A Cadaveric Study of Radial Nerve Course and its Clinical Implications on Radial Nerve Block at Elbow
Srimathi Ramasamy1, Muthu Kumar Thyagarajan2, Chandrasekar Raju3
1 Associate Professor, Department of Anatomy, SRIHER, Chennai, Tamil Nadu, India.
2 Associate Professor, Department of Anatomy, SRIHER, Chennai, Tamil Nadu, India.
3 Associate Professor, Department of Forensic Medicine/Anesthesia, KAPVGMC, Trichy, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Srimathi Ramasamy, Associate Professor, Department of Anatomy, SRIHER, Chennai, Tamil Nadu, India.
E-mail: drtsanatsrmc@gmail.com
Introduction
Upper limb nerve blocks are done commonly by brachial plexus (C5-T1) blocks via supraclavicular, infraclavicular approaches. Sometimes a single peripheral nerve needs additional block with local anaesthetic to achieve adequate block. Peripheral nerve blocks are useful for minor surgical procedures in a single nerve distribution.
Aim
To study the course and clinical significance of the radial nerve in 50 cadaveric upper limbs.
Materials and Methods
A cross-sectional study was conducted on 50 intact dissected upper limbs. The upper limbs were obtained from the Department of Anatomy, Sri Ramachandra Medical College from August 2020 to December 2020. Radial nerve was exposed by routine dissection in all the upper limbs and its entire course was studied and observed for any variation. The distance from the biceps tendon to the radial nerve at the elbow, distance of the radial nerve in the Lateral Intermuscular Septum (LIS) from the epicondyles at the elbow were measured. The results obtained were statistically analysed using Statistical Package for the Social Sciences (SPSS) version 16.0.
Results
In present study, the mean distance of the radial nerve in the LIS to the medial epicondyle was 12.4±0.31 cm and to the lateral epicondyle was 12.1±0.28 cm. The mean distance from the biceps tendon to the radial nerve at the elbow was 1.75±0.22 cm.
Conclusion
From the present study, it can be inferred that effective peripheral radial nerve block can be achieved by blocking the nerve 1.75 cm lateral to the biceps tendon at the elbow 3 cm above the elbow crease. This can be made comfortable to the patient and more precise by ultrasound localisation of the radial nerve.
Anaesthesia, Elbow block, Peripheral nerve block
Introduction
Upper limb nerve blocks are done commonly by brachial plexus (C5-T1) blocks via supraclavicular, infraclavicular approaches. The two main disadvantages of these procedures are iatrogenic injury to other nearby structures like blood vessels and inadequate anaesthesia in the areas supplied by its terminal branches. To have an effective nerve block, terminal nerve block is a suitable add on procedure. Such blocks are useful for minor surgical procedures in a peripheral nerve distribution [1].
Radial nerve arises from the posterior cord of brachial plexus [2], With profunda brachii it lies in the lower triangular space in the arm, then deep to the lateral head of triceps brachiate pierces the LIS and enters the anterior compartment of the arm. It lies between the brachialis and the brachioradialis and extensor carpi radialis longus muscles [3]. It divides into superficial and deep branches in the forearm. It supplies triceps, the extensors of the forearm and it provides the sensory innervation to the skin of the lower lateral arm the posterior aspect of the forearm and the skin over the dorsum of the hand (lateral three and half fingers) [3].
The radial groove, and the LIS are important surgical landmarks for the radial nerve in the arm since the radial nerve is commonly injured in these sites and also as it passes between the heads of the triceps brachii muscle [4-7]. Radial nerve lies 1 to 2 cm lateral to the biceps tendon at the elbow. This is a landmark to identify the radial nerve where it can be blocked to achieve sensory anaesthesia in the area supplied by it [1].
Ultrasound-guided elbow blocks reduce the duration of anaesthesia, the dose of drug required, and is comfortable and safe for the patient. Iatrogenic injury to the adjacent vessels can be avoided [8]. Hence, present study was conducted with an aim to study the course of the radial nerve in the 50 upper limbs of both sides and its clinical significance.
Materials and Methods
Fifty intact upper limbs were dissected for evaluation in this cadaveric cross-sectional study which were obtained from the Department of Anatomy, Sri Ramachandra Medical College during August 2020 to December 2020. Ethical clearance was obtained from the Institutional Ethics Committee. (REF:IEC-N1/20/JAN/73/01 dated 24.8.2020).
