Talon’s cusp is described as a process of horn-like shape curving from the base downwards to the cutting edge. Ripa and Mellor later described this phenomenon as talon cusp resemblance to talon of eagle. Talon cusp is a well-defined extra addition cusp like structure which extends from half of the Cementoenamel Junction (CEJ) to the incisal edge on the surface of an anterior tooth. The aetiology is unknown for the formation of the talon cusp. A talon cusp is often diagnosed during routine dental examination as an incidental finding and usually does not show any symptoms. In such cases, careful clinical and radiographic examination is mandatory for correct diagnosis and treatment planning. Due to limitation of 2-D (two dimensional) radiographs, these images are unable to recognise the complicated anatomy of the tooth. Use of Cone-Beam Computed Tomography (CBCT) has become common in dentistry. CBCT has been useful in producing a three-dimensional (3-D) image without distortion of the teeth, maxillofacial skeleton and related tissues. Scan of CBCT help to plan treatment and also provide valuable information about dental anatomy. This paper describes a case of 23-year-old female patient with a facial talon cusp on the permanent maxillary left central incisor, which was endodontically managed and followed by aesthetics rehabilitation with a follow-up for a period of one year.
Dental anomaly, Extra cusp, Porcelain veneer
Case Report
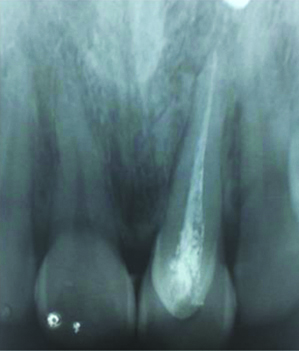
A 23-year-old female patient arrived in the Department of Conservative Dentistry and Endodontics with a complaint of pain in the upper front tooth region of the jaw for one month. Patient also wanted to correct her abnormal appearance of the front tooth. Medical and family histories were non contributory. Dental history revealed Root Canal Treatment (RCT) with temporary restoration done two years back with respect to tooth 21. On intraoral examination, the presence of a horn like protuberance was observed extending from CEJ towards incisal edge (stage 3) along with discoloration on the labial aspect of the permanent maxillary left central incisor. The pain was dull, localised and intermittent in nature. There were no other associated symptoms. Pain on percussion was present with respect to 21. Facial talons cusp has been classified into three stages according to the grades starting from slightest to most extreme form by Mayes AT (2007). In this case stage 3 has been observed which consist of a cusp on the facial aspect extending from the CEJ to the incisal end [Table/Fig-1] [1]. Preoperative radiograph intra oral periapical radiograph reported a radio-opaque structure which was ‘V’ shaped and superimposed on the image of the maxillary left central incisor. With the help of CBCT, extension of pulp tissue radiolucency into the cusp could be determined.
Preoperative picture showing talon cusp in relation to 21.

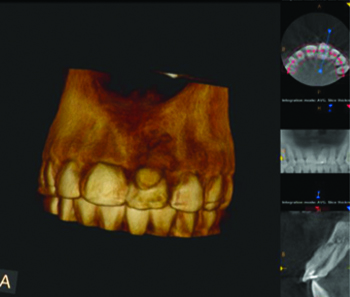
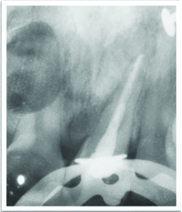
Radiopaque filling was seen in the root canal of the involved tooth [Table/Fig-2]. Pulp involvement cannot be observed in Intra oral Periapical Radiographs (IOPAR) due to overlap of protuberance on tooth crown. Aesthetic of the patient was compromised because of the presence of cusp which was extra and discolored w.r.t 21. Patient was advised CBCT to reveal the involvement of pulp into the accessory cusp. The CBCT scan of the involved teeth was performed at 120 KVp. CBCT illustrated the complicated anatomy of 21 tooth and displayed that the pulp chamber was well defined from the globes [Table/Fig-3,4]. One of the challenges in this case is making the correct diagnosis. Dental anomalies occurring in form of a double tooth, is an extremely rare phenomenon. The term which can be used to represent this case is unclearly mentioned or explained in the literature, there are various terms which are used such as talon cusp, accentuated cingulum, or dens evaginatus (the term usually used when it is present in the posterior teeth) [2]. Diagnosis made was facial talons cusp because of the protuberance seen as “a process of horn-like shape curving from the base downwards to the cutting edge” on the facial surface of the tooth. This phenomenon was given by Ripa and Mellor because of cusp’s compared to talon of an eagle [3]. Treatment plan was made after clinical and radiographic examination which includes non surgical endodontic retreatment followed by placement of veneer.
