A multitude of pathologic conditions originating from the lumbar spine can contribute to a variety of signs and symptoms. The spectrum of lumbar spine pathologies includes degenerative, traumatic, infectious, neoplastic, congenital, inflammatory, autoimmune, and vascular [1]. The most common of these pathologies is the lumbar spondylosis, which is a degenerative process of the spine leading to spinal cord compression and canal narrowing [2]. With increasing age, the discs progressively dehydrate resulting in desiccation, which is seen on MRI as decrease in T2 signal and can be seen even in asymptomatic patients. Numerous studies have reported lumbar spine abnormalities to be more frequent in the female population when compared with their male counterparts [3-5]. However, de Schepper EIT et al., reported that males were highly affected in their study with lumbar pathologies [6].
MRI currently, is an excellent imaging modality of choice for the demonstration of pathologies of the lumbar spine and the intervertebral disc. It can outline soft tissues; it is non-invasive, and has multi-planar imaging capabilities with no ionizing radiations [7]. Most studies in our locality focused on low back pain as it relates to degenerative changes [8,9]. None of these reports evaluated the general pathologies of the lumbar spine. A sound knowledge of the common pathologies of the lumbar spine in our setting will assist clinicians and radiologist in making accurate diagnosis. To the best of our knowledge, there is dearth of report on the MRI findings in patients with lumbar spine pathologies in our locality. Hence, this study was undertaken with the aim to determine the type and distribution of MRI findings in lumbar spine pathologies in Rivers State and to correlate with the demographic variables.
Materials and Methods
This was an observational cross-sectional study carried out from May 2020 to November 2020 among all symptomatic and asymptomatic patients who were referred for lumbar spine MRI at two selected Imaging Diagnostics Centres in Rivers State, which were selected purposively based on that fact the two centres have MRI machine of the same field strength of 0.35 Tesla.
Ethical approval (UPTH/ADM/90/SII/VOL.XL/897) was obtained from the Human Research and Ethic committee of University of Port Harcourt Teaching Hospital, River State, Nigeria. Permission for this study was also obtained from the various study centers. The patients were informed about the purpose of this study and their consent was properly sought, and obtained. The nature of their participation was entirely voluntary.
Inclusion and Exclusion criteria: Patients who gave properly filled request forms with complete patient demographic information such as gender, age, and clinical indications were included in the study. Only patients diagnosed with lumbar spine pathologies were included in this study while those with normal findings on MRI were excluded.
Sample size calculation: The sample size of 151, was determined using Yamane T [10] formula:

Where n=desired sample size
N=population of study
e=accepted error limit (0.05)
From the radiological reports’ archives of the study centers, a total population of 243 patients underwent lumbar spine MRI from May 2019 to April 2020.
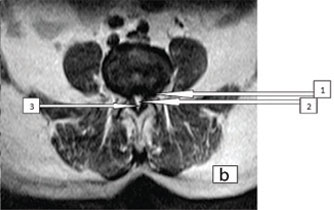
The lumbar spine MRI examinations were performed using open type 0.35 Tesla MRI machines (Brivo MR235, General Electric, and Siemens Magnetom C) using both planar surface and multicoil phased array. The patients were examined lying supine with head first, arm beside and the body in a neutral position. Fast spin-echo sequence was used to obtain T1 and T2 weighted images in axial and sagittal planes. Short Tau Inversion Recovery (STIR) sequences were also acquired for adequate assessment of the spine. The imaging parameters were; T1W sagittal image: Repetition Time (TR)/Time of Echo (TE)=337-495/15-19, Field of View (FOV)=240 mm-260 mm, slice thickness=4-5 mm, Flip angle=900, matrix size=206×256 and number of excitation (Nex)=3-4, and T2W sagittal image: TR/TE=3200-4700/110-125, FOV=240-260 mm, slice thickness=4-5 mm, Nex=3-4 and Flip angle=900. Axial images (T1W: TR/TE=257-457/13-18, FOV=240×240 mm, slice thickness=4-5 mm, Nex=3-4 and flip angle=900 and T2W: TR/TE=2221-3400/120-125, FOV=240×240 mm, slice thickness=4-5 mm, Nex=3-4 and Flip angle=900. The acquired images were interpreted by atleast two consultant radiologists with more than three years of experience in MRI spine reporting [Table/Fig-1,2].
