The usage of smartphones has escalated tremendously, and they have become the most popular handheld devices among teenagers and young adults. Technology has progressed in recent years and the smartphone has proven to be the most dependable device for communication, entertainment, and various other functions using the internet. This brings along the bane associated with technology and young adults born in the era of technology are termed as digital natives. Most of the smartphone tasks are performed with the neck in a forward position which results in increased anterior curve of the lower cervical spine and increased curvature in the upper thoracic vertebra [1,2].
When a person uses a smartphone, the cervical lordosis is obliterated and it causes injuries to soft tissues around the neck. To balance the neck, the load on the upper trapezius and the erector spinae muscles of the cervical spine increases [3]. With the head in a forward position or a slouched position, the load on the extensor muscles and the connective tissues increases. Subsequently, this poor posture can result in damaging the soft tissues and structure around the spine and thereby altering the proprioceptors in the muscles and ligaments [4]. Poor posture for the long term, can damage not only the cervical spine but also the structures around the lumbar spine, the ligaments, and the bones [5]. Muscle activation and degeneration of ligaments caused by poor posture can also cause neck pain and impair proprioceptors in the muscles and ligaments [6-8]. The structures around the neck and shoulder show a high degree of fatigue, pain, and trigger point formation and are vulnerable to pain when the smartphones are used in an awkward posture [9]. In addition to subjective problems of pain, stress, and fatigue many studies have also focussed on psychological problems [10-12].
However, the current evidence of their utilisation in a flexed neck posture for a prolonged period is considered being the cause for many musculoskeletal problems is somewhat uncertain.
There were very few studies focussing on neck pain and disability due to the extreme use of smartphones in University students but there was no study which correlated smartphone addiction level to neck disability in the Indian context. Therefore, the main aim of the present study was to find out the impact of smartphone addiction on neck pain and disability in university students.
Materials and Methods
This cross-sectional study was conducted between August 2019 to September 2019. Before commencement of the study, an ethical clearance was obtained from the Ethical Committee of Garden City University, Banglore, Karnataka, India. The participants were informed about the nature of the study and an informed consent was taken from them for their willingness to participate in the study. Simple non probability sampling method was used for the selection.
Inclusion criteria: Smartphone users between the age of 18 years to 25 years were included in the study.
Exclusion criteria: Participants who were having radiculopathy, neck and back deformities, history of trauma, fracture or surgery in the neck were excluded from the study.
Sample size calculation: It was calculated by G*power 3.1 software. It was found that as many as 88 subjects were needed for the current study.
The questionnaires were shared with the students through electronic media. And the study recorded their risk of addiction using SAS-SV and neck disability using NDI along with their personal demographic data.
A total of 108 responses were received, out which eight were incomplete and hence, were not included for the analysis. The final analysis was done for 100 responses received, out of which 65 were from female students and 35 were from male students.
Outcome Measures
Smartphone addiction scale-Short version: The SAS-SV is used to identify high-risk smartphone addiction. The SAS-SV includes 10 questions that describe daily-life disturbance, positive anticipation, withdrawal, cyberspace-oriented relationship, overuse, and tolerance. For each item, participants expressed their opinion on a 6-point scale ranging from 1 (strongly disagree) to 6 (strongly agree). It identifies the different ranges for males and females. For males a cut-off value of 31 and for females cut off value of 33 was taken [13].
Neck Disability Index (NDI): It was developed by Vernon and Mior using the Oswestry Low Back Pain Index (OLBPI) as a template for identifying items and a scoring metric. The assessment involves 10 items. Out of the 10 items, four relate to subjective symptoms, four relate to activities of daily living, and two relate to discretionary activities of daily living. Each item is scored on a 0-5 scale in which 0 represents ‘no activity limitation’ and 5 represents ‘complete disability’. The maximum score was 50. A higher score indicated a greater neck disability. The interpretation of NDI scores was 0 to 4- no disability; 5 to 14- mild disability; 15 to 24-moderate disability; 25 to 34- severe disability; and greater than 35- complete disability and was used for this study [14-16].
