Successful Management of Renal Fusion Anomaly of Kidney with Nephrolithiasis and Urinary Incontinence
Sunirmal Choudhury1, Ankit Sandhu2, Dilip Kumar Pal3
1 Associate Professor, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
2 PDT MCH, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
3 Professor and Head, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Institute of Postgraduate Medical Education and Research, 244, AJC Bose Road, Kolkata-700020, West Bengal, India.
E-mail: drdkpal@yahoo.co.in
The presence of an ectopic ureter may be indicated by continuous wetting, seen especially in girls. In majority of such cases, an ectopic ureter is associated with a duplex collecting system and complete ureteral duplication. A 32-year-old female presented with urinary incontinence with normal voiding episodes and right flank pain. On investigation, she was found to have duplex moiety on the right-side with partially duplicated ureter and quadruple moiety on the left-side with partially duplicated quadruple ureter with ectopic opening of ureters. The patient also had right upper calyceal stone. It was successfully managed with totally minimal invasive technique with retrograde intrarenal surgery for right nephrolithiasis and left laparoscopic ureteric reimplantation for ectopic ureter. Patient was continent during the follow-up period of nine months with no significant complications. Developmental anomalies of kidney and ureter though rare, can be managed with total minimal invasive techniques, requires proper planning, instruments and its implementation.
Calyceal stone, Duplex moiety, Ectopic ureter, Intrarenal surgery, Quadruple moiety
Case Report
A 32-year-old young unmarried female presented to the Urology Outpatient Department (OPD) with complaints of urinary incontinence and continuous leakage of urine per urethra with intermittent normal voiding episodes since birth and mild right flank pain, for last one year. She complained of 4-6 pad soakage daily since birth. She had poor quality of life due to continuous wetting. She had no significant medical, surgical and family history.
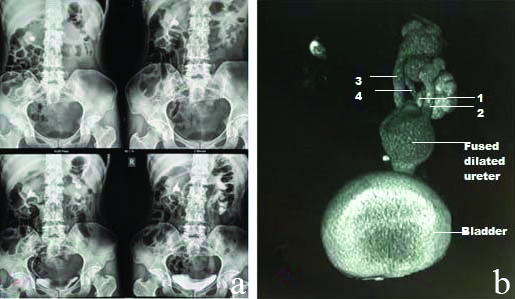
Abdominal examination was unremarkable. Pelvic examination showed urine pooling in the vaginal vault and no pelvic organ prolapse. On Computed Tomography (CT) kidney urinary bladder and CT urography, she was found to have right partially duplicated collecting system with upper calyceal stone and left quadruple collecting system with bilateral ectopic opening with decreased left renal function. Right ureter opened with common sheath just above bladder neck. Left ureters fused at L5 level to open with single ectopic opening at distal urethra. Blood parameters revealed urea-44 mg/dL, creatinine-1 mg/dL. Ultrasonography suggested right nephrolithiasis with left hydroureteronephrosis. Intravenous urography and CT urography revealed right nephrolithiasis (1.5×1 cm) at upper calyx, left-sided grade IV hydronephrosis with pelvicalyceal system dilatation with quadruple moiety and dilated left ureter [Table/Fig-1]. Cystoscopy and Retrograde Pyelography (RGP) revealed right-side double moiety kidney with stone and left-side quadruple moiety. Right ureteric orifice was seen just above bladder neck and left ureteric orifice opening at distal urethra. On renal DTPA scan, the left kidney had Glomerular Fiteration Rate (GFR) of 16.53 with differential function of 28.57% and right kidney had GFR of 41.45 with differential function of 71.49%.
a) Intravenous Pyelogram (IVP) showing right nephrolithiasis with decreased left function; b) CT Urography showing left-sided quadruple moiety. 1,2,3,4 are four partially duplicated ureters fusing to form single dilated ureter.
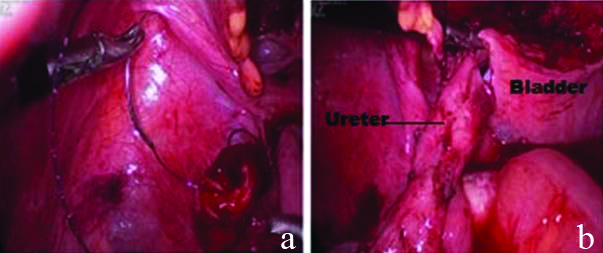
Patient underwent staged operation as stone clearance was challenging due to its location in upper calyx. Right ureterorenoscopy with DJ stenting followed by right Retrogradeintrarenal Surgery (RIRS) using olympus flexible fibreoptic ureteroscope was done followed by laser lithotripsy and complete stone clearance was achieved. It was followed by laparoscopic left ureteric reimplantation to salvage the left kidney. Steps of standard laparoscopic dissection followed and left extravesical ureteric reimplantation (modified Lich Gregoir) was done over posterior surface of bladder after placing a 5 Fr- 26 cm DJ stent [Table/Fig-2].