T2W sagittal, Sagittal plane showing lumbar spondolytic changes.

Axial MR images respectively (Arrows: 1=narrowing of neural canal with impingement on the exit nerve root, 2=spinal canal stenosis and 3=ligamentum flavum hypertrophy).
The patients were evaluated for disabilities using the Nurick grading classifications [11];
0: Signs or symptoms of root involvement but without evidence of spinal cord disease.
1: Signs or symptoms of spinal cord disease but no difficulty in walking.
2: Slight difficulty in walking but does not prevent full-time employment.
3: Difficulty in walking which prevented full-time employment or ability to do all household work but which was not enough to require somebody’s help to walk.
4: Able to walk only with someone else’s help or with aid of a frame.
5: Chair bound or bedridden.
The grading information, socio-demographic variables such as gender, age, marital status and occupation (professionals: teacher, lawyers, accountants etc., and non-professionals: masons, mechanics, carpenters etc.,) and educational status were obtained via mini-interview using proforma designed according to the study objectives. The imaging findings used for this study were retrieved from the MRI reports and were categorised into levels of spinal involvement (single, double, and multiple) and types of pathology.
Statistical Analysis
Both descriptive and inferential (Pearson’s correlation test) statistics were done using Statistical Package For Social Sciences (SPSS) version 21.0 (SPSS, Inc Ill USA, 2003). The Pearson’s Correlation test was done to evaluate the correlations between the demographic variables (age and gender) and the classified pathologies and the duration of pathology, and the Nurick grading scales using Pearson’s correlation test. The level of statistical significance was set at p<0.05.
Results
Out of 151 patients that were included in this study, majority 78 (51.7%) of the patients were within the age group of 40-59 years with an overall mean age of 52.51±14 years. Males were more in number 91 (60.26%) when compared with their female counterparts 60 (39.74%). Large number 86 (56.95%) of the patients were non-professionals [Table/Fig-3].
Socio-demographic variable of the patients (N=100).
| Socio-demographic variables | Frequency (n) | Percentage (%) |
|---|
| Gender |
| Male | 91 | 60.26 |
| Female | 60 | 39.74 |
| Age group (Years) |
| <20 | 2 | 1.3 |
| 20-39 | 50 | 33.1 |
| 40-59 | 78 | 51.7 |
| 60 and above | 21 | 13.9 |
| Marital status |
| Married | 102 | 67.55 |
| Single | 42 | 27.81 |
| Divorced | 1 | 0.67 |
| Spouse diseased | 6 | 3.97 |
| Occupation |
| Professionals | 65 | 43.05 |
| Non-professionals | 86 | 56.95 |
| Educational status |
| Tertiary | 67 | 44.37 |
| Secondary | 38 | 25.17 |
| Primary | 29 | 19.21 |
| None | 17 | 11.26 |
Majority 114 (75.50%) of the patients had single pathology and the least 15 (9.93%) had multiple pathologies. Among those that had single pathology, a greater proportion 65 (43.05%) had spondylosis [Table/Fig-4].
