A Case of Large Bowel Obstruction- An Unusual Cause in a Middle Aged Female
Subhransu Kumar Hota1, Vedavyas Mohapatra2, Nageswar Sahu3, Pranati Misra4, Urmila Senapati5
1 Assistant Professor, Department of Pathology, Kalinga institute of Medical Science, Bhubaneswar, Odisha, India.
2 Consultant, Department of Gastrointestinal Surgery, Kalinga institute of Medical Science, Bhubaneswar, Odisha, India.
3 Associate Professor, Department of Pathology, Kalinga institute of Medical Science, Bhubaneswar, Odisha, India.
4 Associate Professor, Department of Pathology, Kalinga institute of Medical Science, Bhubaneswar, Odisha, India.
5 Professor and Head, Department of Pathology, Kalinga institute of Medical Science, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Subhransu Kumar Hota, Assistant Professor, Department of Pathology, Kalinga institute of Medical Science, Bhubaneswar, Odisha, India.
E-mail: subhhota1985@gmail.com
Endometriosis is a disease seen among women in reproductive age group. It is characterised by deposition of endometrial tissue outside the uterus. It commonly involves the pelvic organs like ovary, fallopian tube and pelvic ligaments. Involvement of gastrointestinal tract by endometriosis is uncommon and the incidence varies widely among different studies. Colonic endometriosis can be confused with malignancy both clinically and radiologically. In these instances, histopathology is essential for a correct diagnosis. Here, the authors report a case of colonic endometriosis presenting with features of large bowel obstruction in a 49-year-old female with previous history of laparoscopic hysterectomy. Radiological scanning of abdomen and colonoscopic examination were suspicious of sigmoid malignancy. Although colonic biopsy was inconclusive and tumour markers were normal, she underwent sigmoidectomy with lymph node clearance as per oncological principles with primary anastomosis. The final histopathological examination revealed features of colonic endometriosis without any evidence of malignancy. Detailed evaluation of the patient did not reveal endometriosis at any other site. Patient was discharged after full surgical recovery and was doing well till the last follow-up.
Colonic endometriosis, Colonoscopy, Histopathology, Hysterectomy
Case Report
A 49-year-old female from Eastern Odisha presented to the Surgery Out Patient Department (OPD) with chief complaints of colicky pain of moderate to severe intensity in the left lower abdomen since last six months with associated loss of weight and altered bowel habits. She had no co-morbidities or intake of hormone replacement therapy. She had undergone laparoscopic hysterectomy for dysfunctional uterine bleeding one year back. The detailed histopathological reports were not available with her.
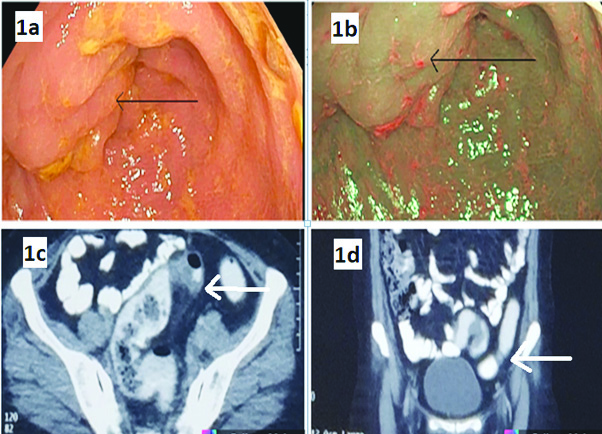
Patient's general physical and systemic examinations were normal. Her blood investigations (routine haematological and biochemical) including Carcino-Embryonic Antigen (CEA) were within normal limits as 1.07 ng/mL (normal <2.5 ng/mL). Colonoscopy showed presence of nodular and infiltrative mucosa at 30 cm from anal verge with luminal narrowing [Table/Fig-1a,b]. Rest of the colon looked normal. Contrast Enhanced CT scan (CECT) of abdomen revealed short segment sigmoid stricture with luminal narrowing [Table/Fig-1c,d] and not associated with lymphadenopathy. Colonoscopic biopsy of sigmoid stricture was inconclusive as biopsy was too superficial containing only normal looking surface epithelium and lamina propria.
a) Colonoscopy showing presence of nodular and infiltrative mucosa at 30 cm from anal verge with luminal narrowing; b) Narrow band imaging of infiltrative mucosa shows no abnormal area; c) Transverse section of CECT abdomen shows short segment wall thickening with luminal narrowing in sigmoid colon; d) Coronal section of CECT abdomen showing similar findings.
