheenth). The biomechanical preparation was done upto 35 k (sequence 20k, 25k, 30k, 35k) file. The canal was dried using paper points and the negative pressure of the syringe. The triple antibiotic paste consisting of metronidazole, ciprofloxacin, and minocycline was placed as intracanal medicament. The access opening was closed using orafill. Patient was recalled after one week.
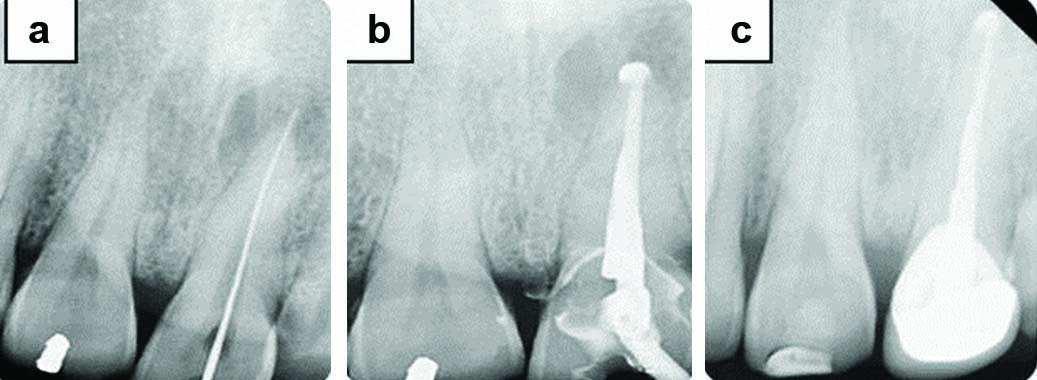
In the second visit, healing of intraoral sinus was clinically observed and no tender on percussion was observed. The temporary restoration was removed and tooth was cleaned and shaped by using Hand Protapers files SX, S1, S2, F1 upto F5, along with 15% EDTA lubrication and irrigation with saline and 3% NaOCL. The triple antibiotic was placed for second consecutive week and tooth was temporarily sealed with orafill. Obturation was planned in the third visit when the patient was totally asymptomatic and no weeping of canal was observed. Thorough cleaning and irrigation of the canal was followed by drying it with paper points and negative pressure of the syringe. Obturation was done using AH plus sealer and Gutta Percha following warm vertical condensation with obturation pen (fast pack, eigtheenth). Sealer puffs were observed. The post-endodontic restoration was finished with composite filling and followed by porcelain fused to metal crown for tooth after 3 weeks of obturation [Table/Fig-3a-c,4].
Intraoral periapical (IOPA) X-ray showing. a) 15k files in canal; b) Obturation with gutta percha points and AH plus sealer; c) Crown in left maxillary central incisor.
Follow-up photograph after crown on left central incisor and composite restoration on right central incisor.

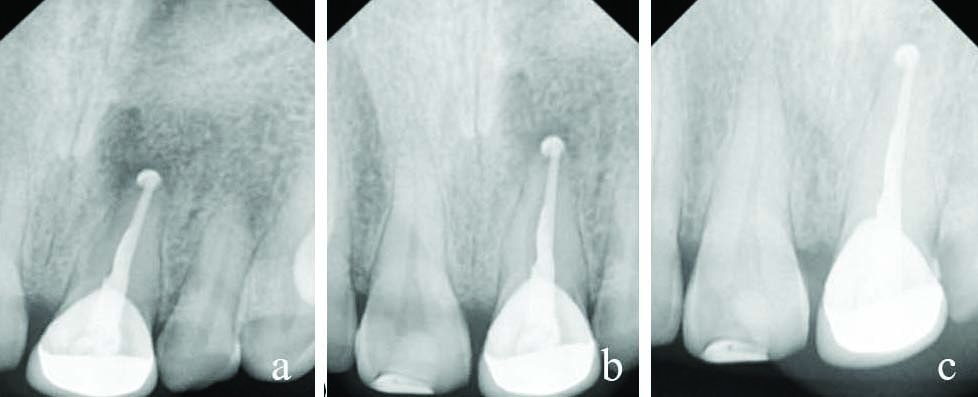
The gold tattoo on right central incisor was removed using airotor and ultrasonic scaler, followed by composite restoration. Further crown was advised for same tooth later. On follow-up of one month, six months and one year, periapical healing was noticed on IOPA X-rays for left central incisor [Table/Fig-5a-c].