Frequency and percentage distributions of lumbar spine pathologies.
| Lumbar pathologies | Frequency | Percentage (%) |
|---|
| Single pathology |
| Spondylosis | 65 | 43.05 |
| Disc hemiations | 8 | 5.3 |
| Exit nerve root compression | 7 | 4.6 |
| Facetal arthrosis | 3 | 2 |
| Fat marrow changes | 3 | 2 |
| Ligamentum fava hypetrophy | 3 | 2 |
| Narrowing of neural foramina | 8 | 5.3 |
| Wedge collapse of vertebrae | 1 | 0.7 |
| Radiculopathy | 1 | 0.7 |
| Retrolisthesis | 1 | 0.7 |
| Spinal canal stenosis | 5 | 3.3 |
| Spondylolisthesis | 9 | 5.96 |
| Double pathology |
| Retrolisthesis, spondylosis | 4 | 2.6 |
| Exit nerve root compression, spinal canal stenosis | 4 | 2.6 |
| Fat marrow change, spondylosis | 2 | 1.3 |
| Ligamentum fava hypetrophy, Spondylosis | 2 | 1.3 |
| Narrowing of neural foramina, spinal canal stenosis | 4 | 2.6 |
| Spinal canal stenosis, exit nerve root compression | 3 | 2 |
| Spindylosis, radiculopathy | 1 | 0.7 |
| Spondylosis, fat marrow changes | 2 | 1.3 |
| Multiple pathologies |
| Disc herniation, spinal canal stenosis, exit nerve root compression | 15 | 9.9 |
| Total | 151 | 100 |
There were positive correlations but statistically non-significant relationships between the pattern’s pathology with patient’s gender. There were positive correlations and statistically significant relationships between the patterns of pathologies and the patient’s age group [Table/Fig-5].
Correlations between the patterns of pathologies and demographic variables.
| Patterns of pathologies | Gender | Age group |
|---|
| r | p | r | p |
|---|
| Single pathology | 0.214 | 0.091 | 0.361 | 0.012 |
| Double pathologies | 0.718 | 0.061 | 0.514 | 0.003 |
| Multiple pathologies | 0.628 | 0.073 | 0.946 | 0.001 |
Pearson’s correlation analysis, significance (p<0.05) and Non-significance (p<0.05)
A greater proportion 73 (48.34%) of the patients had single level of spinal involvement with the fourth lumbar vertebra being commonly affected 26 (17.22%). There were positive correlations and statistically significant relationships between double levels of spinal involvement (r=0.561, p=0.021) and multiple levels of spinal involvement (r=0.631, p=0.001) with non-professional category of the patients [Table/Fig-6].
The correlations between spinal levels of involvement and the patient’s occupations.
| Spinal levels | Frequency n (%) | Occupation |
|---|
| Professionals | Non-professionals |
|---|
| r | p | r | p |
|---|
| Single | | 0.761 | 0.086 | 0.251 | 0.061 |
| L1 | 6 (3.97) | | | | |
| L2 | 10 (6.62) | | | | |
| L3 | 13 (8.61) | | | | |
| L4 | 26 (17.22) | | | | |
| L5 | 18 (11.92) | | | | |
| Double | | 0.346 | 0.063 | 0.561 | 0.021 |
| L1/L2 | 5 (3.31) | | | | |
| L2/L3 | 9 (5.96) | | | | |
| L3/L4 | 12 (7.45) | | | | |
| L4/L5 | 21 (13.91) | | | | |
| L2/L4 | 11 (7.28) | | | | |
| L3/L5 | 6 (3.97) | | | | |
| Multiple | | 0.813 | 0.093 | 0.631 | 0.001 |
| L1/L3/L4 | 1 (0.66) | | | | |
| L2/L4/L5 | 4 (2.45) | | | | |
| L3/L4/L5 | 7 (4.64) | | | | |
| L4/L5/S1 | 2 (1.32) | | | | |
| Total | 151 (100%) | | | | |
Out of 151 patients, the majority 49 (32.45%) had Nurick grade II and the least 7(4.64%) had Nurick grade V. A greater number of the patients with Nurick grade II that is 26 (17.22%) were within the age group of 40-59 years. Males among those that had Nurick grade II were highest in number 38 (25.17%). Out of 42 patients that had 2-3 years duration of pathology, the majority 12 (7.95%) had Nurick grade IV [Table/Fig-7].