Inclusion criteria: The upper limbs of normal surface anatomy and bony landmarks of both genders and sides were included in the study.
Exclusion criteria: The upper limbs with trauma, deformity and contractures were excluded from the study.
Radial nerve was exposed by routine dissection in all the upper limbs and its entire course was studied and observed for any variation [9]. For dissection, the limbs were placed in an extended position. An incision was made from the tip of the acromion process to the superior aspect of the olecranon process [10]. The skin and subcutaneous tissues were removed from the back of arm to view the triceps brachi muscle. The long and lateral heads of the triceps were separated. Radial nerve was exposed by incising through the lateral head of triceps, then in the spiral groove between lateral and medial heads of the triceps. The radial nerve was traced upto the elbow as it passes into the anterior compartment of the arm by piercing the LIS.
The distance from the biceps tendon to the radial nerve at the elbow, distance of the radial nerve from its entry point in LIS to the medial epicondyle, distance of the radial nerve from its entry point in LIS to the lateral epicondyle at the elbow were measured. Radial nerve localisation was done in elbow, at LIS using USG techniques [11].
Statistical Analysis
The data was recorded and analysed using SPSS version 16.0. The incidence of each variation was expressed in frequency (N) and percentage. The distance variable was expressed as Mean±Standard deviation.
Results
In present study, the mean distance from the biceps tendon to the radial nerve at the elbow was 1.75±0.22 cm [Table/Fig-1], the mean distance of the radial nerve in the LIS to the medial epicondyle was 12.4±0.31 cm [Table/Fig-2] and to the lateral epicondyle was 12.18±0.28 cm [Table/Fig-3]. The results were compared with those of previous researchers [Table/Fig-4] [1,12,13].
Distance of the radial nerve from the biceps tendon at the elbow.
| Distance from biceps tendon (in cm) | Side | No. of upper limbs | Percentage of upper limbs |
|---|
| 2 | Right | 20 | 40 |
| 1.6 | Left | 7 | 14 |
| 1.5 | Right | 9 | 18 |
| 1.8 | Left | 14 | 28 |
Mean±SD=1.75±0.22
Distance of the radial nerve (LIS) from the medial epicondyle at the elbow.
| Distance from medial epicondyle (in cm) | Side | No. of upper limbs | Percentage of upper limbs |
|---|
| 12.8 | Left | 6 | 12 |
| 12.6 | Right | 20 | 40 |
| 12.6 | Left | 8 | 16 |
| 12 | Left | 4 | 10 |
| 12 | Right | 1 | 2 |
| 12.2 | Left | 3 | 6 |
| 12.4 | Right | 8 | 16 |
Mean±SD=12.4±0.31
Distance of the radial nerve (LIS) from the lateral epicondyle at the elbow.
| Distance from lateral epicondyle (in cm) | Side | No. of upper limbs | Percentage of upper limbs |
|---|
| 12 | Right | 20 | 40 |
| 12 | Left | 10 | 20 |
| 12.2 | Left | 5 | 10 |
| 12.5 | Right | 8 | 16 |
| 11.8 | Left | 2 | 4 |
| 11.8 | Right | 1 | 2 |
| 12.4 | Left | 4 | 8 |
Mean±SD=12.18±0.28
Comparison of the index study with Literature.