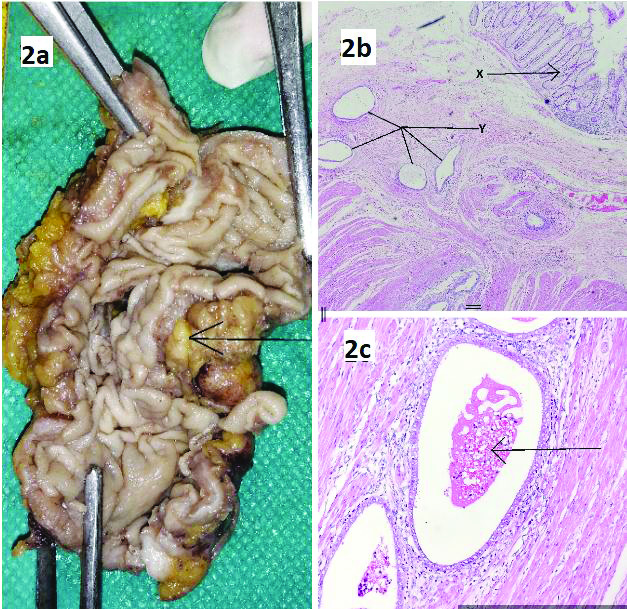
The clinical diagnosis made was carcinoma colon with a differential diagnosis of Gastrointestinal Stromal Tumour (GIST). Due to suspicion of malignancy, she underwent sigmoidectomy with lymphadenectomy as per oncological principles with primary anastomosis. Gross examination revealed a segment of large intestine measuring 9.0 cm in length. There was a constricted segment of 3.0 cm length with normal surface mucosa. On cut section of constricted part, it showed a nodule measuring 2.5 cm diameter just beneath the mucosa [Table/Fig-2a]. Eleven pericolic lymph nodes were isolated. Tissue sections showed normal looking colonic mucosa. The submucosa, muscularispropria and serosa showed nodules of endometrial glands and stroma. Haemorrhage and haemosiderin laden macrophages were seen in the lumen of endometrial glands [Table/Fig-2b,c]. There was no evidence of malignancy. Lymph nodes showed reactive change without any tumour deposit. Postoperative course of the patient was uneventful and she was discharged on day seven and was free of symptoms after surgery. Follow-up of the patient for 12 months revealed no symptoms and she was doing well.
a) Cut open specimen of sigmoid colon showing constriction site and a firm well-circumscribed nodule below normal appearing mucosa; b) X- Microscopic sections from this nodule revealed normal colonic surface epithelium and crypts [H&E,100X], Y-The submucosa, muscularis propria and subserosa contained endometrial glands and stroma [H&E,100X]; c) Endometrial glands cystically dilated with haemorrhage and haemosiderin laden macrophages inside the lumen [H&E,400X].
Discussion
Endometriosis is defined as the presence of normal endometrial mucosa at ectopic site that is outside the uterus. It is commonly seen in 3rd decade of life, affecting 5-12% of women in child bearing age group. Depending on the sites involved, endometriosis is divided as endopelvic or extrapelvic [1-3]. The endopelvic ectopic sites are located in the minor pelvis, the ovaries, the fallopian tubes and the uterosacral ligaments, whereas, the more unusual extrapelvic sites are the abdominal wall, scars of the perineum, the urinary and gastrointestinal tract, the thorax and the nasal mucosa [4]. Extragenital pelvic endometriosis describes in a more accurate way as endometriotic lesions involving pelvic organs such as rectum, sigmoid, and bladder [5].
Gastrointestinal tract is involved in 3.8%-37% of women diagnosed with endometriosis and intestinal obstruction is seen in 7%-23% of these cases [6,7]. Among different parts of gastrointestinal tract most common site is sigmoid colon followed by rectum, ileum, appendix, and caecum [8]. This higher incidence in rectosigmoid area of intestine (close to the uterus) supports the theory of implantation due to retrograde menstruation. Endometrial tissue is implanted through the fallopian tubes to these sites, because of their proximity to uterus [2]. Implants of endometrial tissue typically involves the intestinal wall from the serosa inwards [3].
