Breast cancer is the most common malignancy in females worldwide. Mammography is a screening tool to detect breast cancer. It is cost-effective and easily available [1]. Screening of breast cancer increases the survival among the patients [2]. Dynamic MRI of the breast is viewed as an examination technique which is supplementary to mammography and sonogram and can provide important additional diagnostic information [3-5].
Accepted indications for MRI of the breast include examination of patients who have undergone lumpectomy or mastectomy and patients having prosthetic breast implants. This method also appears to be useful for differentiation between post operative scarring and carcinoma as well as to exclude a multicentric breast cancer prior to breast conserving surgery [6,7]. MRI is recommended as a screening test for women who are at high risk of breast cancer according to genetic susceptibility [8-10].
The sensitivity of MRI however is limited in cases of Ductal Carcinoma In-Situ (DCIS) [3]. After being diagnosed with breast cancer, a breast MRI may be performed to determine the size of the tumour and level of infiltration, the presence of multicentric lesions in the same breast, whether there is an undetected tumour in the opposite breast and lymph node metastasis to the opposite axilla. MRI has very high sensitivity in detecting carcinoma breast than mammography and sonography of breast [3,7]. The sensitivity of mammography is limited in breast containing dense tissue, due to the presence of fibro-glandular tissue over the lesion which reduces the detection of abnormalities [11].
As mammography cannot detect the early cancer of the breast in young patients with dense breast tissue, in those settings MRI is required for early detection of the cancer. This study had been conducted to compare the effectiveness of mammography and MRI in detecting breast cancer in Indian setting by taking a large group of population.
The objective of this study was to compare the sensitivity and specificity of MRI and mammography in the diagnosis of breast cancer.
Materials and Methods
This was a longitudinal observational study done in the General Surgery Department of SCB Medical College, Cuttack from April 2018 to January 2020. Approval from the Institutional Ethics Committee was obtained (IEC/IRB No: 1008/14.10.2019). Informed and written consent was obtained from all participants.
Inclusion criteria: Patients with breast lump (suspected clinically of malignancy) and belonging to 25-75 years age group were included in the study.
Exclusion criteria: Patients with recurrence after previous surgery, patients who did not give consent to take part in the study were excluded from the study.
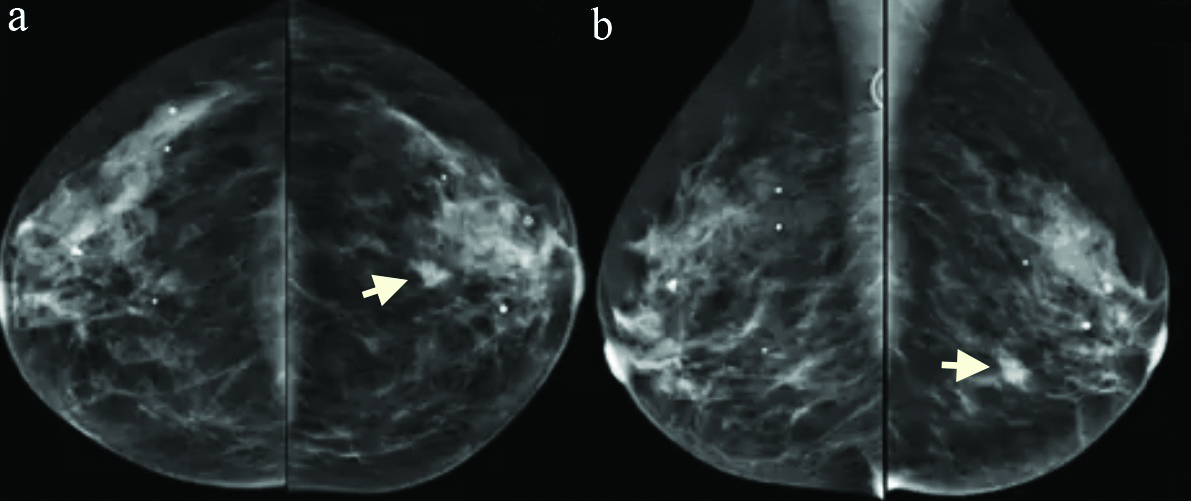
Demographic parameters of all patients like age, weight, Body Mass Index (BMI), family history were noted. The clinical Tumour, Nodes, Metastases (TNM) stage was determined in all patients [12]. All the patients were subjected to standard mammogram and MRI of the breast in the Radiology Department of the institution by an expert radiologist with at least five year experience [Table/Fig-1,2,3 and 4].