| Study | Year | No. of upper limb samples | Distance from lateral epicondyle (in cm) | Distance from medial epicondyle (in cm) | Distance from biceps tendon (in cm) |
|---|
| Artico M et al., [12] | 2009 | 20 | 11 | 13.3 | |
| Carlan D et al.. [13] | 2007 | 27 | 10.9 | NA | |
| Chelly JE, [1] | 2009 | | | | 1-2 |
| Present study | 2020 | 50 | 12.1 | 12.4 | 1.75 |
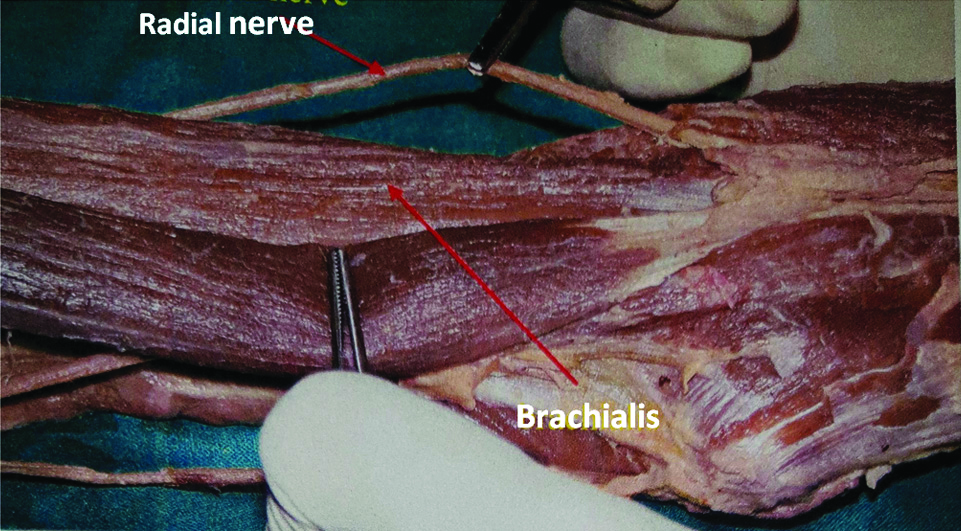
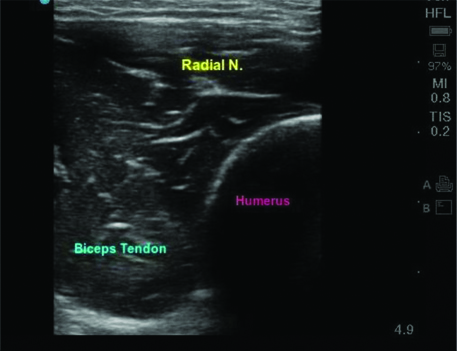
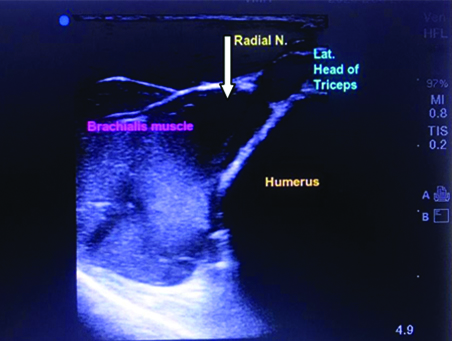
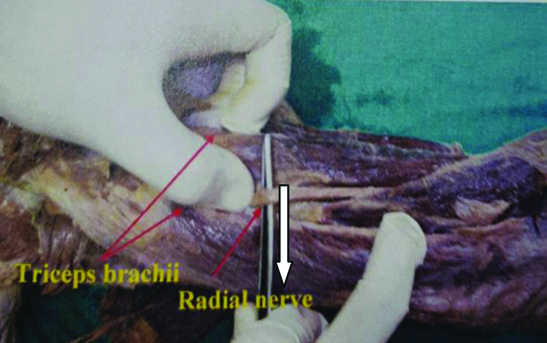
The radial nerve is best exposed by dissection above the lateral aspect of the elbow, where it lies between the brachioradialis and the brachialis muscles [Table/Fig-5]. The nerve divides into the superficial (sensory) and deep (motor) branches in the forearm [Table/Fig-6]. The nerve can be visualised by Ultrasonography 3-4 cm above the elbow crease. [Table/Fig-7a,b]. A single injection at this point blocks both the branches of the nerve. The nerve travels closer to the posterior surface of the humerus in the spiral groove [Table/Fig-8]. There was no variation observed in the course of the radial nerve in the upper limbs.
Radial nerve lying between brachialis and brachioradialis at the elbow.
Radial nerve dividing into superficial and deep branches in proximal forearm.

USG localisation of Radial nerve at the elbow.
USG localisation of Radial nerve where it pierces the Lateral Intermuscular Septum (LIS).
Radial nerve in the spiral groove.
Discussion
Radial nerve lies between the brachialis and brachioradialis muscles, 1 to 2 cm lateral to the biceps tendon at the elbow [1]. In the present study, the mean distance from the biceps tendon to the radial nerve at the elbow was 1.75±0.22 cm. The mean distances between the entry point of the nerve in the LIS and the medial and lateral epicondyles were 133±14 and 110±23 mm, respectively [12]. The radial nerve is prone to injury where it is in relation to the lateral aspect of the humerus in its distal third from 10.9 cm±1.5 proximal to the lateral epicondyle [13].
