Irreducible Hernia in Female Children with Ovary, Uterus or Uterine Adnexa: A Case Series
Joseph Francis1, Suhitha Gajanthody2, Ashraf Ahamed3, Divya Syam4
1 Senior Resident, Department of General Surgery, Yenepoya Medical College Hospital, Mangalore, Karnataka, India.
2 Assistant Professor, Department of Paediatric Surgery, Yenepoya Medical College Hospital, Mangalore, Karnataka, India.
3 Associate Professor, Department of Paediatric Surgery, Yenepoya Medical College Hospital, Mangalore, Karnataka, India.
4 Junior Resident, Department of General Surgery, Yenepoya Medical College Hospital, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suhitha Gajanthody, Department of Paediatric Surgery, Yenepoya Medical College Hospital, Mangalore, Karnataka, India.
E-mail: suhith1983@gmail.com
Inguinal hernias are the most frequent hernias of childhood. They are relatively uncommon in females as compared to males. Congenital inguinal hernias are due to the failure of closure of processus vaginalis. In females, this usually obliterates around the eighth month of foetal life. When these remain patent, a rare but possible herniation of contents can occur through this, like the genito-urinary system, including the ovaries and sometimes the fallopian tubes. However, the occurrence of uterus as one of the contents is a rare entity. This is a case series of six such cases with various genital tract entities as contents in paediatric female inguinal hernia. In conclusion, the rare entity of uterus, uterine adnexae and ovaries being a content of inguinal hernia has to be kept in mind when treating female children.
Genito-urinary system, Ovarian torsion, Sliding hernia, Strangulation
Introduction
Inguinal hernias occur in 5% of full-term and 30% of preterm infants, and it is 4 to 10 times more frequent in boys [1]. The cause is postulated to be the incomplete closure of the processus vaginalis of the peritoneum. In girls, the genital tract may be found as a sliding component, fallopian tube and ovary in 15-20% inguinal hernias. However, the occurrence of uterus as of the contents is a rare entity [2]. A review of literature suggests that little is known regarding the specific causation or aetiopathogenesis of the condition with variations in suggested surgical treatment.
This is a case series of six cases with various genital tract entities as contents in paediatric female inguinal hernia. All the patients visited the study institute between 2016 and 2020.
Case Series
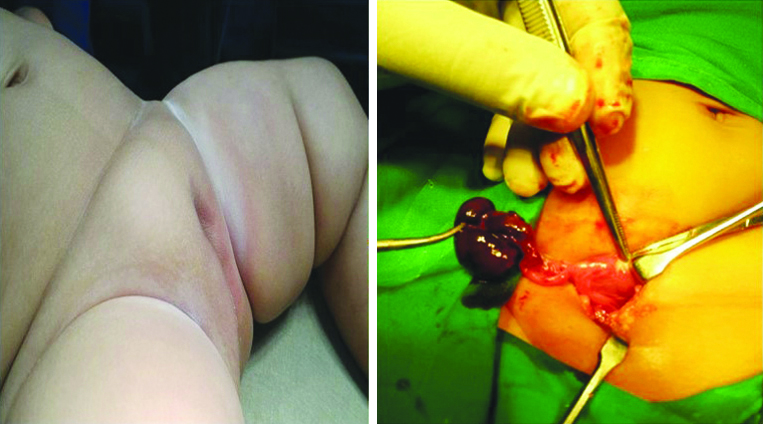
Case 1: A 4-month-old child was presented with complaints of right sided inguinal swelling and excessive cry since two days. On examination, the patient had irreducible inguinal hernia with severe tenderness. Ultrasonography (USG) revealed right inguinal hernia (ovary and fallopian tube as content) with no vascularity on doppler. Intraoperatively, the content was found to be right fallopian tube and torsioned right ovary which was not viable. So, the patient was subjected to oophorectomy followed by high ligation.
Case 2: A 3-month-old child presented with complaints of right side inguinal swelling and pain over the swelling for three days. On examination, the patient had irreducible inguinal hernia with tenderness. Intra-operatively the content of hernia was found to be uterus, bilateral ovaries and fallopian tubes, which were reduced. Lax posterior wall was plicated and strenghthened.
Case 3: A 6-year-old child came with complaints of bilateral inguinal swellings noticed since birth. On examination, the patient had bilateral irreducible swellings with no tenderness. The USG revealed bilateral inguinal hernia with ovaries as the content. Surgical findings revealed ovary as the content on the right side and ovary and fallopian tube on the left. Bilateral high ligation was done for this patient.
Cases 4, 5 and 6: These three children had similar chief complaints of right, left and left inguinal swellings respectively, since birth with no other symptoms. They were 5, 2 and 3 months of age, respectively. Examination revealed irreducible inguinal swellings with no tenderness. Intraoperatively, the contents were the ipsilateral ovary and fallopian tube, which were reduced and high ligation done.