Symptoms of bowel wall endometriosis usually depend on the site affected and the depth of the invasion [2]. Most cases of gastrointestinal endometriosis are asymptomatic [9]. Symptoms of bowel endometriosis can be non specific and present with dysmenorrhea, dyspareunea or common gastrointestinal complains. However, any pelvic symptoms, if cyclical in nature should raise the suspicion of endometriosis [3]. Acute mechanical intestinal obstruction is a rare complication seen in cases with severe small bowel involvement or sclerosing and fibrotic reaction leading to dense pelvic adhesion movements [2,9]. As colonic endometriosis does not have any specific symptoms, it can easily be confused as irritable bowel syndrome, inflammatory bowel diseases or even malignancy [7]. The findings like intestinal wall thickening on radio imaging and adhesive mass lesion during operative procedure simulates malignancy as happened in our case. Colonoscopic biopsy can be helpful in excluding malignancy, but the biopsy must be deep enough. Usually, these cases are advised for radical resection and subjected to histopathology for diagnostic confirmation [7]. In most of the cases, laparoscopy or laparotomy with histopathological examination remains the only way to resolve the dilemma of diagnosis [10]. Management requires a team approach and follow-up. Hormonal therapy may improve symptoms but, does not prevent the progression of the disease. Surgery is the choice of treatment for intestinal endometriosis, when there are symptoms as intestinal obstruction, bleeding, and severe pain and if malignancy is suspected. Surgical resection of the affected bowel seems necessary in cases suspicion of malignancy as done in the present case. Total abdominal hysterectomy and bilateral salpingo-oophorectomy at the time of bowel resection should be considered only in perimenopausal women and women who do not desire fertility [2].
Although endometriosis is a common problem in the women in the reproductive age group, this case is a rare case of extrapelvic endometriosis with sigmoid colon being the only site of involvement. Exhaustive preoperative workup with CECT and colonoscopic biopsy and intraoperative assessment were suggestive of malignancy but the final histopathology report of endometriosis was a surprising finding.
Conclusion(s)
In case of reproductive women with pain in the abdomen and radiology showing features of bowel obstruction differential of endometriosis should be kept in mind. Extensive multidisciplinary approach should be done to reach the final diagnosis. Clinical, radiological and pathological concordance is necessary. Small biopsy may not help in diagnosis many times, so, histopathological examination is essential to reach final diagnosis of colonic endometriosis.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Mar 27, 2021
Manual Googling: Apr 28, 2021
iThenticate Software: May 03, 2021 (14%)
[1]. Giudice LC, Kao LC, EndometriosisLancet 2004 364:1789-99.10.1016/S0140-6736(04)17403-5 [Google Scholar] [CrossRef]
[2]. Charatsi D, Koukoura O, Ntavela I, Chintziou F, Gkorila G, Tsagkoulis M, Gastrointestinal and urinary tract endometriosis: A review on the commonest locations of extrapelvic endometriosisAdvances in Medicine 2018 2018:346120910.1155/2018/346120930363647 [Google Scholar] [CrossRef] [PubMed]
[3]. Habib N, Centini G, Lazzeri L, Amoruso N, El Khoury L, Zupi E, Bowel endometriosis: Current perspectives on diagnosis and treatmentInt J Womens Health 2020 12:35-47.10.2147/IJWH.S19032632099483 [Google Scholar] [CrossRef] [PubMed]
[4]. Simoglou C, Zarogoulidis P, Machairiotis N, Porpodis K, Simoglou L, Mitrakas A, Abdominal wall endometrioma mimicking an incarcerated hernia: A case reportInt J Gen Med 2012 5:569-71.10.2147/IJGM.S3290422807645 [Google Scholar] [CrossRef] [PubMed]
[5]. Markham SM, Carpenter SE, Rock JA, Extrapelvic endometriosisObstetrics and Gynecology Clinics of North America 1989 16(1):193-219.10.1016/S0889-8545(21)00147-9 [Google Scholar] [CrossRef]
[6]. Rana R, Sharma S, Narula H, Madhok B, A case of recto-sigmoid endometriosis mimicking carcinomaSpringerplus 2016 5:64310.1186/s40064-016-2221-627330909 [Google Scholar] [CrossRef] [PubMed]
[7]. Buldanlı MZ, Özemir A, Yener O, Dölek Y, A rare case of acute mechanical intestinal obstruction: Colonic endometriosisTurkish Journal of Trauma & Emergency Surgery 2020 26(1):148-51. [Google Scholar]
[8]. Bergqvist A, Extragenital endometriosis. A reviewEur J Surg 1992 158:07-12. [Google Scholar]
[9]. Prystowsky JB, Stryker SJ, Ujiki GT, Poticha SM, Gastrointestinal Endometriosis: Incidence and Indications for ResectionArch Surg 1988 123(7):855-58.10.1001/archsurg.1988.014003100690113382351 [Google Scholar] [CrossRef] [PubMed]
[10]. Zhang C, Sun Y, Zhang D, Sun Y, Recurrent symptoms of gastrointestinal tract caused by isolated endometriosis in a middle-aged femaleInternational Journal of Colorectal Disease 2016 31:1511-13.10.1007/s00384-016-2522-926838017 [Google Scholar] [CrossRef] [PubMed]