Split Hand/Foot Malformation with Long Bone Deficiency: A Report of Two Female Siblings
Mohammed Ali Al-Shehab1, Ahmed Saleh Hudna2, Fahd Naji Thawaba3, Farouk Abdulrahman Al-Qadasi4
1 Senior Specialist, Department of Paediatrics, University of Science and Technology Hospital, Sana’a, Yemen.
2 Assistant Professor, Department of Paediatrics, University of Science and Technology, Sana’a, Yemen.
3 Consultant, Department of Radiology, University of Science and Technology Hospital, Sana’a, Yemen.
4 Postgraduate, Department of Statistics, International Organisation of Migration, Sana’a, Yemen.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mohammed Ali Al-Shehab, Al-Steen Street, Sana’a, Yemen.
E-mail: dr.m.alshehab@gmail.com
Spilt Hand/Foot Malformation with Long bone Deficiency (SHFMLD) is a rare heterogeneous group of limb malformations characterised by absence/hypoplasia and/or median cleft of hands and/or feet associated with long bone abnormalities, most frequently tibia. This case report described two sisters with congenital limb defects born to healthy consanguineous parents. The six-year-old girl did not had both radii and the left fibula. There was a cleft in the left hand and the right foot. She had one digit in her right upper limb, but did not have the left foot. The four-year-old girl had four short limbs, bilateral tibial aplasia with single digit in all limbs. Both parents were normal, and no other similar cases were reported in the family. According to the authors’ best knowledge, these two cases are the first published cases in Yemen with SHFMLD, but they need a genetic study to determine their genetic profile.
Consanguinity, Ectrodactyly, Lymph malformation, Yemen
Case Report
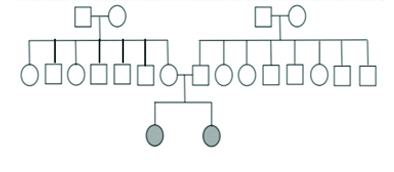
Two sisters aged six years and four years were referred to the Paediatrics department for evaluation and diagnosis. They did not have any illness at the time of their visits to the hospitals. The girls parents (30-year-old father and 25-year-old mother) were healthy and were first cousins by relation with no other affected children or relatives. [Table/Fig-1] illustrates the family pedigree. The mother had no history of complicated pregnancy, drug use during pregnancy or postnatal complications. The affected patients were born by normal vaginal delivery.
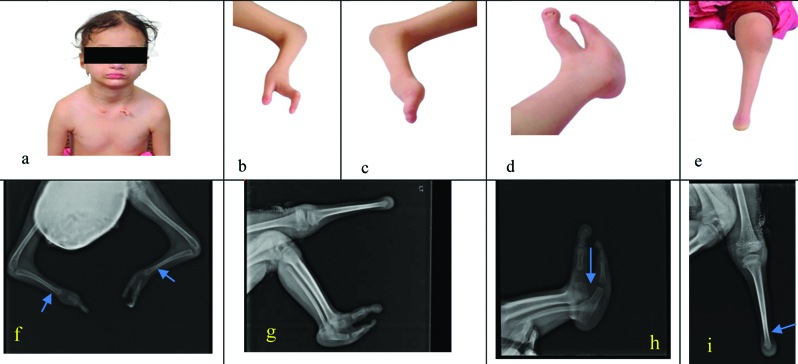
The older sibling, a six-year-old girl was suffering from short stature (height 102 cm), underweight (weight 13 kg) and microcephaly (head circumference 48 cm). She had low-set deformed ears, normal eyes and nose, complete absence of lower teeth, deficient upper teeth (one incisor, two canines, and two molars), and two tags on her neck. Physical examination showed normal hearing and vision as well as normal mental status. Her chest, heart, abdomen and back looked normal. Furthermore, developmental milestones were appropriate for her age. She also had a single digit in the right hand as well as a thumb and deformed-index finger in the left hand. Her forearms were short with contracture of elbows. The right foot had a split malformation between big and little toes and the left foot was absent with a short limb (acromelia). Remaining digits of the upper and lower limbs had hypoplastic nails [Table/Fig-2]. The radiographic image of the upper limbs revealed aplasia of radial bones and undeveloped carpal bones related to her age. There was a single axis of the right-hand bones including the first metacarpus and phalange. Regarding the left hand, the radiographic image demonstrated two-formed adjacent axes of thumb and index, and the index was associated with pointed second-distal phalange at its anterior end. Moreover, there was a bilateral delayed growth of distal humerus’s apophysis and olecranon process. The lower limb radiographic image showed aplasia of the left fibula with absent foot bones. Two formed leg bones on the right side were associated with an abnormal distal tibiofibular joint and a long distal part of fibula that forms abnormal articulation with calcaneum. Radiographic features of the left foot showed two opposing first and fifth metatarsals and phalanges with a cleft in between. Absence of the second, third and fourth metatarsals with phalanges was also seen [Table/Fig-2]. Ultrasound of the abdomen was normal.