Laparoscopic left ureteric re implantation, (a and b).
The RIRS took 70 minutes and complete stone clearance was achieved. It was followed by left laparoscopic ureteric reimplantation which took 130 minutes and with minimal blood loss. There was no perioperative surgical complication. Drain was removed on day three. Per urethral catheter was removed at postoperative day seven. Bilateral DJ stent were removed after six weeks of surgery. Patient was followed-up for nine months and was found to be continent with no complications.
Discussion
An ectopic ureter is defined as a ureter, single or duplex, opening at position other than trigone. Incidence is about 1:2000 and 1:4000 in autopsies [1]. Ureteral duplication has an incidence rate of 0.7% in the population [2]. Ectopic ureter implantation, with an incidence rate of 0.05-0.025% in the population is relatively rare [3].
Ectopic ureter is usually associated with duplex system but having duplex moiety on one side and quadruple moiety on other side is rare. During embryogenesis, the urogenital system and the reproductive system develop from the intermediate mesoderm. When two separated buds arise from a single Wolffian duct; it results in two ureters draining a single kidney. Ureteral duplication can be partial or complete, the latter being most common in 70% of the cases [4]. In case of partial ureteral duplications, which occur due to ureteral bud splitting, result in one ureter ending normally into the bladder and the other being ectopic, ending in the urethra, vulval vestibule [5,6]. In the present case, there was bilateral ectopic opening with the right opening just above bladder neck and left opening in the distal urethra.
A complete ureteral duplication is usually associated with ectopic ureterocele with or without vesicoureteral reflux and ectopic ureteral insertion. Urinary incontinence and enuresis in childhood may be associated with the ectopic ureteral insertion distal to the bladder neck or external sphincter. The patient usually seeks treatment in childhood but in our case due to low economic status patient did not seek treatment until now. According to the Weigert-Meyer law, in case of complete ureteral duplication, the upper moiety ureter inserts into the urinary bladder inferiorly and medially predisposing to ureterocele and obstruction whereas the lower moiety ureter inserts into the urinary bladder more superiorly and laterally predisposing to vesicoureteric reflux [7]. In this case as right-sided ureter opening was above bladder neck, patient had normal voiding episodes, thus right-sided ureteric reimplantation was not required.
Left-side kidney had quadruple moiety draining by four ureters which fuses at L3 vertebra level and opens at ectopic position in distal urethera which was the cause for urinary incontinence. No such study that includes quadruple moiety on one side kidney and double moiety on other side kidney has been reported so far and when encountered poses difficulty in management. Such anomaly and its sequential totally minimal invasive management have never been reported before.
Ultrasound is usually the imaging of choice in the initial assessment, as it is widely available, non invasive and low-cost. It usually detects major abnormalities, such as an ureterocele or hydronephrosis but small abnormalities can be missed. IVP and voiding cystourethrography are helpful in delineating the course of the ureter and its insertion site. In this case, the diagnosis was made using IVP and contrast CT scan, which showed a duplicated collecting system on the right-side with nephrolithiasis and quadruple system on left-side with ectopic opening of both ureters. In cases with equivocal results with CT urogram, direct contrast injection in the dilated ureter may be helpful [8].
The Magnetic Resonance (MR) urogram is considered to be the modality of choice, since it is able to visualise complex urogenital anomalies with excellent imaging of the kidney, ureteral tract and insertion site [9]. Furthermore, there is no risk of radiation exposure. In the present study, MR Urogram was not done as the diagnosis was evident on CT urography and cystoscopy findings.
The best treatment is surgery as it resolves the incontinence, prevent further complications and preserve renal function. Surgical treatment includes upper pole heminephrectomy for non functional duplex system, open or laparoscopic ureteral reimplantation, ligation or clipping depending upon situation [10].
Duicu C et al., reported a case of double collecting system with ipsilateral ectopic opening into vagina in five-year-old female. They did open enbloc reimplantation of ectopic ureters [11]. Hisano M et al., reported a case series of duplex system in four females presenting with urinary incontinence which were managed by laparoscopic ureteropyeloanastomosis of the upper pole ureter to the pelvis of the lower moiety, with prior insertion of a double J stent [12].