Frequency Distribution of Nurick grades among gender, age group and durations of pathology.
| Variables | Nurick grades classifications n (%) | Total |
|---|
| I | II | III | IV | V |
|---|
| Gender |
| Male | 29 (19.21) | 38 (25.17) | 14 (9.27) | 9 (5.96) | 1 (0.67) | 91 (60.28) |
| Female | 8 (5.30) | 11 (7.28) | 15 (9.93) | 20 (13.24) | 6 (3.97) | 60 (39.72) |
| Total | 37 (24.50) | 49 (32.45) | 29 (19.21) | 29 (19.21) | 7 (4.64) | 151 (100%) |
| Age group (years) |
| <20 | - | 2 (1.32) | - | - | - | 2 (1.32) |
| 20-39 | 7 (4.64) | 20 (13.24) | 13 (8.61) | 10 (6.62) | - | 50 (33.11) |
| 40-59 | 21 (13.91) | 26 (17.22) | 15 (9.93) | 16 (10.60) | - | 78 (51.66) |
| 60 and above | 9 (5.96) | 1 (0.66) | 1 (0.66) | 3 (1.99) | 7 (4.64) | 21 (13.91) |
| Total | 37 (24.50) | 49 (32.45) | 29 (19.21) | 29 (19.21) | 7 (4.64) | 151 (100%) |
| Duration of pathology |
| <6 months | 12 (7.95) | 8 (5.30) | 2 (1.32) | 7 (4.64) | 3 (1.99) | 32 (21.19) |
| 6 months- 1 years | 4 (2.65) | 21 (13.91) | 12 (7.95) | 2 (1.32) | - | 39 (25.82) |
| 1year- 2 years | 10 (6.62) | 9 (5.96) | 7 (4.64) | 8 (5.30) | 4 (2.65) | 38 (25.17) |
| 2 years-3 years | 11 (7.28) | 11 (7.28) | 8 (5.30) | 12 (7.95) | - | 42 (27.81) |
| Total | 37 (24.50) | 49 (32.45) | 29 (19.21) | 29 (19.21) | 7 (4.64) | 151 (100%) |
There were positive correlations but non-statistically significant relationships between Nurick grades and the patients’ gender. There was a negative correlation but statistically significant relationship between Nurick grade I (r=-0.735, p=0.002) and age group. There were positive correlations and statistically significant relationships between Nurick grades (II: r=0.961, p=0.001; IV: r=0.112, p=0.024 and V: r=0.415, p=0.010) and the patient’s age group. There were positive correlations and statistically significant relationships between Nurick grades (I: r=0.124, p=0.041; II: r=0.321, p=0.003; III: r=0.421, p=0.001; IV: r=0.312, p=0.031 and V: r=0.213, p=0.001) and duration of pathology [Table/Fig-8].
Correlations between Nurick grades and gender, age and duration of pathology.
| Nurick grading scores | Gender | Age group | Duration of pathology |
|---|
| r | p | r | p | r | p |
|---|
| 0 | - | - | - | - | - | - |
| I | 0.641 | 0.092 | -0.735 | 0.002 | 0.124 | 0.041 |
| II | 0.214 | 0.063 | 0.961 | 0.001 | 0.321 | 0.003 |
| III | 0.918 | 0.094 | 0.310 | 0.092 | 0.421 | 0.001 |
| IV | 0.714 | 0.061 | 0.112 | 0.024 | 0.312 | 0.031 |
| V | 0.817 | 0.071 | 0.415 | 0.010 | 0.213 | 0.001 |
Discussion
In this study, the fourth lumbar vertebra (L4) was the most commonly affected spinal level. This is because this level of vertebrate bears the weight of an individual, and so it is usually prone to abnormalities. Both double and multiple levels of spinal involvements showed statistically significant correlations with the professional category of the patients. This implies that the nature of one’s profession and the associated activities has serious effect on the levels of the spinal involvement thereby causing more than one level of spinal abnormalities.
