Hamstring are the group of biarticulate muscles traversing both hip and knee joint, arising from ischial tuberosity and inserting below the level of knee joint and help in knee flexion and hip extension [1]. Hamstrings form important part of core muscles and their tightness may reduce the lumbar lordosis [1]. Further, hamstring tightness has been associated with anterior knee pain, plantar fasciitis, and abnormalities in gait pattern [2]. A number of studies showed a temporal relation between presence of hamstring tightness and above mentioned abnormalities but fail to prove cause-effect relationship [1-5].
Orthopaedic surgeons have long working hours and at times they have to wear radiation protection equipment (Lead Apron). The literature has also shown that orthopaedic surgeons are prone to develop back pain [6,7]. Back pain is multifactorial and since hamstring tightness has been shown to be associated with LBP, it was thought to evaluate the prevalence of hamstring tightness among younger surgeons. This would also give a chance to target this population for remedial measures. Similar studies have also been conducted among other cohorts like physiotherapists, sedentary workers and college students [5,8-10].
This study was conducted with an aim to find prevalence of hamstring tightness in orthopaedic surgeons who do not suffer from back pain. The secondary objective of the present study was to find if hamstring tightness has any association with BMI.
Materials and Methods
This was a cross-sectional observational study conducted at a tertiary care centre from August 2020 to October 2020. The Helsinki declaration was respected and followed throughout the study. Informed consent was taken from all participants.
Inclusion criteria: All resident Orthopaedic surgeons (postgraduate students and senior residents) between ages 24-35 years were enrolled in the study. The study included only junior and senior residents as this group is young and were amiable to remedial measures.
Exclusion criteria: Those with pre-existing lumbar spine disease, history of hip or knee injury or any history of LBP in preceding year were excluded from the study.
Sample size calculation: Sample size calculation was done using power analysis n= Z2pq/d2 where, z was standard normal distribution, ‘p’ was known prevalence in previous study, ‘q’ was 1-p and ‘d’ is confidence interval. An alpha error of 5% was kept and known prevalence of hamstring tightness was used 82% [11]. Thus, a sample size of 57 was sufficient. The study however, enrolled 82 surgeons.
Study Procedure
The height and weight of the subjects were recorded using a standardised medical scale. BMI was calculated as per World Health Organisation (WHO) guidelines [12]. Four categories were established: underweight, normal, overweight, and obese. An individual would be considered to be underweight if his/her BMI was in the range of 15 to 19.9, normal weight if the BMI was 20 kg/m2 to 24.9 kg/m2, overweight if the BMI was 25 kg/m2 to 29.9 kg/m2, and obese grade 1 if it was 30 kg/m2 to 34.9 kg/m2 or grade 2 obesity: more than 35 kg/m2 [11]. Age and medical history were recorded using a questionnaire. Active knee extension angle were measured by method outlined by Yıldırım MS et al., with slight modification. Individuals were positioned in supine with the contralateral extremity in extension [3]. The ipsilateral hip and the knee were flexed to 90° flexion. Instead of originally described four straps by Yildirim MS et al., the study used two straps that were used for stabilisation as follows: the first strap was used to secure the subject’s contralateral thigh, a second strap on the subject’s iliac anterior spines was used to minimise the posterior pelvic tilt during the test [3]. No box for ischial support was used which obviated the use of third strap that were initially used to hold the box. Further, the fourth strap used by Yildirim MS et al., to stabilise ipsilateral thigh was not used in the present study. The authors in original description required four straps as they evaluated both active and passive knee extension angles. Since, this study did not warrant measurement of active angles the use of latter two straps was omitted. A 90 degree side support was used to restrict hyperflexion of hip. Following hip flexion to 90°, the knee was actively extended maximally for minimum of five seconds without any ankle dorsiflexion by the subject [Table/Fig-1].
a) View from top to show positioning of straps and 90 degree side bar with padding; b) Side view during measurement showing hip flexed to 90 degree with markings on thigh and leg axis; c) Knee extension angle after full active knee extension. The angle shown was regarded as knee extension angle.