Preoperative radiograph showing radiopaque filling in relation to 21.
Coronal view of CBCT image showing talon cusp in relation to 21.
Saggital view of CBCT image showing extra pulp canal in 21.

On first appointment, isolation was done using rubber dam. Removal of temporary restoration and refinement of access cavity was done with EX 24 bur (Mani). Gutta percha was removed with the help of H File (Mani). After gutta percha removal, radiograph was taken to confirm complete removal of gutta percha. Canal was renegotiated with no. 10 and 15 k files. Canal was irrigated with 5.25% NaoCl (Prime Dental Products), saline (0.9% W/V) (Amanta Healthcare Ltd.,) and dried using paper points (Dentsply, Maillefer, Switzerland).
Working length was determined i.e., 21 mm with no. 15 K file (Mani) and confirmed using apex locator (Dentaport ZX J Morita). Cleaning and shaping was performed by rotary instruments (Protaper universal files). Final file used was F3 (30/09) Protaper universal file for shaping of the canal.
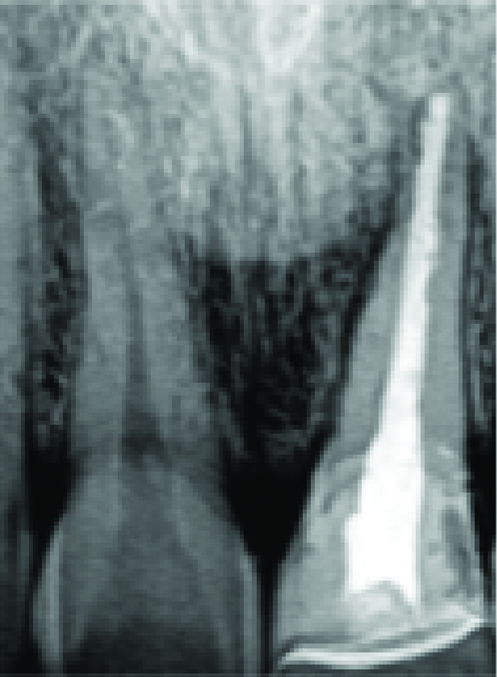
The canal was instrumented and irrigated alternately by using 5.25% sodium hypochlorite solution (NaOCl) and saline. Final irrigation was done using 2% Chlorhexidine (CHX) (Dentochlor, Ammdent). Calcium hydroxide (AvueCal) was placed inside the canal and patient was recalled after one week for evaluation of symptoms and continuation of treatment procedure. Master cone was selected and radiograph was taken to confirm the length. Canal was coated with sealer followed by obturation using cold lateral condensation technique with gutta-percha and AH Plus as the sealer. Coronal restoration was done with composite resin (Filtek Z 250, 3M Dental Products) [Table/Fig-5].
Postoperative radiograph of 21 with radiopaque filling.
Extra cusp like protuberance was reduced with TR-13 (tapered round bur) (Mani) [Table/Fig-6]. Tooth was prepared in single sitting by reducing 0.75 mm enamel with a tapered round fissure bur (TR 13, Mani) creating a light chamfer without internal line angles in cervical and proximal areas. Preparation was extended onto proximal surfaces just labial to or slightly into contact areas). A 0.5 mm deep chamfer finish line was given with the round end tapered diamond held parallel to the lingual surface. Finished facial preparation in 2 planes. Incisal edge was reduced 1.5 mm to provide porcelain coverage [Table/Fig-7]. Impression was taken with the putty (Aquasil, Dentsply) and light body impression material (Express XT light body, 3M ESPE) with single step impression technique.
Reduction of talons cusp with TR-13 bur.
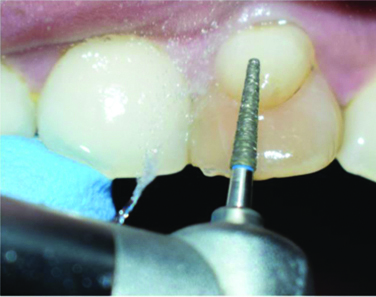
Tooth preparation with respect to 21.

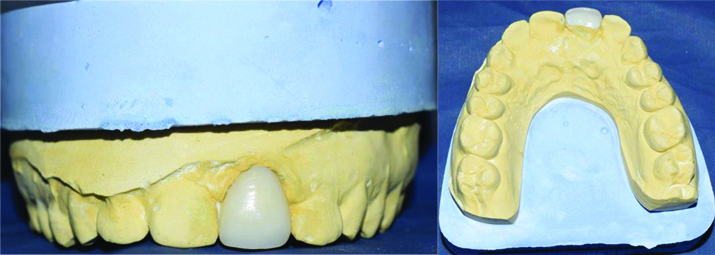
Shade selection was done using Vita Classical Shade Guide (Vident, Brea, CA, USA). Shade tab was kept next to the tooth; A1 shade was selected. Gingival retraction cord 000 (Prime dental, India) was placed into the gingival sulcus for 5-8 minutes to slightly displace the tissue. Veneer was fabricated in relation to 21 and before placing on the tooth, veneer trial was done on cast [Table/Fig-8].