Follow-up radiographs and periapical healing in left central incisor. a) after one month; b) after six months; c) after one year.
Discussion
Beauty conceptions, traditional or religious believes [1], have always motivated people to go for tooth jewellery [2], gold enamel inking, and oral piercings [1]. Fossil records of Indian, Chinese, and Mayan civilisations have confirmed the use of tooth adornments in human history [1]. Gold enamel tattoos are likewise a means of enhancing teeth in the Indian subcontinent [2]. The females of Gujjar, Jaat, Yaduvanshi, Thakurs clan are seen as enamored with gold enamel tattoos, done by neighbourhood feruas [1,2]. The cultural and forensic significance is that, due to the prevalence of Gold Enamel tattoos among several tribes and communities may serve as a crucial and important tool for the identification of deceased and forensic investigations in case of mass disasters [3]. Gold inking or tattoos is an exceptionally delicate strategy from tooth physiology and pathology purpose of view [2], as a number of cases have been accounted for in which individuals have their teeth contaminated or damaged [3]. This case was first reported case of enamel inking in a male.
Consequences of gold inking:
a) Pathological: Tooth enamel inking with gold can be the reason for tooth crack, tooth discolouration, sore arrangement, and discharge seepage [4];
b) Physiological: The weakness of these gold enamel tattoos may incorporate pointless loss of finish, dentinal hypersensitivity, and pulp tissue involvement [5];
c) Oral Hygiene issues: The aggregate hindrances of gold tattoos are plaque commitment and carious lesions [4];
d) Dislodgement: Gold enamel tattoos are strategy touchy or technique sensitive and ought to be finished after the essentials of tooth preparation [5].
Traditional method of gold tattooing: In the Indian subcontinent, implanting gold wires after tooth penetrating with sharp instruments is often done by unprofessional or not qualified personals [1,6], which can compromise the physiology of a sound tooth, may result in trauma to the coronal part of the tooth or pulp tissue, causing periapical trauma in later stages [7,8].
Minimal invasive technique: The cavity preparation of the tooth must be within the enamel thickness of the tooth. Overall health and integrity of the tooth should be conserved as much as possible. The enamel thickness of the tooth can be calculated with the help of preoperative radiographs and digital radiography software [6]. As per Sturdevant, enamel thickness at the incisal ridges of incisors is 2 mm approximately, and it gets thinner towards cementoenamel junction, tooth anomalies like amelogenesis imperfecta and non carious lesions like attrition, abrasion affects the enamel thickness [8]. This estimated enamel thickness from radiography can be transferred and marked over the enamel cutting burs. The end cutting bur (Shofu, F41.6S) can be used as an initial cavity punch-out, followed by straight bur (marked with estimated enamel thickness). William’s probe can be used as a measuring, transferring, and marking tool for enamel thickness. The cavity depth should be kept slightly lesser than the estimated enamel thickness, to avoid dentinal sensitivity. The walls of the cavity should be parallel or slightly converging and cavity varnish should be applied on the cavity floor [5]. Gold can be compacted in the prepared cavity after degassing and using the compaction technique for direct gold fillings [5,8].
In recent literature, many cases have been reported for enamel tattoos. Suhas S and Kumar A reported two cases of enamel tattoos with different patterns [9]. Kumar A and Hemant S gave an insight into the forensic importance, instrumentation, and technique used in the traditional practice of enamel inking, and the myths behind this practice [10]. Hans M et al., discussed the importance of the enamel chumps as an identification trait in forensic studies [11]. Yadav R et al., reported two cases of enamel chumps in females of the same family, which was done at their teenage [1]. Kotechaa SD et al., reported the enamel inking in 11-year-old male child.