Mammogram showing carcinoma in the left breast (arrow); a) cranio-caudal view; b) mediolateral-oblique view.
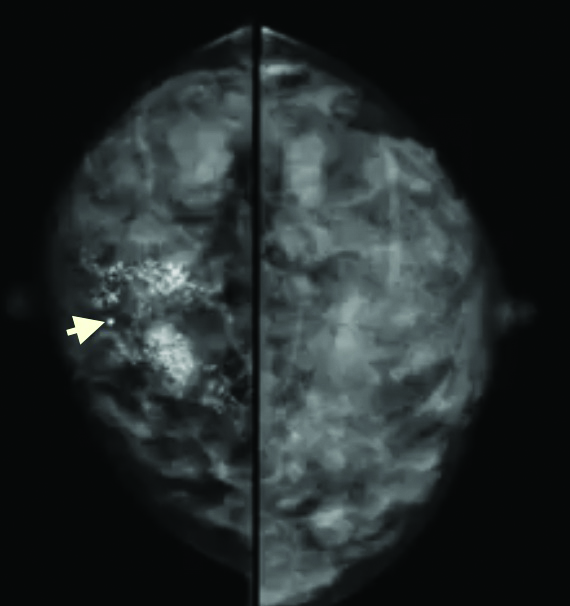
Cranio-caudal mammogram of right breast showing microcalcification (arrow) due to cancer.
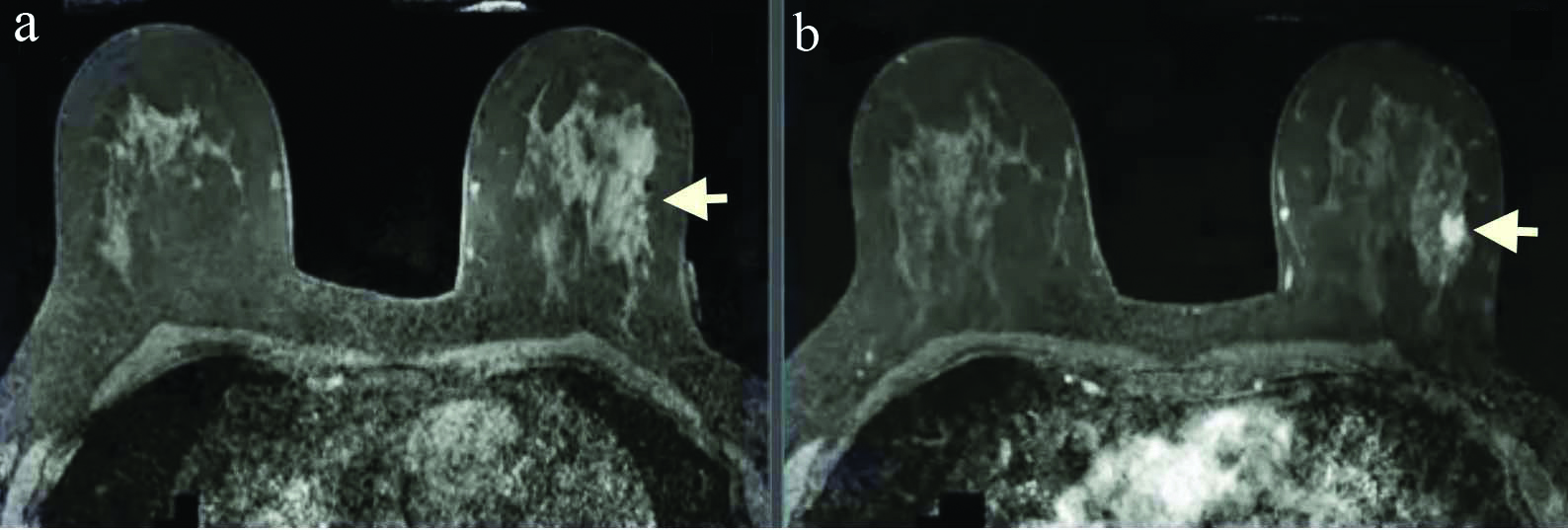
MRI of breasts showing cancer in the left breast (arrow) a. precontrast, b. post gadolinium contrast.
