Combined Effects of Thermotherapy along with Scapular Muscles Strengthening in Cervical Radiculopathy: A Case Report
Shaikh Mohammad Aeraj1, Tajuddin Chitapure2
1 Intern BPT, Department of Musculoskeletal Physiotherapy, MGM School of Physiotherapy, (A Constituent Unit of MGMIHS, Navi Mumbai), Aurangabad, Maharashtra, India.
2 Assistant Professor, Department of Musculoskeletal Physiotherapy, MGM School of Physiotherapy, (A Constituent Unit of MGMIHS), Aurangabad, Navi Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Tajuddin Chitapure, MGM School of Physiotherapy, N-6, CIDCO, Aurangabad-431001, Maharashtra, India.
E-mail: taj.chitapure@mgmsop.edu.in; tajchitapure@gmail.com
Cervical radiculopathy is a syndrome in which the patient complains of pain on the right scapular border along with sensorimotor deficits. This syndrome commonly develops due to compression of the cervical nerve roots. This report describes the case of 52-year-old histopathology laboratory technician who developed cervical radiculopathy due to prolonged cervical forward flexion while working on his table. The patient also complained of pain on the right scapular border. Radiographic analysis showed cervical spondylosis having osteophyte formation on spinous process of C2, C3, C4, C5 and C6 vertebras. Neural tissue tension test was positive for median nerve. He was treated consecutively with strengthening for shoulder abductors, shoulder adductors, scapula elevators and scapular protractors along with thermotherapy. His right medial border scapular pain and symptoms of cervical radiculopathy decreased in severity after the seventh day of treatment. Although the authors cannot suggest a cause and effect relationship, this report allows for initial hypothesis development that thermotherapy approach may have clinical merit. Future studies in the form of well-designed, randomised clinical trials should be performed to evaluate the effectiveness of this approach in patients with cervical radiculopathy.
Neck disability index, Numerical pain rating scale, Resistive training, Thera tubes, Thermotherapy
Case Report
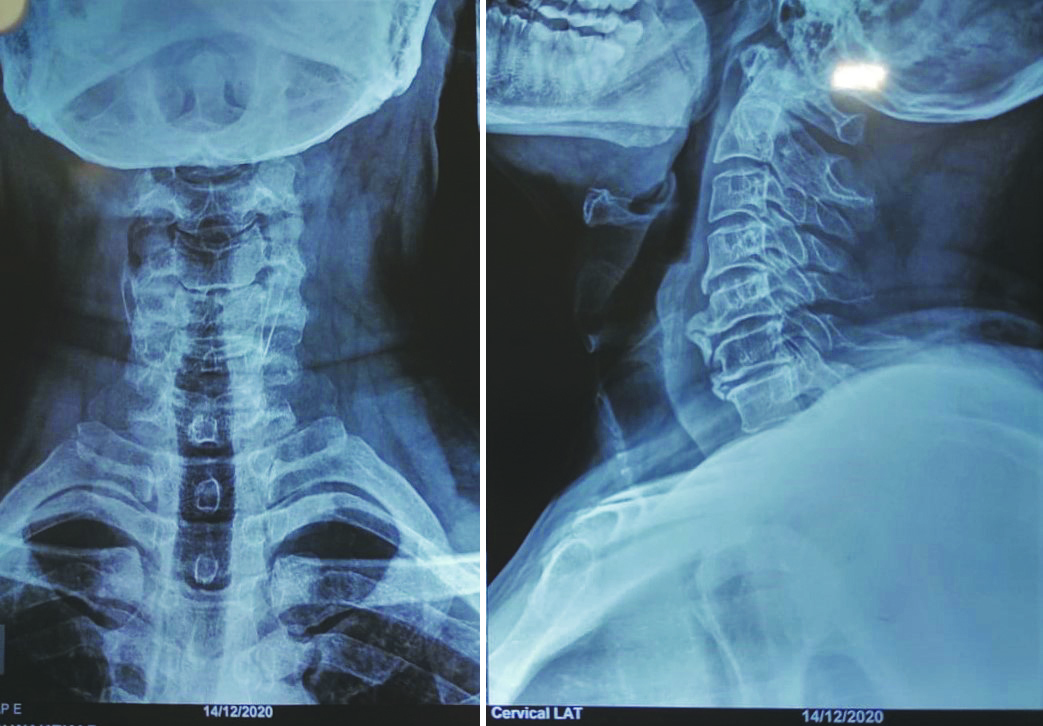
A 52-year-old man, right hand dominant individual with hypothyroidism visited the Outpatient Department (OPD) with a chief complaint of pain on the medial border of his right scapula for the last two days. The pain on the right scapular border was deep, acute and its nature was continuous with a dull aching quality. According to him, he was doing some exercises in the morning without any weights after which he started to experience pain. The onset of pain was sudden. On the same day, in the evening, he started to experience tingling sensation in his right third and fourth digits along with a feeling of heaviness in his right arm. He visited an Orthopaedic consultant who prescribed him some medications and advised for an X-ray. The X-ray showed ossification from C2, C3, C4, C5 and C6 cervical vertebrae [Table/Fig-1].