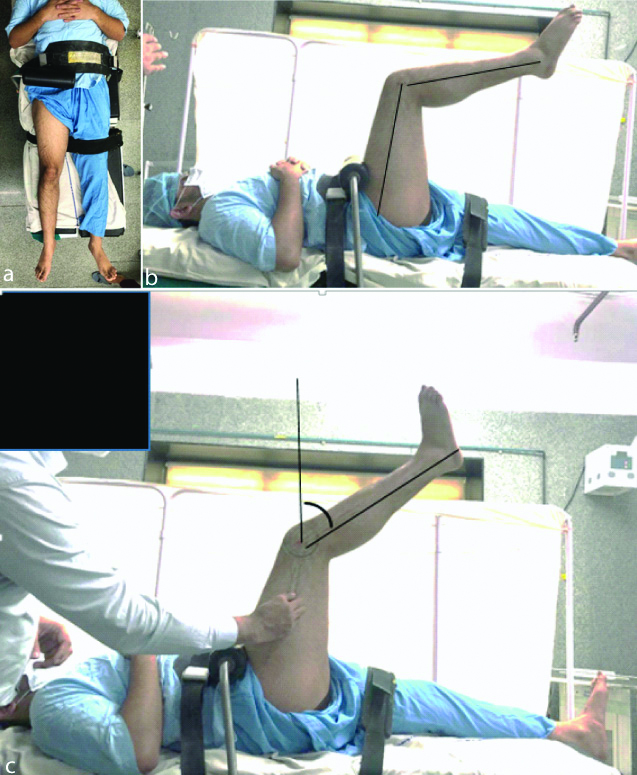
Knee extension angle was defined as the angle that the leg mid axis subtended with the vertical. The measurement was done by two independent orthopaedic consultant not involved in study on two different occasions, to minimise interobserver and intraobserver bias. There was a gap of 10 minutes between readings by two observers taken on the same day. The average of four readings was used as final reading [8]. Less than 20 degree was considered normal, 21-30 degree was regarded as mild tightness, 31-40 degree as moderate tightness and >40 degree as severe tightness [3].
Statistical Analysis
All quantitative data were expressed as mean±standard deviation. Statistical significance of differences in the mean values for categorical variables was determined using Chi-square test for categorical variables. Fischer-exact test replaced Chi-square test when one of the cells in categorical variables was zero. The percentages were calculated for factors not requiring comparison. Student t-test was used for continuous variables. Statistical Package for Social Sciences (SPSS) version 14.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. A p-value less than 0.05 was considered to indicate statistical significance.
Results
A total of 90 surgeons were considered for the study. Of these eight had episodes of lower back pain in last one year which were excluded from the study. All the 82 participants were males and were less than 35 years of age. The mean age was 27.2 years with standard deviation of 3.69. For interobserver reliability, the median weighted kappa statistic was 0.79 and for intraobserver reliability was 0.86, indicating high inter and intra observer reliability. Prevalence of hamstring tightness among Orthopaedic Surgeons in the series was 86.6%.
It was surprising that only 11 surgeons (13.4%) had no hamstring tightness on either side. Fourteen surgeons (17.1%) did not have any hamstring tightness on left side and 13 (15.8%) surgeons had no hamstring tightness on right side [Table/Fig-2] [13].
Hamstring tightness and the BMI [13].
| Variables | Number of volunteers (percentage) |
|---|
| Obesity* |
| Normal | 46 (56.1%) |
| Overweight | 28 (34.2%) |
| Obesity grade 1 | 6 (7.3%) |
| Obesity grade 2 | 2 (2.4%) |
| Knee extension angle-Right hamstring |
| Normal | 13 (15.8%) |
| Mild tightness | 21 (25.6%) |
| Moderate tightness | 35 (42.7%) |
| Severe tightness | 13 (15.9%) |
| Knee extension angle-Left hamstring |
| Normal | 14 (17.1%) |
| Mild tightness | 16 (19.5%) |
| Moderate tightness | 43 (52.4%) |
| Severe tightness | 9 (11%) |
*Obesity grading as per WHO: The WHO designations include the following: Normal- 18.5-24. 9 kg/m2; Overweight-BMI of 25-29.9 kg/m2; Grade 1 obesity-BMI of 30-34.9 kg/m2; Grade 2 obesity: 35-39.9 kg/m2 [13]
There was no side predominance for hamstring tightness and both sides were equally involved (p=0.67). The mean tightness on right side was 30.83 degree and left side was 31.11 degree. However, correlation was found between right and left-sided tightness (coefficient of correlation=0.901) i.e., surgeons with right-sided tightness also had left-sided tightness which was independent of dominant side. Further no relation was found between hamstring tightness and BMI. (Right side p=0.393, left p=0.160) [Table/Fig-3,4].