a) SHFMLD in a six-year-old girl. Note severe clinical findings of SHFMLD: (b) lost three fingers, (c) monodactyly, (d, h) split-foot malformation, (e) short limb. Radiological findings include: (f) bilateral absent radii and (g,i) absent left fibula with acromelia.
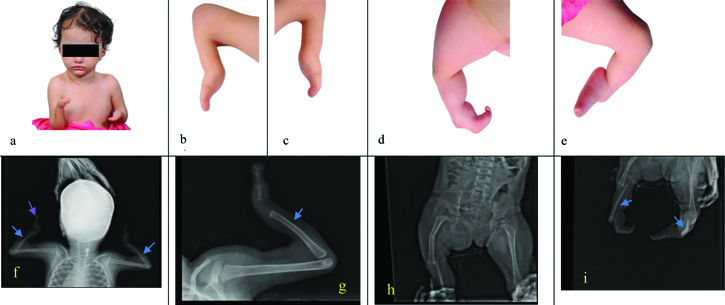
The second sibling, a four year-old girl was with anthropometric features revealing short stature (height 74 cm), underweight (weight 8 kg) and microcephaly (head circumference 47 cm). There were no facial dysmorphic features. The physical examination showed normal hearing, vision, chest, heart, abdomen and back. In addition, the developmental milestones were appropriate for her age. The upper and lower limbs examination revealed single digit with hypoplastic nail in each limb, short forearms, elbow contractures, medial rotation of foot and left knee contracture [Table/Fig-3]. The radiographic findings showed the following: absent radii on both upper limbs, single axis of both the hands including metacarpals and proximal phalanges with non developed carpal bones and deficiently formed wrist joint. Bilateral tibial aplasia with a very short angulated left fibula (mesomelia) and a formed right fibula with missing proximal or distal bones was present in lower limbs. This patient also had a bilateral single axis of foot bones, undeveloped middle and distal phalanges of big toes, and deficient tarsal bones. Furthermore, there were bilateral non developed ankle and knee joints, right developmental dysplasia of the hip, and a short femur with a secondary green stick fracture in the the middle aspect of the femur [Table/Fig-3]. Abdominal ultrasound was normal.
SHFMLD in a four-year-old girl. Note severe clinical findings of SHFMLD: (a-e) abnormal single axes with short limbs. Radiological findings: (f, g) bilateral absent radii, (h, i) bilateral absent tibiae and short left fibula.
The two cases were diagnosed based on the clinical and radiological findings. The differential diagnosis was fibular agenesis with ectrodactyly [1]. The genetic and molecular analysis was not performed for these cases, as they were not available in Yemen. The cases were referred to other specialised centers for multiple procedures (orthopaedic, cosmetic, and plastic) and for rehabilitation, but their parents could not afford the cost due to the family low socio-economic status.
Discussion
Split Hand/Foot Malformation (SHFM) occurs in 1 per 8500-25000 newborns [1] while the incidence of SHFMLD is 1 per million live births [2]. SHFM or ectrodactyly is a rare congenital limb malformation with variable phenotypes. Although it varies from short or abnormal shaped digits to the most severe forms with monodactyly, the classic features are clefts due to lost or undeveloped central three digital rays of the hands and/or feet [1,3,4]. SHFMLD is a rare form of isolated nonsyndromic SHFM associated with a long bone deficiency, usually tibia or femur. It is also considered syndromic SHFM if associated with extra limb manifestations [1]. The diagnosis of these syndromes is generally based on clinical findings, but the genetic tests are needed for confirmation. The high-resolution chromosome analysis and the genome-wide array Comparative Genomic Hybridisation (CGH) are the initial steps for genetic diagnosis. Further studies for mutational analysis are needed especially for the syndromal SHFM [1]. Although no specific genetic cause for SHFMLD has yet been elucidated, three gene loci have been proposed. Gene locations for SHFMLD1, SHFMLD2 and SHFMLD3 are 1q42.2 q43, 6q14.1 and 17p13.3 respectively [4]. Multidisciplinary management, including reconstructive surgery in multiple stages and genetic counseling, is the current practice for the management of SHFM [5].