The majority of the patients in present study had Nurick grade II, which means that they had slight difficulty in walking but they were not prevented from full employment. Among those that had Nurick grade II, males were highest when compared to their female counterparts. This could be attributed to the fact that males involved most in strenuous activities, which exposes them more to lumbar spinal abnormalities. There were positive correlations but non-statistically significant relationships between Nurick grade I, II, III, IV and V, and patients’ gender while there were positive correlations and statistically significant relationships between Nurick grades II, III, IV and V, and the patients’ age. These implies that although, the patient’s gender may influence the nature of disabilities associated with lumbar spine pathologies, it has no statistically evidence while age has so much influence on the Nurick grade types and is justified statistically.
In this study, the majority of the patients were males. This finding is in resonance with the findings of the studies conducted by Uduma U et al., [7] in Cameroon, Iyidobi EC et al., [9], and Irurhe NK et al., [12] in Nigeria, which also reported higher numbers of males than females. Author presumed that the male preponderance noted in this study could be ascribed to the fact that males are the most active members of the human society and equally involved in strenuous activities, which predisposes them to lumbar spine abnormalities when compared to their female counterparts. Present study finding is at variance with the findings of the studies carried by Ajiboye LO et al., and Adekanmi AJ et al., in other parts of Nigeria, which reported female preponderance [13,14]. The discrepancies in present study findings could be attributed to the different sample sizes studied and the nature of the various studies.
A greater number of the patients were within the 40-59 years of age with an overall mean age of 52.5±14 years. This finding was in consonance with the results of the studies conducted by Ebubedike UR et al., Iyidobi EC et al., Irurhe NK et al., in Nigeria, Skaf GS et al., Saleem S et al., and Karunanayake A et al., which also reported patients within the 4th-5th decades of life [8,9,12,15-17]. The differences in the absolute values of present study findings could be ascribed to the variations in the sample sizes.
In this study, results revealed that the majority of the patients had single pathology with lumbar spondylosis as the most common pathological entity. This finding was in harmony with the findings of the studies conducted by Adekanmi AJ et al., and Laxton AW and Perrin RG which also reported lumbar spondylosis as the most common pathology in their studies [14,18]. This finding was inconsistent with the finding of the studies conducted by Maaji SM et al., which reported disc prolapsed and spinal stenosis respectively to be the most common pathology [2]. The discrepancies in present study findings could be attributed to different sample sizes as well as the variations in the nature of the studies. There were positive but non-statistically significant relationships between pathologies and the patients’ gender. This implies that though the occurrence of lumbar spine pathologies may be related to gender, it has no statistical evidence. This finding was in harmony with the findings of the studies carried out by Ebubedike UR et al., and Adekanmi AJ et al., which equally reported non-statistically significant relationships between spinal pathologies and patients’ gender [8,14]. A good knowledge of lumbar spine pathologies taking cognizance of demographic variables is vital to the management of these patients. Authors recommend proper grading of disabilities emanating from lumbar spine pathologies to prevent aggravation as it may affect productivity.
Limitation(s)
There are myriads of pathologies that can be found in the lumbar spine, however present study may not have captured all but centered on degenerative changes. Although, the sensitivity and specificity of the MRI in lumbar spine pathologies are well appreciated, there is still the possibility of misinterpretation of findings due to closeness in imaging characteristics.
Conclusion(s)
Lumbar spine pathologies frequently involve the fourth lumbar vertebra and middle-aged males are commonly affected. Lumbar spondylosis is the most common pathology of the lumbar spine and most patients suffered Nurick grade II disability, indicating that they have slight difficulty walking which does not incapacitate them in engaging in full employment.
Pearson’s correlation analysis, significance (p<0.05) and Non-significance (p<0.05)