In the present study, the mean distance of the radial nerve from its entry in the LIS to the medial epicondyle was 12.4±0.31 cm [Table/Fig-2] and to the lateral epicondyle was 12.1±0.28 cm [Table/Fig-3], respectively
The results were compared with those of previous researchers [Table/Fig-4]. Most researchers have only measured the distance of the radial nerve in LIS to the lateral epicondyle [13]. But in the present study, distances from both epicondyles were measured. Researchers have measured the distance of the radial nerve to the triceps aponeurosis [14,15], but in index study, the distance from the biceps tendon was measured.
Clinical Implications
During surgical fixation of humeral fractures, identification and conservation of the radial nerve may avoid secondary nerve palsy. Improper plate fixation can result in transaction of the radial nerve by screws [16]. Distal-third diaphyseal fractures of the humerus are treated by modified posterior approach [17]. It is possible that the more extensive radial nerve exploration in this approach leads to a higher risk of radial nerve injury [18].
The nerve can be visualised by the Ultrasonography 3-4 cm above the elbow crease. A single injection at this point blocks both the branches of the nerve [11]. This is an important landmark to perform radial nerve block to achieve sensory anaesthesia in its terminal distribution. Such a peripheral nerve block of the radial nerve will be useful in minor surgical procedures in the areas supplied by the nerve. Ultrasound-guided radial nerve block will improve the proper localisation and also ensures safety and decreased duration of the procedure [11].
Landmark based techniques of peripheral nerve block in the upper limb have been restricted to sites at the elbow and wrist where surface landmarks are readily identified [8]. Injection at these levels carries the risk of neurovascular injury. Using ultrasound guidance, the local anaesthetic can be safely injected in other sites also without the risk of neurovascular injury. Variations in upper limb anatomy are commonly identified by ultrasonography. It also helps faster sensory onset of anaestheia, avoiding motor loss and greater block success compared with Landmark based techniques [19].
Hence, the present study will be useful to the Orthopaedic Surgeons to identify the radial nerve during surgical fixation of humeral shaft fractures and prevent it from being injured during surgeries. This study will be of use to the Anaesthesiologists to localise the radial nerve using surface landmarks like lateral and medial epicondyes, biceps tendon and also using ultrasound guidance during peripheral nerve blocks.
Limitation(s)
The present research study is limited by a small number of specimens and also the measurements were made from disarticulated limbs and hence, gender variation if any could not be found.
Conclusion(s)
A single terminal nerve occasionally needs block in addition to the brachial plexus block with local anaesthetic to have an adequate block for minor surgical procedures of the hand. From present study it can be inferred that effective peripheral blockade of the radial nerve can be achieved by blocking the nerve 1.75 cm lateral to the biceps tendon at the elbow 3 cm above the elbow crease.
Present study helps to understand the surgical anatomy of the radial nerve which would be of use to surgeons in order to avoid iatrogenic injuries to the adjacent neurovascular structures.
Mean±SD=1.75±0.22
Mean±SD=12.4±0.31
Mean±SD=12.18±0.28
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? NA
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jan 15, 2021
Manual Googling: May 15, 2021
iThenticate Software: May 20, 2021 (23%)
[1]. Chelly JE, Peripheral nerve blocks: A color atlas 2009 Lippincott Williams & Wilkins [Google Scholar]
[2]. Ip MC, Chang KS, A study on the radial supply of the human brachialis muscleThe Anatomical Record 1968 162(3):363-71.10.1002/ar.10916203114236202 [Google Scholar] [CrossRef] [PubMed]