Conclusion(s)
This is a unique case of a middle-aged woman presenting with urinary incontinence and right-side nephrolithiasis with right-side duplicated system with partial duplication of ureter and left-side quadruple system with four ureters draining the moiety independently but then fuse together with ectopic opening in urethra. As left-sided ureter was the cause of incontinence so it was dealt with left ureteric reimplantation. Right-sided nephrolithiasis was managed by minimal invasive procedure. This is probably the first case report of sequential minimal invasive management of rare anomaly of kidney with quadruple moiety of ureter presenting with complications as urinary incontinence and nephrolithiasis.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Dec 18, 2020
Manual Googling: Feb 13, 2021
iThenticate Software: May 22, 2021 (19%)
[1]. Albers P, Foster RS, Bihrle R, Adams M, Keating MA, EUs and ureteroceles in adultsUrology 1994 45:870-74.10.1016/S0090-4295(99)80098-3 [Google Scholar] [CrossRef]
[2]. Gay SB, Armistead JP, Weber ME, Williamson BR, Left infrarenal region: Anatomic variants, pathologic conditions, and diagnostic pitfallsRadiographics 1991 11(4):549-70.10.1148/radiographics.11.4.18871111887111 [Google Scholar] [CrossRef] [PubMed]
[3]. Demir M, Çiftçi H, Kiliçarslan N, Gümüş K, Oğur M, Gülüm M, A case of an ectopic ureter with vaginal insertion diagnosed in adulthoodTurk J Urol 2015 41(1):53-55.10.5152/tud.2014.8156726328201 [Google Scholar] [CrossRef] [PubMed]
[4]. Berrocal T, López-Pereira P, Arjonilla A, Gutiérrez J, Anomalies of the distal ureter, bladder and urethra in children: Embryologic, radiologic, and pathologic featuresRadioGraphics 2002 22(5):1139-64.10.1148/radiographics.22.5.g02se10113912235344 [Google Scholar] [CrossRef] [PubMed]
[5]. Fernbach S, Feinstein K, Spencer K, Lindstrom C, Ureteral duplication and its complicationsRadioGraphics 1997 17(1):109-27.10.1148/radiographics.17.1.90178039017803 [Google Scholar] [CrossRef] [PubMed]
[6]. Sadler T, Langman J, Langman’s Medical Embryology 2010 Philadelphia, PaWolters Kluwer Health in Lippincott William & Wilkins [Google Scholar]
[7]. Denver PS, George T, Saxena D, Joseph T, Hoisala VR, Ureteral reflux into an ectopic ureter moiety of a duplex kidney from the bladder neck with distal ureteral pseudodiverticulum formationJournal of Clinical and Diagnostic Research 2016 10:07-09. [Google Scholar]
[8]. Croitoru S, Gross M, Barmeir E, Duplicated ectopic ureter with vaginal insertion: 3D CT urography with IV and percutaneous contrast administrationAm J Roentgen 2007 189(5):W272-74.10.2214/AJR.05.143117954624 [Google Scholar] [CrossRef] [PubMed]
[9]. Liu L, Yang J, Zhu L, Yi L, Zhu B, Song W, Crossed-fused renal ectopia associated with inverted-Y ureteral duplication, ectopic ureter, and bicornuate uterusesUrology 2010 75(5):1175-77.10.1016/j.urology.2010.02.03720347478 [Google Scholar] [CrossRef] [PubMed]
[10]. Romao RL, Figueroa V, Salle JL, Koyle MA, Bägli DJ, Lorenzo AJ, Laparoscopic ureteral ligation (clipping): A novel, simple procedure for pediatric urinary incontinence due to ectopic ureters associated with non-functioning upper pole renal moietiesJ Pediatr Urol 2014 10(6):1089-94.10.1016/j.jpurol.2014.04.00824881807 [Google Scholar] [CrossRef] [PubMed]
[11]. Duicu C, Kiss E, Simu I, Aldea C, A rare case of double-system with ectopic ureteral openings into vaginaFront Pediatr 2018 6:17610.3389/fped.2018.0017629974045 [Google Scholar] [CrossRef] [PubMed]
[12]. Hisano M, Denes FT, Brito AH, Lucon M, Machado MG, Bruschini H, Laparoscopic ureteropyeloanastomosis in the treatment of duplex systemInt Braz J Urol 2012 38(2):235-41.10.1590/S1677-5538201200020001222555029 [Google Scholar] [CrossRef] [PubMed]