Follow-up of all the patients were done at two weeks and three months after surgery which were all uneventful. The clinical details, and the procedures done have been mentioned in [Table/Fig-1] and the related images are shown in [Table/Fig-2,3].
| Variables/Case No. | 1 | 2 | 3 | 4 | 5 | 6 |
|---|
| Age | 4 months | 3 months | 6 years | 5 months | 2 months | 3 months |
| History of prematurity | No | No | No | No | No | No |
| Side | Right | Right | Bilateral | Right | Left | Left |
| Symptoms | Inguinal swellingExcess cry | Inguinal swelling | Inguinal swelling | Inguinal swelling | Inguinal swelling | Inguinal swelling |
| Clinical examination | Irreducible swelling, no signs of strangulation | Irreducible swelling, no signs of strangulation | Bilateral irreducible swelling, no signs of strangulation | Irreducible swelling, no signs of strangulation | Irreducible swelling, no signs of strangulation | Irreducible swelling, no signs of strangulation |
| Preoperative sonological findings | Right inguinal hernia with ovary and fallopian tube as content with no vascularity on doppler | Inconclusive | Bilateral inguinal hernia with ovary seen on both sides | Inconclusive | Inconclusive | Left ovary visualised as content of inguinal hernia |
| Contents | Right ovary and fallopian tube with torsion | Uterus, bilateral ovaries and fallopian tubes | Right side-ovaryLeft side-ovary with fallopian tube | Right ovary and fallopian tube | Left ovary and fallopian tube | Left ovary and part of uterus |
| Operative procedure | Right oopherectomy and high ligation | Plication with posterior wall strengthening | Bilateral high ligation | High ligation | High ligation | High ligation |
Right sided inguinal hernia with ovarian torsion.
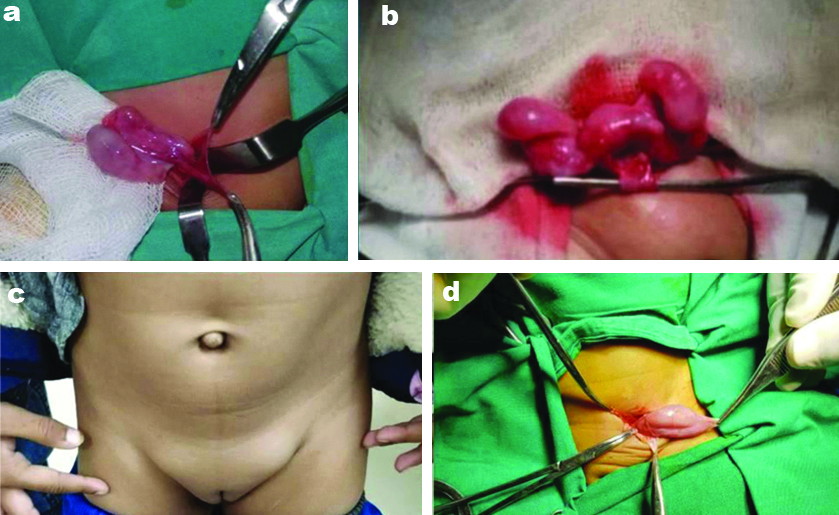
a) Right ovary with fallopian tube, b) Hernia Uteri inguinale with bilateral ovaries and fallopian tube, c) Clinical picture of bilateral inguinal hernia, d) Left Hernia Uteri inguinale.
Discussion
A patent processus vaginalis results in an indirect inguinal hernia. Sometimes, sliding hernia may occur with variable contents such as appendix, small bowel, Meckel’s diverticulum, genital tract elements like uterus, ovary or fallopian tubes and the bladder. In the girl child, ovary is a common entity and finding the uterus within the hernia is defined as Hernia Uteri Inguinale (HUI) [3]. Prematurity is often associated with increased incidence of genital tract components as contents in the hernia [2]. In this series, none of the subjects were born prematurely.
Akillioğlu I et al., described seven cases of HUI among 3100 female children over 11 years, with a mean age of 7.4 months at diagnosis. Four out of seven cases had inguinal mass on the left side; all were diagnosed intraoperatively to have genital organs as contents [2]. In the present series, five out of six children were diagnosed at less than one year of age, with one child presenting as late as 6 years with a bilateral swelling. Three cases presented with swelling on the right, two on the left and one was bilateral.
Merriman TE and Auldist AW studied 11 cases of ovarian torsion in inguinal hernia and found that the primary aetiology was torsion of the ovary upon its pedicle, temporarily held in a “bell-clapper” like position within a hernial sac. The incidence of ovarian torsion in the study was 2-33% [4]. In the present series, first case was preoperatively suspected to have ovarian torsion due to negative doppler signal on sonography. Intraoperatively, the ovary was not viable and hence removed along with fixation of the tubes and high ligation to prevent further herniation.
