Subareolar Abscess in an Adult Male Mimicking Carcinoma Breast
Uma Kumar1, Annu Nanda2, Udita Singhal3, Pooja Jain4
1 Consultant Pathologist, Department of Pathology, Balaji Action Cancer Institute, Delhi, India.
2 Professor, Department of Pathology, ESIC Dental College and Hospital, Rohini, Delhi, India.
3 Associate Professor, Department of Pathology, ESIC Dental College and Hospital, Rohini, Delhi, India.
4 Medical Officer, Department of Pathology, ESIC Dental College and Hospital, Rohini, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anu Nanda, Room No. 307, Professor and Head, Department of Pathology, ESIC Dental College and Hospital, Rohini, Delhi, India.
E-mail: annunanda@rediffmailcom
Anucleate squames, Fine needle aspiration, Malignancy, Unusual presentation
Dear Editor,
Subareolar abscess generally occurs in young females, but it is extremely rare in males. Since, breast carcinomas in males arises in the subareolar region, it is important to differentiate between benign and malignant lesions in this areas [1,2].
Authors describe a case of male breast swelling clinically mimicking malignancy, diagnosed as subareolar abscess on Fine Needle Aspiration Cytology (FNAC). A-52-year old male presented with a painful swelling in the left breast for last 15 days. The swelling was progressively increasing in size. The patient was a non-smoker, non-diabetic and gave a negative history of trauma, nipple piercing, any iatrogenic procedure, tubercular infection and medical treatment. On inspection, overlying skin was red and there was no nipple discharge. On palpation, there was a firm, well defined, tender mass measuring 3×2 cm in subareolar region in left breast [Table/Fig-1]. No palpable regional lymphadenopathy was noted.
Clinical image showing a subareolar breast swelling in a male patient.

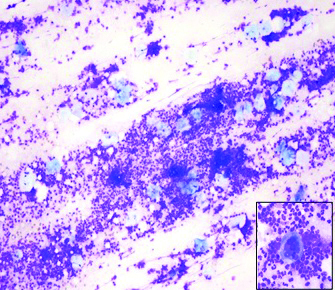
Haematological investigations revealed polymorphonuclear leucocytosis. Liver function tests, kindey function tests and random blood sugar were within normal limits. FNAC, performed with a 22 gauge needle yielded 0.5 mL pus, which was smeared, fixed and stained with Giemsa and Ziehl-Neelson (ZN) stain. Microscopic examination of the stained slide revealed a highly cellular smear with a predominance of neutrophils along with few nucleated squamous cells, anucleated squames and histiocytes. Occasional foreign body giant cells were also seen [Table/Fig-2]. Background showed granular debris. No evidence of malignant cells was noted. ZN stain for acid-fast bacilli was negative. A diagnosis of subareolar abscess was rendered. The patient was given a course of broad spectrum antibiotics. The swelling reduced after two weeks of medication.
Smear showing dense acute inflammatory infiltrate along with scattered anucleated squames (Giemsa, 20X) and inset showing a multinucleated giant cell (Giemsa, 20X).
Zuska JJ et al., first described subareolar abscess in female breast in 1951 [3]. There is squamous metaplasia of major lactiferous ducts or congenital anomalies of ductal system which causes keratin plugging and then abscess formation. It can open through the skin and can cause a discharging sinus [1,3]. Subareolar abscess in male breast is very rare and very few case reports are published in literature. Diabetes and cigarette smoking are strongly associated with abscess formation in males [4]. But in present case, the patient was a non-diabetic and a non-smoker. Treatment strategy includes incision and drainage with broad spectrum antibiotics. Some patients respond to antibiotics only and do not require drainage, as was observed in present case. However, recurrence is reported [1,2].
Diagnostic cytological features for subareolar abscess are-presence of anucleate squames associated with dense acute on chronic inflammation and occasional foreign body giant cell as seen in present case [4]. Various breast lesions in the subareolar region containning benign and metaplastic squamous cells are epidermoid cyst, pilomatrixoma, papilloma, syringomatous adenoma, fibroadenoma, phyllodes tumour, medullary carcinoma and most commonly gynecomastia. Subareolar abscess can mimic inflammatory breast carcinoma clinically, so cytology smears should be carefully screened for any atypical cells. Malignant squamous cells can occasionally be seen in fibroadenomas, phyllodes tumour and primary squamous cell carcinoma of breast [1,4].
Fine needle aspiration is a simple and cost effective tool to differentiate between these lesions. Pathologists and clinicians should be aware of this entity, so that unnecessary surgery can be avoided.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 25, 2021
Manual Googling: May 04, 2021
iThenticate Software: May 31, 2021 (13%)
[1]. Silverman JF, Raso DS, Elsheikh TM, Lannin D, Fine-needle aspiration cytology of a subareolar abscess of the male breastDiagn Cytopathol 1998 18(6):441-44.10.1002/(SICI)1097-0339(199806)18:6<441::AID-DC11>3.0.CO;2-H [Google Scholar] [CrossRef]
[2]. Rajaram ST, Kini H, Rau AR, Pai RR, Subareolar abscess in the male breastDiag Cytopathol 2008 36(10):766-67.10.1002/dc.2091018773434 [Google Scholar] [CrossRef] [PubMed]
[3]. Zuska J J, Crile G Jr, Aryes WW, Fistulas of lactiferous ductsAm J Sur 1951 81(3):312-17.10.1016/0002-9610(51)90233-44 [Google Scholar] [CrossRef]
[4]. Subramaniam MM, En NM, Subareolar abscess in a male breast: Cytological characterisation and distinction from other benign and malignant squamous cell aspiratePathology 2012 44(5):472-74.10.1097/PAT.0b013e3283559db422777072 [Google Scholar] [CrossRef] [PubMed]