Statistical Analysis
The data were analysed using IBM SPSS 20.0 statistical software to correlate smartphone addiction scale and NDI. Spearman’s correlation test was performed to analyse the relationship between smart phone addiction and neck disability. Descriptive analysis such as mean, standard deviation was found for the scores of SAS-SV and NDI.
Results
In the current study, the response rate was 92.6%, and 8 (7.4%) students’ responses were incomplete and removed from the analysis. So, only 100 subjects (65 females and 35 males) were included for the final analysis with mean age 20.3±1.62 years. The descriptive data of the participants are shown in [Table/Fig-1].
Descriptive statistics of outcome measures.
| Outcome measure | Minimum | Maximum | Mean±Std. deviation |
|---|
| Age (years) | 18 | 25 | 20.32±1.62 |
| SAS-SV | 15 | 33 | 25.72±6.65 |
| NDI | 2.22 | 48.89 | 26.66±12.58 |
The SAS-SV categorised subjects into no addiction, high risk of addiction, and addiction. The scores of NDI categorised the subjects into no disability, mild disability, moderate disability, and severe disability. The results of the data show that 40%, 23.1% and 36.9% of females were in the no addiction, high risk of addiction and addicted category, respectively, and among the males, 31.4%, 62.9%, and 5.7% were in the category of no addiction, high risk of addiction and addicted category, respectively. In this study, the mean score of SAS-SV for both male and female subjects was 25.72. It was found that females were higher in the addiction category. With respect to NDI 3.07% of females were in the no disability category, 53.8% were in the mild disability and 41.5% of subjects were in the moderate disability and 1.5% were in the severe disability category. Among the male subjects, there were 2.9% who were in the no disability category, 37.1% under mild disability, and 60% were in the moderate disability. However, there were no males in the severe disability. Though females were more in the addiction category, the study did not find them to develop proportionate severe neck disability [Table/Fig-2]. In this study, the mean score for NDI in male and female subjects was 26.66.
Frequency distribution of subject characteristics.
| Outcome measure | Frequency | Male (%) | Female (%) |
|---|
| SAS-SV | 100 | 35 | 65 |
| No addiction | 37 | 11 (31.4) | 26 (40) |
| High risk of addiction | 37 | 22 (62.9) | 15 (23.1) |
| Addiction | 26 | 2 (5.7) | 24 (36.9) |
| NDI | 100 | 35 | 65 |
| No disability | 3 | 1 (2.9) | 2 (3.07) |
| Mild disability | 48 | 13 (37.14) | 35 (53.8) |
| Moderate disability | 48 | 21 (60) | 27 (41.5) |
| Severe disability | 1 | 0 | 1 (1.5) |
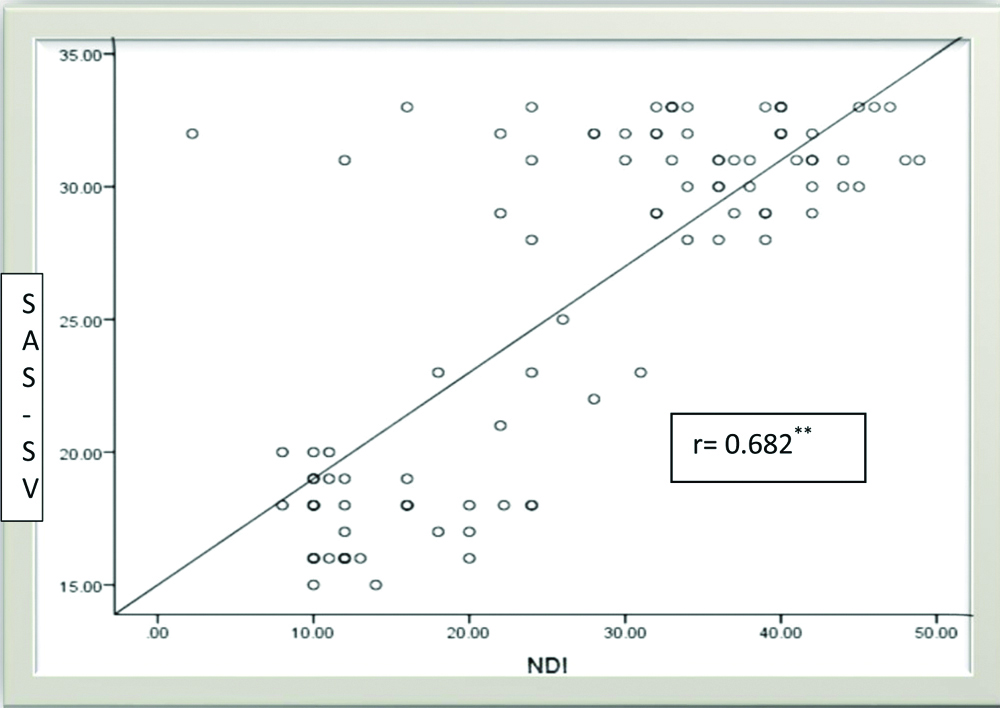
The Spearman correlation analysis results of the study clearly showed that there was a moderate positive correlation (r=0.682) between smartphone addiction and neck pain and disability. The level of significance was p<0.01 [Table/Fig-3].