In this case, the triple antibiotic paste was used in between the visits as root canal medicament, as it helps in regeneration and periapical healing of the lesions. As a necrotic and pulpless tooth has no blood supply, local application of the antibiotic paste is more advantageous over systemic antibiotics [12]. As the possible route of the periapical lesion was through the chronic pulpal necrosis due to the ill method of drilling holes in the tooth, which caused weakening of tooth structure and periapical infection over the years. It can be classified as a primary endodontic lesion [13] as the tooth has moderate and dull pain and periapical radiolucency was seen radiographically. Periodontal probing pocket depth was also not much [7]. Hand Protapers were used with the crown down technique, as it is faster and less debris extrusion occurs as compared to K files, also it maintains the shape of the apical third of the canal [6]. Periapical healing of the lesion was observed over the follow-up visits after 1 month, 6 months, and 1 year. No or little disappearance of sealer puff was noted in radiographs. AH plus sealer also has antibacterial properties, and unintentional sealer puffs cause no pain and harm to the periapical tissues [7].
Conclusion(s)
The gold enamel inking can cause irreversible damage to tooth and may result in irreversible pulp and periapical lesions. The pros and cons of the enamel inking should be explained to patient before hand. Minimal invasive cavity preparation is necessary to avoid any unwanted consequences and patients should be encouraged to get the same by dentist.
[1]. Yadav R, Yadav A, Rai R, Pahuja M, Solanki S, Gold tooth tattoos: Identifying features in forensic odontologyJ Clin Diagn Res 2016 10(7):ZJ08-09.10.7860/JCDR/2016/21441.820927630974 [Google Scholar] [CrossRef] [PubMed]
[2]. Kotechaa SD, Hedgea YD, Chaudhrya K, Yelurib R, Masiha U, Singhaa C, Gold enamel choumps- a case reportEgyptian Journal of Forensic Sciences 2016 6(3):303-06.10.1016/j.ejfs.2015.05.002 [Google Scholar] [CrossRef]
[3]. Jethi N, Arora KS, Forensic endodontics and national identity programs in IndiaIndian J Dent Res 2020 31:662-65.10.4103/ijdr.IJDR_187_1933107475 [Google Scholar] [CrossRef] [PubMed]
[4]. Bhatia S, Arora V, Gupta N, Gupta P, Bansal M, Thakar S, Tooth jewellery- its knowledge and practice among dentists in Tricity, IndiaJ Clin Diagn Res 2016 10(3):ZC32-35.10.7860/JCDR/2016/18578.744127134997 [Google Scholar] [CrossRef] [PubMed]
[5]. Garg N, Garg A, Textbook of operative dentistry 2018 4th edNew DelhiJaypee Brothers [Google Scholar]
[6]. Oberoi SS, Oberoi A, Growing quackery in dentistry: An Indian perspectiveIndian J Public Health 2015 59(3):210-12.10.4103/0019-557X.16466126354397 [Google Scholar] [CrossRef] [PubMed]
[7]. Ilan R, John I, Ingle’s Endodontics 2019 7th editionPMPH USA [Google Scholar]
[8]. Gopikrishna V, Sturdevant’s art and science of operative dentistry- South Asian Edition 2013 [Google Scholar]
[9]. Suhas S, Kumar A, ‘Choump’ enamel tattoosJ Forensic Odontostomatol 2007 25:61-62. [Google Scholar]
[10]. Kumar A, Hemant S, Choumps-enamel tattoos revisitedJ Forensic Odontostomatol 2009 27:81-88.10.1038/sj.bdj.2011.73021904339 [Google Scholar] [CrossRef] [PubMed]
[11]. Hans M, Nagpal A, Shetty S, ChoumpsBr Dent J 2011 211:194 [Google Scholar]
[12]. Mohammadi Z, Jafarzadeh H, Shalavi S, Yaripour S, Sharifi F, Kinoshita JI, A review on triple antibiotic paste as a suitable material used in regenerative endodonticsIran Endod J 2018 13(1):01-06. [Google Scholar]
[13]. Shenoy N, Shenoy A, Endo-perio lesions: Diagnosis and clinical considerationsIndian J Dent Res 2010 21:579-85.10.4103/0970-9290.7423821187629 [Google Scholar] [CrossRef] [PubMed]