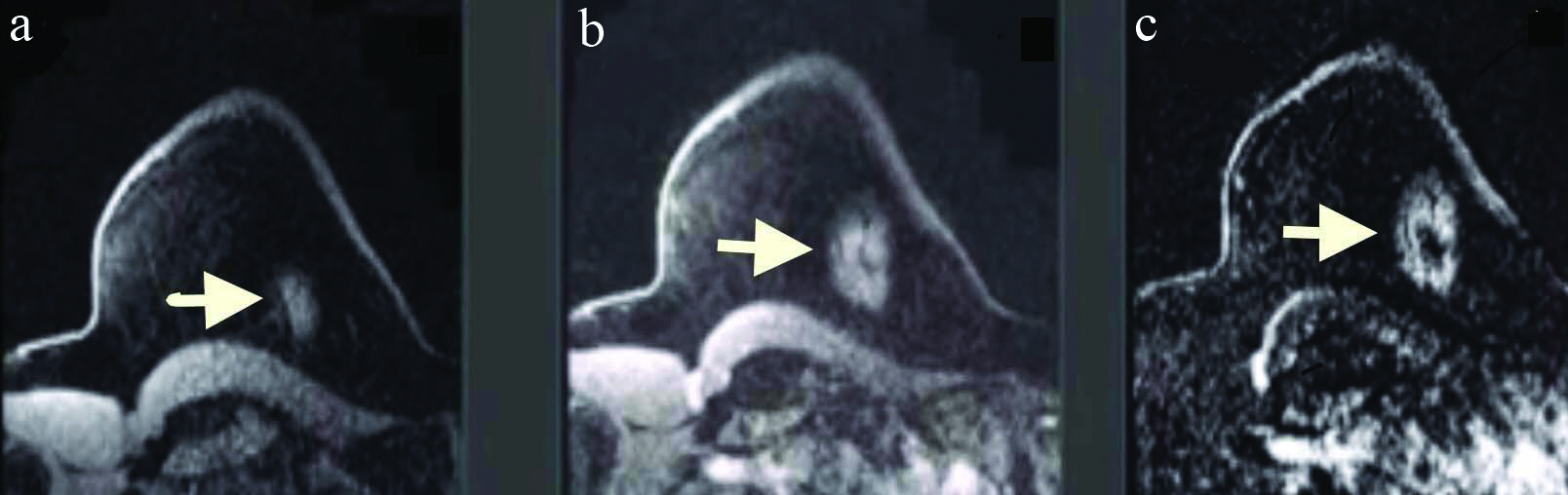
MRI of breasts showing cancer in the left breast (arrow) a. precontrast, b. post gadolinium contrast, c. subtraction image
The Breast Imaging Reporting and Database (BI-RADS) score was determined for every patient [13]. After imaging, the diagnosis was confirmed by trucut biopsy by a histopathologist with at least five year experience, in the Pathology Department of the institute. The results of MRI and mammography were compared with that of the results of histopathology and the sensitivity and specificity of MRI and mammography were calculated.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Version 21.0 (IBM, IL, Chicago). Parametric numerical data were reported as mean±standard deviation for continuous variables; non parametric numerical data were represented as median (range). Student’s t-test was used to compare numerical variables and Chi-square test was used to compare qualitative data. The p<0.05 was considered statistically significant.