Congenital malformations including SHFM increase with consanguinity [6-8]. Arab populations including Yemenis comprises one of the highest rates of consanguineous marriages (20-50%) in the world, which increased the risk of autosomal recessive and multifactorial disorders [7]. For instance, a study in United Arab Emirates (UAE) indicated that 23 cases with SHFMLD were from 10 consanguineous marriages [2]. Moreover, two Yemeni cases having SHFM with hearing loss from consanguineous families were reported in a Saudi case report and known to be autosomal recessive [9]. Here, authors reported two Yemeni sisters with SHFMLD who were born from a consanguineous couple. This increased occurrence of SHFMLD in consanguineous families might indicate pseudodominance [2] or autosomal recessive inheritance [7]. Genetic studies from many reports showed that the SHFMLD is predominantly inherited as an autosomal dominant, but autosomal recessive or sporadic inheritance disorders were also reported in few cases [1,2,10]. Normal phenotype in other family members could be due to the incomplete penetrance of SHFMLD [2]. In this report, the normal phenotype in parents could be attributed to the incomplete penetrance or sporadic mutation. Unfortunately, no genetic studies have been conducted in Yemen to determine the genetic profile of these two cases.
It was observed in this report that the patients’ mother had no history of pre-natal drug use or obvious chemical exposure. However, the reported girls were born in a qat-growing area, which is an amphetamine-like substance chewed by many people and needs many chemicals during its cultivation. Pre-natal drug or chemical exposure might increase the risk of congenital malformations in the offspring [8].
Clinical manifestations of SHFMLD can vary within the same family [2,11,12]. Long bone defects are most frequently affecting tibia and rarely affecting other bones such as radius, femur or fibula [12-14]. These two cases had bilateral complete radial agenesis, left fibular aplasia in the older girl and bilateral tibial aplasia in the younger one. Radial abnormalities were reported in another study in Brazil [15] and complete radial agenesis was observed in the two cases in France [11]. Other limb abnormalities, such as ectrodactyly, absent carpal/tarsal bones, aplasia of one or more metatarsal/metacarpals or phalanges, were identified in these two reported cases and in one other report from UAE [2]. Extra-limb malformations associated with SHFMLD like ectodermal dysplasia or cleft lip/palate were reported in other studies in literature [2,11], but the two patients in this report did not have any such malformations. Normal neuro development was obvious in these two cases as in many other reported cases [11-14].