Spearman correlation test was used to find the correlation between NDI and SAS-SV, the level of significance was p<0.01.
NDI: Neck disability index and SAS-SV: Smartphone assessment scale-short version
Discussion
The current study was done to evaluate the association between addictive smartphone users and neck disability with the help of SAS-SV and NDI. The SAS-SV categorised subjects into no addiction, high risk of addiction, and addiction. The scores of NDI categorised the subjects into no disability, mild disability, moderate disability, and severe disability. Out of 100 samples that were analysed, 37% were under the no addiction category, the remaining 63% either were under the high risk or addicted to smartphone category which is quite alarming in university students. This study revealed that no student in this sample was without a smartphone. The posture in which they used the smartphone also adds on to their disability, where they adopt a flexed spinal posture while texting on mobile phones. This is found to be the most common posture that contributes to neck pain [17].
Besides, this study, it was also found out that only 3% of the samples did not have any neck disability whereas 48% had a mild and equal number of the percentage had a moderate disability of the neck. So, it can be inferred that students of higher education have higher chances of developing pain and functional difficulty in activities of daily living and are quite common because of the regular use of the smartphone. This study reiterates the statement made by other authors who stated that the most common posture is a flexed posture while using the smartphone and this leads to neck pain. It also acknowledges the studies done previously which state that pain due to musculoskeletal disorders is a common problem seen in college-going students [17-20].
Further, this study demonstrated that subjects who were at high risk of smartphone addiction have a higher score in the NDI and the study found a significant positive correlation between smartphone addiction and neck disability. A high score on the disability in the neck may be contributed to altered and sustained neck posture leading to repetitive strain injury to neck musculature and surrounding soft tissue structures. This is supported by studies that stated that excessive smartphone use resulted in neck disability as the neck would have to be flexed more often by compromising the posture. This would lead to the development of trigger point in the upper trapezius and alter the curvature of the spine and increase the stress on the cervical spine [21-23]. In this study, moderate correlation was found between the SAS-SV, and NDI. A systematic review has also proved that the duration of smartphone usage is directly proportionate to the development of musculoskeletal complaints in the shoulders, neck, and lower back pain [24].
Limitation(s)
In this study, the gender failed to be stratified, hence the total number of female students was more than the males. Gender can serve as a confounding factor as previous research studies have shown that females are more likely to develop musculoskeletal symptoms of neck and upper extremities compared to males [25]. The study included only university students and was limited to the given age group, limiting the ability of this study to assess the pain characteristics among different age groups, the use of other devices (e.g., laptops), or even the posture of studying from books were not considered. Further studies assessing the above mentioned characteristics needs to be conducted.
Conclusion(s)
This study concludes that the excessive use of smartphones in university students could result in neck pain and disability as it was found that there is a moderate correlation between the smartphone addiction and neck disability. Students need proper guidance on optimal usage of smartphone as well as correct body posture during usage of a smartphone which may considerably reduce neck disability in university students. Hence, there is an urgent need for ergonomic education for young adults regarding usage of smartphones and awareness about the possible musculoskeletal problems that could arise due to excessive use of smartphones in an improper position. The importance of having healthy sitting positions and using mobile phones for restricted durations, to control the increasing prevalence of neck pain should be emphasised.