Relationship of obesity with left-sided hamstring tightness.
| Left hamstring tightness | BMI | Total |
|---|
| Normal weight | Over weight | Grade 1 obesity | Grade 2 obesity |
|---|
| Normal | 10 | 3 | 1 | 0 | 14 |
| Mild | 10 | 5 | 1 | 0 | 16 |
| Moderate | 23 | 17 | 3 | 0 | 43 |
| Severe | 3 | 3 | 1 | 2 | 9 |
| Total | 46 | 28 | 6 | 2 | 82 |
Relationship of obesity with left sided hamstring tightness.
| Right hamstring tightness | BMI | Total |
|---|
| Normal | Over weight | Grade 1 obesity | Grade 2 obesity |
|---|
| Normal | 9 | 3 | 1 | 0 | 13 |
| Mild | 14 | 5 | 2 | 0 | 21 |
| Moderate | 19 | 16 | 0 | 0 | 35 |
| Severe | 4 | 4 | 3 | 2 | 13 |
| Total | 46 | 28 | 6 | 2 | 82 |
Another interesting finding was that surgeons with no hamstring tightness were short in height compared to those with mild tightness (172±4.5 cm vs 178±6.2 cm) (p=0.025).
Discussion
For fitness and desirable musculoskeletal functioning, flexibility is one of the vital prerequisites [14]. Sedentary lifestyle leads to loss of flexibility of muscles [15]. Specifically, the muscles of the posterior leg, commonly known as the hamstring, have a greater tendency to shorten without proper conditioning [12,13]. Tightness among hamstring group of muscles leads to reduced range of motion and is also a causative factor for other musculoskeletal problems including increased pelvic tilt and increased lumbar and/or dorsal kyphosis. Hence, it is known to be associated with conditions such as herniated discs, spondylolisthesis, kyphosis and back pain [16]. Gonzalez-Galvez N et al., have shown that lack of flexibility in hamstring muscles is directly related with LBP in adults and adolescents [12]. Similar studies are done on other sedentary groups like physiotherapists and individuals involved in prolonged desk jobs [8,9]. Young resident orthopaedic surgeons are usually involved in long working hours and therefore, have less time for conditioning hamstring exercises so this study was planned to determine the prevalence of hamstring tightness in young resident orthopaedic surgeons. The most important finding of the study is that a large majority of young orthopaedic surgeons had hamstring tightness. Further, the tightness was not related to BMI. This points towards urgent need to appraise young surgeons regarding high prevalence of hamstring spasm.
Shakya NR and Manandhar S, studied 107 physiotherapist and found that 40% of them had hamstring tightness [8]. Pradeep B et al., in their study on sedentary workers between 35-55 years of age, showed active knee extension angle was less than 20 degree in 31.6% on right side and 35% on left side [9]. Similar to the lifestyle of physiotherapists and desk workers in above study, the young resident orthopaedic surgeons have a sedentary lifestyle with limited time for exercises due to their busy schedule. The present study shows hamstring tightness to be more prevalent in resident orthopaedic surgeons compared to above studies [8,9], also it is important to note that the mean age of present study was less than above studies. This further shows that the condition is more dismal than realised.
Similar to the findings of Rose S and Thakur D who evaluated prevalence of hamstring tightness among college students, the present study also found that there was a significant correlation between the right and left hamstring muscle tightness. However, statistical tests of significance failed to prove if one side tightness was more prevalent than other side [10]. Koli BK and Anap DB who evaluated hamstring tightness among college students, found that amongst patients with hamstring tightness, 38% had high BMI but the present study found that there was no correlation between BMI and tightness [5].
The literature is lacking on relationship between height and hamstring tightness. Even though the present study shows statistical significance between height and hamstring tightness groups, its clinical implication owing to small sample size of the study, cannot be determined. Further larger studies may be required to see if taller people in general have more hamstring tightness than shorter people.
This is probably the first study to determine the prevalence of hamstring tightness among young resident orthopaedic surgeons. It is believed that busy schedule of resident surgeons, long hours of surgery, use of lead aprons coupled with lack of exercises put this group at risk of LBP. Hamstring tightness has been related to back pain in various studies [1,2]. The present study shows that hamstring tightness starts to occur at an early age. The present study provides the evidence that the measures should be taken to educate and provide timely intervention for young orthopaedic surgeons who are prone to develop back pain.
Limitation(s)
All participants were males and sample size was relatively small. Further multicentric studies are required to identify if hamstring tightness is more prevalent among orthopaedic surgeons compared to general population. It is a cross-sectional study and therefore, selection bias cannot be ruled out.
Conclusion(s)
Prevalence of hamstring tightness is very high among young orthopaedic surgeons. Since the condition is known to be related to LBP, the administration should pay more attention to the ergonomics and physical environment in which the training of next generation surgeons is conducted. The young resident orthopaedic surgeons should be made aware of the burden of the condition and they should be encouraged to do conditioning exercises to prevent the adverse effects of tight hamstring at later age.
*Obesity grading as per WHO: The WHO designations include the following: Normal- 18.5-24. 9 kg/m2; Overweight-BMI of 25-29.9 kg/m2; Grade 1 obesity-BMI of 30-34.9 kg/m2; Grade 2 obesity: 35-39.9 kg/m2 [13]