Veneer fabrication with respect to 21.
The intaglio surface was treated for 20 seconds with 9.6% HF acid (Pulpdent, USA) to secure optimal bonding to the adhesives and luting cements. The HF acid was thoroughly cleaned and air dried followed by application of the silane. Monobond S (silane agent) is applied onto the pretreated surface with the help of applicator tip, allowed to react for 60 seconds and then thoroughly dispensed with air.
Etching of enamel was done for 20 seconds using 37% phosphoric acid followed by thorough cleaning with water and gently air dried. Dentin bonding agent (Scotchbond universal adhesive, 3M ESPE) was applied for 20 seconds on the etched surface, before it was dispersed and light-cured. Luting cement Variolink N was then applied to the bonding surface of the restoration afterwards with finger pressure restoration was gently placed followed by application of liquid Strip. Liquid strip helps in preventing the formation of an oxygen inhibition layer. At last, light curing was done for 20 seconds. The assessment of residual cement elimination was done by probing the crevicular sulcus. Dental floss was passed with light friction [Table/Fig-9]. No symptom was observed and the tooth was vital after a follow-up of one year [Table/Fig-10].
Cementation of veneer on 21 with Variolink N luting cement.


Oral prophylaxis was advised to the patient. Patient was advised for crown lengthening for gingival level correction to enhance aesthetic but patient was not ready for the procedure as she had her marriage in one week and was satisfied with the treatment. Patient had reported for a short time period to the department for the above treatment. Treatment was done in three visits within 10 days of time. The follow-up radiograph showed no radiolucency in periapical tissues in the treated tooth of the maxillary left central incissor [Table/Fig-11].
One year follow-up radiograph of 21 without any radiolucency in the periapical tissues.
Discussion
According to Davis and Brook knowledge of the anomaly is essential for an accurate diagnosis of the talon cusp and to avoid unneeded surgical procedures, such as tooth extractions [4]. There were several reported clinical cases including the present report only 75% of facial talon cusps were seen in permanent dentition. A 92% affect the maxillary teeth when compared with mandibular teeth [5]. In this case, patient with a facial talon cusp on a left maxillary permanent central incisor was reported.
Talon cusps occur usually on the lingual or palatal surfaces of the anterior teeth. Talon cusps may be associated with Mohr syndrome, Sturge-Weber syndrome, Rubinstein-Taybi syndrome, incontinentia pigmenti achromians, or Ellis-van Creveld syndrome. A unique variant which has vertical cristae (rugae adamantineae) has been observed on the facial surface of maxillary incisor [6]. Clinical manifestation in relation to any of the above mentioned syndrome was not seen in the patient. A defining feature of Rugae adamantineae is a ridge of enamel that crosses the center of the vestibular surface of the tooth in a cervical-incisal direction, as shown in this paper [7].
The management of talon cusps has various modalities such as no treatment, sequential grinding of the cusp, pit and fissure sealants, restorative treatment, pulp therapy, crown, and extraction of the tooth. In this case, the tooth required aesthetic and functional rehabilitation when diagnosed, which was fulfilled by placement of veneer after RCT of the tooth [8,9].
According to a study, talon cusp was grinded as recommended in cases with premature contact and occlusal interference [5]. After complete cuspal grinding, placement of veneer was done. Veneers are considered to be an alternative to a full crown for enhancing the anterior tooth appearance [Table/Fig-10]. An in vivo study have shown that over a period of 10 years ceramic veneer exceeds estimated survival of 90% [10]. Porcelain veneers are thus considered as conservative and predictable option for full coverage. Indications of veneer must be precise to guarantee satisfactory outcome and longevity. Lithium disilicate was selected because of their less porosity and higher crystalline content compared to other ceramics. Lithium disilicate veneer has flexural strength of approximately 360 MPa- 400 MPa which is sufficient to rehabilitate the anterior guidance. It is more natural looking in aesthetics when compared with other ceramic veneers [11]. Variolink N was used for luting lithium disilicate veneer in this case.