Radiograph showing ossification (C2, C3, C4, C5, and C6) of cervical vertebrae.
As a histopathology technician, he has to do a lot of rotatory movements with his right arm. He works for about 2-3 hours daily as well as he has to forward flex his neck while working on samples.
On observation of posture in lateral view, a prominent forward head posture was seen and in posterior view, right shoulder elevation was seen. On palpation, there was presence of tenderness along the right scapular region.
The intensity of pain on initials in caps (NPRS) was nine out of ten. On assessment of the range of motion of the cervical spine, all the active and passive range of motions i.e., cervical forward flexion, side flexion, rotation and extension were incomplete and painful while shoulder active and passive range of motions were complete and pain-free. Manual muscle testing of cervical, scapular and shoulder muscles showed a grade 4 out of 5, according to the Medical Research Scale (MRC) for muscle strength grading [1]. The resisted isometrics of the same muscles were powerful but weak. Passive intervertebral accessory movements showed the C4 and C5 cervical vertebrae to be hypomobile. While the upper limb nerve tension test for the right hand showed involvement of median nerve as symptoms were elicited in 60 degrees of elbow flexion. Neck Disability Scores of the patient were 14 out of 50 with 28% disability according to the scale [2]. After detailed assessment and reviewing the investigations, it was concluded that the patient had cervical radiculopathy.
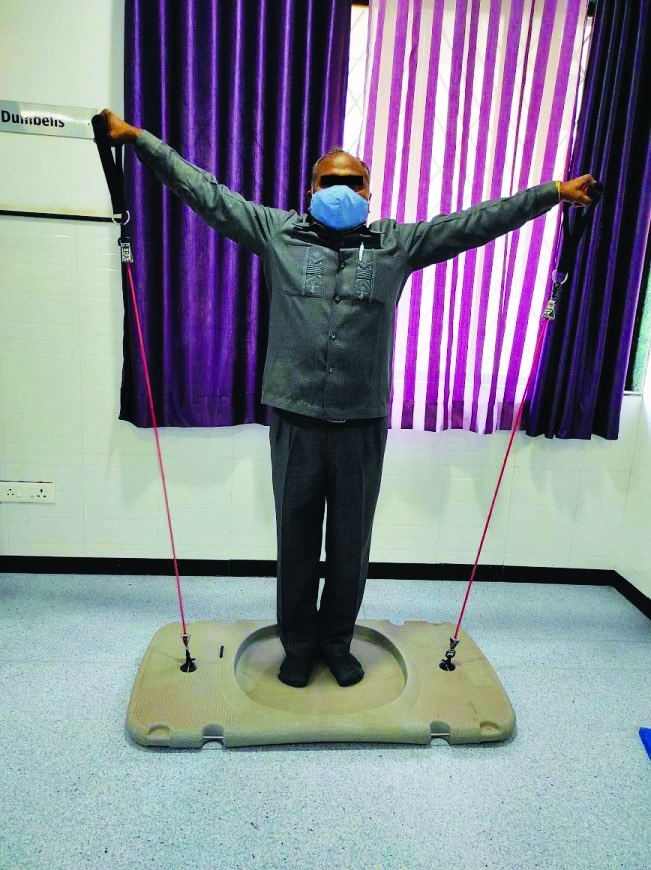
While designing the treatment protocol, it was made sure that no conventional therapy will be used. The protocol included hot moist pack and strengthening of shoulder and scapular muscles only. The patient was advised to visit the OPD for seven consecutive days. Hot moist pack was applied to the neck and upper back patient for 20 minutes. After that, the patient was made to do scapular protractions, scapular retractions, shoulder shrugs and lateral arm raises for three sets of ten repetitions each with the help of Thera tubes. Additionally, patient was advised to take hot moist pack at home as well [Table/Fig-2,3 and 4]. After one week, the patient was advised with the same protocol for home program and was called for a follow-up after the next one week.