[3]. Gray H, Standring S, Gray’s anatomy: The anatomical basis of clinical practice 2008 Churchill Livingstone [Google Scholar]
[4]. Dong Q, Jacobson JA, Jamadar DA, Gandikota G, Brandon C, Morag Y, Entrapment neuropathies in the upper and lower limbs: Anatomy and MRI featuresRadiology Research and Practice 2012 2012:23067910.1155/2012/23067923125929 [Google Scholar] [CrossRef] [PubMed]
[5]. Bumbasirevic M, Palibrk T, Lesic A, Atkinson HD, Radial nerve palsyEFORT Open Reviews 2016 1:286-94.10.1302/2058-5241.1.00002828461960 [Google Scholar] [CrossRef] [PubMed]
[6]. Cho H, Lee HY, Gil YC, Choi YR, Yang HJ, Topographical anatomy of the radial nerve and its muscular branches related to surface landmarksClinical Anatomy 2013 26(7):862-69.10.1002/ca.2211523090923 [Google Scholar] [CrossRef] [PubMed]
[7]. DeFranco MJ, Lawton JN, Radial nerve injuries associated with humeral fracturesThe Journal of Hand Surgery 2006 31(4):655-63.10.1016/j.jhsa.2006.02.01316632062 [Google Scholar] [CrossRef] [PubMed]
[8]. McCahon RA, Bedforth NM, Peripheral nerve block at the elbow and wristContinuing Education in Anaesthesia, Critical Care & Pain 2007 7(2):42-44.10.1093/bjaceaccp/mkm005 [Google Scholar] [CrossRef]
[9]. Jain RK, Champawat VS, Mandlecha P, Danger zone of radial nerve in Indian population- A cadaveric studyJ Clin Orthop Trauma 2019 10(3):531-34.Epub 2018 Feb 2110.1016/j.jcot.2018.02.00631061584 [Google Scholar] [CrossRef] [PubMed]
[10]. Prasad M, Issac B, Anatomic landmarks to identify the radial nerve during the posterior approach of the humerus: A cadaveric study prasanna samuel, premkumarJournal of Clinical and Diagnostic Research 2018 12(11):AC01-04.10.7860/JCDR/2018/37922.12275 [Google Scholar] [CrossRef]
[11]. Capek A, Dolan J, Ultrasound-guided peripheral nerve blocks of the upper limbBja Education 2015 15(3):160-65.10.1093/bjaceaccp/mku048 [Google Scholar] [CrossRef]
[12]. Artico M, Telera S, Tiengo C, Stecco C, Macchi V, Porzionato A, Surgical anatomy of the radial nerve at the elbowSurgical and Radiologic Anatomy 2009 31(2):101-06.10.1007/s00276-008-0412-818795220 [Google Scholar] [CrossRef] [PubMed]
[13]. Carlan D, Pratt J, Megan J, Patterson M, Weiland AJ, Boyer MI, The radial nerve in the brachium: An anatomic study in human CadaverJ Hand Surg Am 2007 32(8):1177-82.10.1016/j.jhsa.2006.07.00117923300 [Google Scholar] [CrossRef] [PubMed]
[14]. Arora S, Goel N, Cheema GS, Batra S, Maini L, A method to localise the radial nerve using the ‘Apex of Triceps Aponeurosis’ as a landmarkClin Orthop Relat Res 2011 469:2638-44.10.1007/s11999-011-1791-421286885 [Google Scholar] [CrossRef] [PubMed]
[15]. Hasan SA, Rauls RB, Cordell CL, Bailey MS, Nguyen T, “Zone of Vulnerability” for radial nerve injury: Anatomic studyJournal of Surgical Orthopaedic Advances 2014 23(2):105-10.10.3113/JSOA.2014.010524875341 [Google Scholar] [CrossRef] [PubMed]
[16]. Kinaci A, Kloen P, Videler A, Kreulen M, Unusual radial nerve injury by a locking compression plate for humerus fractureBMJ Case Rep 2014 2014:bcr201320151510.1136/bcr-2013-20151524862412 [Google Scholar] [CrossRef] [PubMed]
[17]. Páramo-Díaz P, Arroyo-Hernández M, Rodríguez Vega V, Aroca-Peinado M, León-Baltasar JL, Caba-Doussoux P, Surgical treatment of extra-articular distal-third diaphyseal fractures of the humerus using a modified posterior approach and an extra-articular plateRev Esp Cir Ortop Traumatol 2017 61(6):404-11.10.1016/j.recote.2017.10.00228890121 [Google Scholar] [CrossRef] [PubMed]
[18]. Shoji K, Heng M, Harris MB, Appleton PT, Vrahas MS, Weaver MJ, Time from injury to surgical fixation of diaphyseal humerus fractures is not associated with an increased risk of iatrogenic radial nerve palsyJ Orthop Trauma 2017 31(9):491-96.10.1097/BOT.000000000000087528459772 [Google Scholar] [CrossRef] [PubMed]
[19]. McCartney JL, Lin L, Shastri U, Evidence basis for the use of ultrasound for upper-extremity blocksReg Anaesth Pain Med 2010 35:S10-15.10.1097/AAP.0b013e3181d2567520216020 [Google Scholar] [CrossRef] [PubMed]