Results
A total of 228 patients who fulfilled the eligibility criteria were included in the study. All patients were females. The mean age was 53.8 years (range of 27-73 years, SD=11.5 years). The mean weight and mean BMI were 61.3 kg (range of 48-97 kg, SD=12.25 kg) and 23.9 kg/m2 (range of 17.7-28.4 kg/m2, SD=2.67 kg/m2). The age distribution of the patients is shown in [Table/Fig-5]. Most of the patients were between 45-65 years of age.
Age distribution of patients.
| Age (in years) | No. of patients (N=228) |
|---|
| 25-35 | 8 (3.5%) |
| 35-45 | 21 (9.2%) |
| 45-55 | 98 (43%) |
| 55-65 | 87 (38.2%) |
| 65-75 | 14 (6.1%) |
| Mean | 53.8±11.5 years |
Mammography detected malignancy in 193 (84.64%) out of the 228 patients; whereas MRI detected malignancy in 209 (91.6%) patients. Total 216 (94.7%) patients actually had malignancy and 12 (5.3%) patients had no malignancy which was confirmed by histopathological examination [Table/Fig-6].
Sensitivity and specificity of mammography and MRI in detecting breast cancer.
| Parameters | Mammography | MRI |
|---|
| Malignancy detected {number of patients (%)} | 193 (84.64) | 209 (91.6) |
| Malignancy not detected {number of patients (%)} | 35 (15.36) | 19 (8.4) |
| Sensitivity (%) | 95 | 95.83 |
| Specificity (%) | 89.28 | 83.33 |
Among the 216 histopathologically confirmed patients, 174 (80.5%) had invasive ductal carcinoma, 23 (10.6%) had ductal carcinoma in situ, 13 (6%) had invasive lobular carcinoma and 6 (2.9%) had lobular carcinoma in situ. In 12 patients, who were suspected of malignancy clinically, the histopathology report came out to be benign (seven were fibroadenoma, three were fibrocystic disease and one each phyllodes tumour and fat necrosis).
According to cTNM staging, distribution of the patients is depicted in [Table/Fig-7] (with 70.6% patients belonging to stage 2). The BI-RADS score of the patients is shown in [Table/Fig-8] (with 49.1% patients belonging to BI-RADS-4).
| Stage | Number of patients n (%) |
|---|
| 2A | 87 (38.2) |
| 2B | 74 (32.4) |
| 3A | 53 (23.2) |
| 3B | 14 (6.2) |
BI-RADS score of patients.
| BI-RADS score | Number of patients n (%) |
|---|
| 2 | 23 (10.1) |
| 3 | 9 (4) |
| 4 | 112 (49.1) |
| 5 | 84 (36.8) |
The sensitivity and specificity of mammography and MRI in detecting breast cancer are depicted in [Table/Fig-9]. The difference in sensitivity and specificity between mammography and MRI in detecting breast cancer was found to be statistically non significant.
Sensitivity and specificity of mammography and MRI (p-value <0.05 is considered as statistically significant).
| Variables | Mammography | MRI | p-value |
|---|
| Sensitivity | 95% | 95.83% | 0.952 |
| Specificity | 89.28% | 83.33% | 0.651 |
Discussion
In this study, it was found that the sensitivity and specificity of mammography was 95% and 89.28%, respectively, in detecting breast cancer whereas sensitivity and specificity of MRI in detecting breast cancer is 95.83% and 83.33%, respectively. Invasive ductal carcinoma (80.5%) was the most common type of histological variety in the study. Invasive ductal carcinoma is the most common variety of breast cancer accounting for 70-80% of all invasive breast cancers [14].