Shoulder protractors strengthening.

Shoulder adductors strengthening.

Shoulder abductors strengthening.
After 14 days of continuous treatment, the pain scoring of the patient on NPRS was 1. The scoring on neck disability index was 2 i.e., 4% disability [Table/Fig-5]. There were no significant changes in power of the muscles.
Pre and post-treatment outcome of neck disability index.
| Pretreatment scoring | Post-treatment scoring |
|---|
| Section | Scoring | Section | Scoring |
|---|
| Pain intensity | 5 | Pain Intensity | 1 |
| Personal care (washing, dressing, etc.,) | 2 | Personal care (washing, dressing, etc.,) | 0 |
| Lifting | 1 | Lifting | 1 |
| Work | 2 | Work | 0 |
| Headache | 0 | Headache | 0 |
| Concentration | 1 | Concentration | 0 |
| Sleeping | 1 | Sleeping | 0 |
| Driving | 0 | Driving | 0 |
| Reading | 1 | Reading | 0 |
| Recreation | 1 | Recreation | 0 |
Discussion
Cervical radiculopathy is a syndrome in which the patient complains of pain along with sensorimotor deficits. This syndrome commonly develops due to compression of the cervical nerve roots [3]. Although the prognosis of this condition is quite favourable, a detailed and systematic assessment followed by a standardised rehabilitation is advised to minimise unnecessary investigations and a quicker way for the patient to get back to the activities of daily living [4]. As there is constant development in the literature regarding cervical radiculopathy, medical experts are able to find new and improved ways for diagnosing and treating the condition [5].
Rhee J et al., stated in their study that regardless of the involvement of the cervical nerve root, the patient might complain of upper trapezial and intrascapular pain [6]. The serratus anterior, rhomboids major and minor, levator scapulae and trapezii constitute the “scapular stabilisers”. This group of muscles work on the principal of synergist co-contraction, so that the scapula is anchored on the thorax and the movement is guided [7]. A study by Schory A et al., confirms that the ideal position for strengthening of scapular stabilisers is the standing position as the upper trapezius is least active while performing exercises in supine, prone or side lying [8]. Hence, in this patient exercises were administered in standing position. According to a study conducted by Malanga GA et al., heat therapy induces pain relief, increases blood flow, improves metabolism and increases the overall elasticity of shortened connective tissue as well as a common and effective electrotherapeutical technique used in providing relief for chronic as well as acute types of pain [9].
Cleland JA et al., advocates the prescription of scapular stabiliser strengthening combined with cervical traction as an effective way to rehabilitate cervical radiculopathy [10]. Moezy A et al., stated that strengthening of scapular stabilisers is effective in treating shoulder impingement syndrome, nonspecific neck pain, shoulder pain and adhesive capsulitis [11]. Strengthening of lower trapezius has a positive effect on the scapular tipping in diabetic frozen shoulder [12]. However, there is no literature which shows the effect of scapular strengthening alone in cervical radiculopathy. With reference to above, the authors decided to use a protocol which included use of hot moist pack and shoulder-scapular muscle strengthening. After a continuous one-week session, the results were surprising as the authors did not expect the protocol to be so much effective that the pain of the patient reduced to a significant extent.