In a study by Zitsman JL et al., vaginal bleeding in an infant was an indicator for HUI [5]. In this series, all the children were of female phenotype and no genital abnormalities were detected. Hence, karyotyping was not performed. Abdominal ultrasound confirmed the presence of female genital organs.
Bijnens E et al., concluded that sonographers may occasionally encounter the uterus and adnexal structures within an inguinal hernia [6]. Ming YC et al., also suggested that sonography to be performed routinely in female inguinal hernia cases [7]. Clinical examination was the corner stone of diagnosis in the present series; with all cases presenting as irreducible inguinal masses. Signs of strangulation like redness of skin and tenderness could not be positively elicited in these infants, and hence were not relied upon. Ultrasonography was done in all cases, keeping in mind the possibility of genital organs as contents but lacked conclusive evidence. However, it aided in early operative intervention in the case of ovarian torsion.
Various case reports suggested that a classic herniorrhaphy with high ligation of the sac was the most commonly performed procedure [8-10]. In this case series, same principles was followed for hernia repair and had experienced good results.
Conclusion(s)
The rare entity of uterus, uterine adnexae and ovaries being a content of inguinal hernia has to be kept in mind when treating female children. An ultrasound may guide towards early detection of surgical emergency like ovarian torsion, as early signs of strangulation are difficult to elicit in children.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jan 21, 2021
Manual Googling: May 05, 2021
iThenticate Software: May 31, 2021 (10%)
[1]. Chen YH, Wei CH, Wang KWK, Children with inguinal hernia repairs: Age and gender characteristicsGlob Pediatr Health 2018 5:01-06.10.1177/2333794X1881690930560149 [Google Scholar] [CrossRef] [PubMed]
[2]. Akillioğlu I, Kaymakci A, Akkoyun I, Güven S, Yücesan Ş, Hiçsönmez A, Inguinal hernias containing the uterus: A case series of 7 female childrenJ Pediatr Surg 2013 48(10):2157-59.10.1016/j.jpedsurg.2013.04.02724094973 [Google Scholar] [CrossRef] [PubMed]
[3]. George EK, Oudesluys-Murphy AM, Madern GC, Cleyndert P, Blomjous JGAM, Inguinal hernias containing the uterus, fallopian tube, and ovary in premature female infantsJ Pediatr 2000 136(5):696-98.10.1067/mpd.2000.10514010802507 [Google Scholar] [CrossRef] [PubMed]
[4]. Merriman TE, Auldist AW, Ovarian torsion in inguinal herniasPediatr Surg Int 2000 16(5-6):383-85.10.1007/s00383000042810955568 [Google Scholar] [CrossRef] [PubMed]
[5]. Zitsman JL, Cirincione E, Margossian H, Vaginal bleeding in an infant secondary to sliding inguinal herniaObstet Gynecol 1997 89(5 II SUPPL):840-42.10.1016/S0029-7844(97)00055-0 [Google Scholar] [CrossRef]
[6]. Bijnens E, Broeckx J, Hoffbauer R, Borreman JP, Sonographic diagnosis of an incarcerated inguinal hernia containing uterus and left adnex AJ Ultrasound Med 1992 11(5):249-50.10.7863/jum.1992.11.5.2491588698 [Google Scholar] [CrossRef] [PubMed]
[7]. Ming YC, Luo CC, Chao HC, Chu SM, Inguinal hernia containing uterus and uterine adnexa in female infants: Report of two casesPediatr Neonatol 2011 52(2):103-05.10.1016/j.pedneo.2011.02.00621524631 [Google Scholar] [CrossRef] [PubMed]
[8]. Cascini V, Lisi G, Di Renzo D, Pappalepore N, Lelli Chiesa P, Irreducible indirect inguinal hernia containing uterus and bilateral adnexa in a premature female infant: Report of an exceptional case and review of the literatureJ Pediatr Surg 2013 48(1):e17-19.10.1016/j.jpedsurg.2012.09.06523331833 [Google Scholar] [CrossRef] [PubMed]
[9]. Fowler CL, Sliding indirect hernia containing both ovariesJ Pediatr Surg 2005 40(9):e13-14.10.1016/j.jpedsurg.2005.05.06616150325 [Google Scholar] [CrossRef] [PubMed]
[10]. Harjai MM, Uncommon content in congenial inguinal herniaJ Indian Assoc Pediatr Surg 2014 19(4):244-45.10.4103/0971-9261.14202325336812 [Google Scholar] [CrossRef] [PubMed]