In their study of 60 patients, Patil SV et al., found out that 45 patients had palpable and 15 patients had non palpable breast mass. In case of palpable lesions mammography and MRI had sensitivity of 95% and 90%, respectively whereas the specificity of 30% and 50%, respectively. For non palpable lumps, the sensitivity of mammography was 70% as compared to sensitivity of MRI 90%, while specificity of mammography was 25% and MRI showed 50% specificity [15].
In their study of 529 women starting from 30 years and above for a duration of five years Kuhl CK et al., found out, the sensitivity of MRI was 91% and of mammogram was 33% and the specificity of both MRI and mammography were 97% [7]. Kacl GM et al., studied 50 patients and found out the sensitivity and specificity of mammography and MRI in detecting breast cancer was 82% and 64%, and 92% and 76%, respectively [16].
Wernli KJ et al., studied 13,266 women above 18 years of age from 2005 to 2012. They found out the sensitivity of mammography and MRI as 70.3% and 61.4%, respectively [17]. In Toronto, Warner E et al., screened 236 women of age group 25-65 years by using multi-modal approach. Within three years of their study, they identified 22 new cases out of which 16 were invasive cancer. They found that sensitivity of MRI and mammogram was 77% and 36%, respectively and specificity was 95% and 99.8% for MRI and mammography, respectively [18].
Podo F et al., conducted a study in Italy in 2002 and found out the sensitivity of mammography and MRI were 13% and 100%, respectively and the specificity was 100% and 99% for mammography and MRI, respectively from their study [19].
Kriege M et al., studied 1,909 women between 25-70 years of age at six centers across Netherlands. The sensitivity of MRI and mammogram was 71% and 40%, respectively and specificity was 90% and 95% for MRI and mammography, respectively [20]. The results of studies done by Morris EA et al., and Comstock CE et al., (examined 1,444 women between 40-75 years) are shown in [Table/Fig-10] [7,15-22].
Results of various studies regarding the effectiveness of MRI and mammography in detecting breast cancer [7,15-22].
| Study (year) | Sensitivity of mammography | Specificity of mammography | Sensitivity of MRI | Specificity of MRI |
|---|
| Patil SV et al., (2020) (palpable breast mass) [15] | 95% | 30% | 90% | 50% |
| Patil SV et al., (2020) (non palpable breast mass) [15] | 70% | 25% | 90% | 50% |
| Kuhl CK et al., (2005) [7] | 33% | 97% | 91% | 97% |
| Kacl GM et al., (1998) [16] | 82% | 64% | 92% | 76% |
| Wernli KJ et al., (2019) [17] | 70.3% | - | 61.4% | - |
| Warner E et al., (2004) [18] | 36% | 99.8% | 77% | 95% |
| Podo F et al., (2002) [19] | 13% | 100% | 100% | 99% |
| Kriege M et al., (2004) [20] | 40% | 95% | 71% | 90% |
| Morris EA et al., (2003) [21] | - | 69% | - | 77% |
| Comstock CE et al., (2020) [22] | - | 95.7% | - | 86.7% |
The results of this study are similar to the above mentioned studies. It was found out that the sensitivity of MRI is slightly more than mammography in detecting breast cancer, though statistically non significant. The sensitivity of MRI is more in detecting breast cancer in young females who have dense breast [9,23,24].
Magnetic resonance imaging tends to overdiagnose the malignancy for which the specificity of MRI is low to moderate in the range of 37-97% [25,26]. MRI is quite expensive and is difficult to perform in claustrophobic patients. In a resource poor country like India, MRI is not available widely and it should be used in selected cases. Still MRI is the modality of choice for detecting cancer in young patients with dense breast tissue and patients having familial cancer syndromes. In these patients the sensitivity of mammography is poor in detecting the cancer [3,8,9].
Limitation(s)
The limitation of the study is that special emphasis for screening of familial breast cancer was not given.
Conclusion(s)
From the study, it was found out that the sensitivity and specificity of MRI and mammography is similar in detecting breast cancer. However, both the investigations have their own pros and cons. A multicentric study involving more number of patients should be done to further evaluate these investigations in detecting breast cancer.