Conclusion(s)
There is a lot of literature present which supports use of conventional physical therapy for the management of cervical radiculopathy, however there is no research which supports the strengthening of scapular stabilisers and moist pack alone for the treatment of cervical radiculopathy. This can lead to a new approach for treating an age-old syndrome.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 12, 2021
Manual Googling: Apr 14, 2021
iThenticate Software: May 06, 2021 (9%)
[1]. Larson ST, Wilbur J, Muscle weakness in adults: Evaluation and differential diagnosisAmerican family physician 2020 101(2):95-108. [Google Scholar]
[2]. Khan I, Sivaganesan A, Archer KR, Bydon M, McGirt MJ, Nian H, Does neck disability index correlate with 12-month satisfaction after elective surgery for cervical radiculopathy?. Results from a national spine registryNeurosurgery 2020 86(5):736-41.10.1093/neuros/nyz23131268151 [Google Scholar] [CrossRef] [PubMed]
[3]. Caridi J, Pumberger M, Hughes A, Cervical radiculopathy: A reviewHSS Journal ® 2011 7(3):265-72.https://doi.org/10.1007/s11420-011-9218-z23024624 [Google Scholar] [CrossRef] [PubMed]
[4]. Polston D, Cervical RadiculopathyNeurologic Clinics 2007 25(2):373-85.10.1016/j.ncl.2007.01.01217445734 [Google Scholar] [CrossRef] [PubMed]
[5]. Onks C, Billy G, Evaluation and treatment of cervical radiculopathyPrimary Care: Clinics in Office Practice 2013 40(4):837-48.10.1016/j.pop.2013.08.00424209721 [Google Scholar] [CrossRef] [PubMed]
[6]. Rhee J, Yoon T, Riew K, Cervical radiculopathyJournal of the American Academy of Orthopaedic Surgeons 2007 15(8):486-94.10.5435/00124635-200708000-0000517664368 [Google Scholar] [CrossRef] [PubMed]
[7]. Paine R, Voight M, The role of the scapulaJournal of Orthopaedic & Sports Physical Therapy 1993 18(1):386-91.10.2519/jospt.1993.18.1.3868348140 [Google Scholar] [CrossRef] [PubMed]
[8]. Schory A, Bidinger E, Wolf J, Murray L, A systematic review of the exercises that produce optimal muscle ratios of the scapular stabilisers in normal shouldersInternational Journal of Sports Physical Therapy 2016 11(3):321 [Google Scholar]
[9]. Malanga GA, Yan N, Stark J, Mechanisms and efficacy of heat and cold therapies for musculoskeletal injuryPostgraduate Medicine 2015 127(1):57-65.10.1080/00325481.2015.99271925526231 [Google Scholar] [CrossRef] [PubMed]
[10]. Cleland JA, Whitman JM, Fritz JM, Palmer JA, Manual physical therapy, cervical traction, and strengthening exercises in patients with cervical radiculopathy: A case seriesJournal of Orthopaedic & Sports Physical Therapy 2005 35(12):802-11.10.2519/jospt.2005.35.12.80216848101 [Google Scholar] [CrossRef] [PubMed]
[11]. Moezy A, Sepehrifar S, Dodaran MS, The effects of scapular stabilisation-based exercise therapy on pain, posture, flexibility and shoulder mobility in patients with shoulder impingement syndrome: A controlled randomised clinical trialMedical Journal of the Islamic Republic of Iran 2014 28:87 [Google Scholar]
[12]. Kirthika V, Bhavani P, Rajalaxmi V, The effect of combining scapular stabilisation techniques with conventional physiotherapy in improving range of motion and functional ability in subjects with phase II adhesive capsulitis of the shoulder jointTJPRC: Journal of Physiotherapy & Occupational Therapy 2015 1(1):25-23. [Google Scholar]