In the present case, talon cusp presented a true talon i.e., extends from the CEJ to the incisal edge. Radiograph is inherently difficult to use for tracing the pulpal configuration inside because the cusp is superimposed on the affected tooth. For this reason, clinician decided to examine the tooth by CBCT [12]. CBCT is an X-ray imaging approach that shows that gives high-resolution 3-D images and has advantage in the identification and localisation of anatomy of tooth [13,14]. In the reported case, CBCT images helped to observe a cusp that showed no communication with the pulp.
Over a period of one year follow-up, this case reported no postoperative complications. The patient did not report pain or any symptoms over a period of one year. No discolouration, shade or translucency difference was observed on the veneer surface.
Conclusion(s)
Clinician should be aware of such anomalies and their outcomes so that proper management of the anomaly can be instituted. Premature diagnosis and treatment are suggested to avoid complications and to maintain a healthy pulpal and periodontal status. CBCT are very helpful in diagnosis but also can serve as predominant aid in treatment planning and in ensuring successful results.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 29, 2020
Manual Googling: Mar 12, 2021
iThenticate Software: Apr 08, 2021 (12%)
[1]. Mayes AT, Labial talon cusp: A case study of pre-European-contact American IndiansJ Am Dent Assoc 2007 138:515-18.10.14219/jada.archive.2007.020517403743 [Google Scholar] [CrossRef] [PubMed]
[2]. Ekambaram M, Yiu CK, King NM, An unusual case of double tooth with facial and lingual talon cuspsOral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 105:e63-67.10.1016/j.tripleo.2007.11.03318329569 [Google Scholar] [CrossRef] [PubMed]
[3]. Sarpangala M, Devasya A, Variants of Talon Cusp (Dens Evaginatus)J Clin Diagn Res 2017 11(1):ZJ01-02.10.7860/JCDR/2017/24042.920728274081 [Google Scholar] [CrossRef] [PubMed]
[4]. Suresh KV, Pramod RC, Yadav SR, Kumar N, Mounesh Kumar CD, Kumar SP, Multiple talon cusps on maxillary central incisor: A case reportJ Dent Res Dent Clin Dent Prospects 2017 11(2):127-30.10.15171/joddd.2017.02328748055 [Google Scholar] [CrossRef] [PubMed]
[5]. Nu Nu Lwin H, Phyo Kyaw P, Wai Yan Myint Thu S, Coexistence of true talon cusp and double dens invaginatus in a single tooth: A rare case report and review of the literatureClin Case Rep 2017 5(12):2017-21.10.1002/ccr3.125229225847 [Google Scholar] [CrossRef] [PubMed]
[6]. Shrestha A, Marla V, Shrestha S, Maharjan IK, Developmental anomalies affecting the morphology of teeth-a reviewRSBO Revista Sul-Brasileira de Odontologia 2015 12(1):68-78.10.21726/rsbo.v12i1.175 [Google Scholar] [CrossRef]
[7]. Shafer 7th edition. A textbook of oral pathology [Google Scholar]
[8]. Myers LC, Treatment of a talon cusp incisor: Report of caseJ Dent Child 1980 47:119-21. [Google Scholar]
[9]. De Sousa SM, Tavano SM, Bramante CM, Unusual case of bilateral talon cusp associated with dens invaginatusInt Endod J 1999 32(6):494-98.10.1046/j.1365-2591.1999.00243.x10709498 [Google Scholar] [CrossRef] [PubMed]
[10]. Peumans M, De Munck J, Fieuws S, Lambrecht P, Vanherle G, Van Meerbeek V, Prospective ten-year clinical trial of porcelain veneersJ Adhes Dent 2004 6(1):65-76. [Google Scholar]
[11]. Burke FJ, Survival rates for porcelain laminate veneers with special reference to the effect of preparation in dentin: A literature reviewJ Esthet Restor Dent 2012 24(4):257-65.10.1111/j.1708-8240.2012.00517.x22863131 [Google Scholar] [CrossRef] [PubMed]
[12]. Shashikiran ND, Babaji P, Reddy VV, Double facial and lingual trace talon cusps: A case reportJ Indian Soc Pedod Prev Dent 2005 23:89-91.10.4103/0970-4388.1644916012212 [Google Scholar] [CrossRef] [PubMed]
[13]. Filho FB, Zaitter S, Haragushiku GA, de Campos EA, Abuabara A, Correr GM, Analysis of the internal anatomy of maxillary first molars by using different methodsJ Endod 2009 35(3):337-42.10.1016/j.joen.2008.11.02219249591 [Google Scholar] [CrossRef] [PubMed]
[14]. Durack C, Patel S, Cone beam computed tomography in endodonticsBraz Dent J 2012 23(3):179-91.10.1590/S0103-6440201200030000122814684 [Google Scholar] [CrossRef] [PubMed]