Conclusion(s)
To conclude, this is the first report on two patient sisters of consanguineous Yemeni parents, with clinical and radiological manifestations of SHFMLD. Genetic diagnosis for SHFMLD is important for the family, but unfortunately there are no specialised centers in Yemen for conducting such studies.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Dec 16, 2020
Manual Googling: Mar 23, 2021
iThenticate Software: May 31, 2021 (8%)
[1]. Gurrieri F, Everman DB, Clinical, genetic, and molecular aspects of split-hand/foot malformation: An updateAm J Med Genet A 2013 161(11):2860-72.10.1002/ajmg.a.3623924115638 [Google Scholar] [CrossRef] [PubMed]
[2]. Naveed M, Nath SK, Gaines M, Al-Ali MT, Al-Khaja N, Hutchings D, Genomewide linkage scan for split–hand/foot malformation with long-bone deficiency in a large Arab family identifies two novel susceptibility loci on chromosomes 1q42. 2-q43 and 6q14. 1Am J Hum Genet 2007 80(1):105-11.10.1086/51072417160898 [Google Scholar] [CrossRef] [PubMed]
[3]. Carter TC, Sicko RJ, Kay DM, Browne ML, Romitti PA, Edmunds ZL, Copy-number variants and candidate gene mutations in isolated split hand/foot malformationJ Hum Genet 2017 62(10):877-84.10.1038/jhg.2017.5628539665 [Google Scholar] [CrossRef] [PubMed]
[4]. Yang X, Lin X, Zhu Y, Luo J, Lin G, Genetic analysis of a congenital split-hand/split-foot malformation 4 pedigreeMol Med Rep 2018 17(6):7553-58.10.3892/mmr.2018.883829620206 [Google Scholar] [CrossRef] [PubMed]
[5]. Guero S, Holder-Espinasse M, Insights into the pathogenesis and treatment of split/hand foot malformation (cleft hand/foot)J Hand Surg (European Volume) 2019 44(1):80-87.10.1177/175319341880737530380990 [Google Scholar] [CrossRef] [PubMed]
[6]. Shawky RM, Elsayed SM, Zaki ME, El-Din SMN, Kamal FM, Consanguinity and its relevance to clinical geneticsEgyptian J Medical Hum Genet 2013 14(2)10.1016/j.ejmhg.2013.01.002 [Google Scholar] [CrossRef]
[7]. Tadmouri GO, Nair P, Obeid T, Al Ali MT, Al Khaja N, Hamamy HA, Consanguinity and reproductive health among ArabsReproductive Health 2009 6(1):1710.1186/1742-4755-6-1719811666 [Google Scholar] [CrossRef] [PubMed]
[8]. Ashi M, Assur R, Awan B, Aljaaly H, Bilateral split hand foot malformation in siblings: Case seriesInt J Surg Case Reports 2018 44:114-17.10.1016/j.ijscr.2017.12.03029499514 [Google Scholar] [CrossRef] [PubMed]
[9]. Shamseldin HE, Faden MA, Alashram W, Alkuraya FS, Identification of a novel DLX5 mutation in a family with autosomal recessive split hand and foot malformationJ Med Genet 2012 49(1):16-20.10.1136/jmedgenet-2011-10055622121204 [Google Scholar] [CrossRef] [PubMed]
[10]. Babbs C, Heller R, Everman DB, Crocker M, Twigg SR, Schwartz CE, A new locus for split hand/foot malformation with long bone deficiency (SHFLD) at 2q14. 2 identified from a chromosome translocationHum Genet 2007 122(2):191-99.10.1007/s00439-007-0390-717569090 [Google Scholar] [CrossRef] [PubMed]
[11]. Petit F, Andrieux J, Demeer B, Collet LM, Copin H, Boudry-Labis E, Split-hand/foot malformation with long-bone deficiency and BHLHA9 duplication: Two cases and expansion of the phenotype to radial agenesisEuropean J Med Genet 2013 56(2):88-92.10.1016/j.ejmg.2012.11.00223202277 [Google Scholar] [CrossRef] [PubMed]
[12]. Paththinige CS, Sirisena ND, Escande F, Manouvrier S, Petit F, Dissanayake VHW, Split hand/foot malformation with long bone deficiency associated with BHLHA9 gene duplication: A case report and review of literatureBMC Medical Genetics 2019 20(1):10810.1186/s12881-019-0839-231200655 [Google Scholar] [CrossRef] [PubMed]
[13]. Petit F, Jourdain AS, Andrieux J, Baujat G, Baumann C, Beneteau C, Split hand/foot malformation with long-bone deficiency and BHLHA9 duplication: Report of 13 new familiesClinl Genet 2014 85(5):464-69.10.1111/cge.1221923790188 [Google Scholar] [CrossRef] [PubMed]
[14]. Armour CM, Bulman DE, Jarinova O, Rogers RC, Clarkson KB, DuPont BR, 17p13. 3 microduplications are associated with split-hand/foot malformation and long-bone deficiency (SHFLD)European J Hum Genet 2011 19(11):1144-51.10.1038/ejhg.2011.9721629300 [Google Scholar] [CrossRef] [PubMed]
[15]. Ullah A, Gul A, Umair M, Ahmad F, Aziz A, Wali A, Homozygous sequence variants in the WNT10B gene underlie split hand/foot malformationGenet Molecular Biolol 2018 41(1):01-08.10.1590/1678-4685-gmb-2016-016229384555 [Google Scholar] [CrossRef] [PubMed]