Systematic Review on Relation Between Surface Treatment and Outcome of Delayed Replantation of Permanent Anterior Avulsed Teeth
Shaili Mehta1, Jayeeta Verma2
1 Former Intern, Department of Conservative Dentistry and Endodontics, MGM Dental College and Hospital, Navi Mumbai, Maharashtra, India.
2 Lecturer, Department of Conservative Dentistry and Endodontics, MGM Dental College and Hospital, Navi Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shaili Mehta, Former Intern, Department of Conservative Dentistry and Endodontics, MGM Dental College and Hospital, Junction of NH4 and, Sion-Panvel Expy, Sector 18, Navi Mumbai-410209, Maharashtra, India.
E-mail: drshailimehta@gmail.com
Introduction
One of the most severe dental injury is Tooth Avulsion or exarticulation. Tooth avulsion is the complete displacement of tooth out of the socket. The common treatment employed for avulsed teeth is replantation, the prognosis of which depends on the handling of the tooth specimen and time lag between avulsion and replantation of the teeth. Surface treatment of root surface of avulsed teeth prior to delayed replantation is a common practice and a variety of agents and methods have been used for the same. The literature lacks evidence that establishes a definitive relation between surface treatment and prognosis of delayed replantation of avulsed teeth.
Aim
To understand the effect of surface treatment and outcome after replantation of avulsed anterior permanent teeth with an extraoral dry time of more than 60 minutes.
Materials and Methods
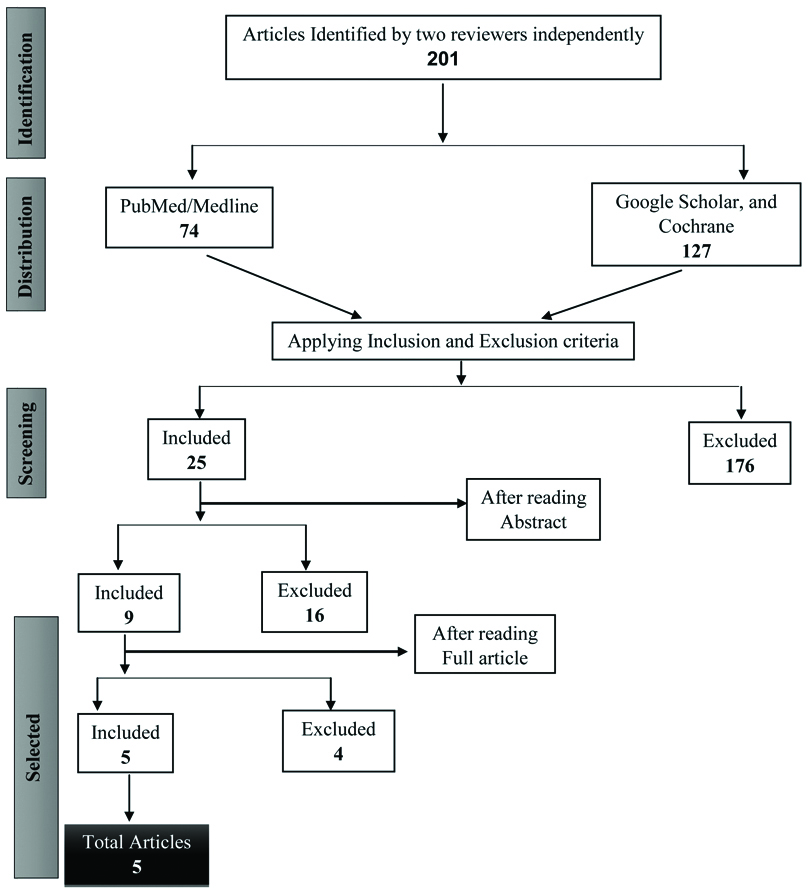
The protocol for systematic review was registered on PROSPERO, registration number was CRD42020222919. A search was performed on case reports and case series available on delayed replantation of avulsed anterior permanent teeth on databases like Medline/PubMed, Google Scholar, and Cochrane from the year 2000 to 2018. The MeSH terms and keywords like tooth avulsion*, tooth fractures*, tooth injuries*, traumatology*, delayed replantation methods and delayed replantation standards with Boolean operators were used for data identification and screening. After applying inclusion and exclusion criteria, total five articles were included.
Results
The duration of storage of the teeth were variable with cases reported from 24 hours to 72 hours of extraoral dry time. All five reports used different methods for surface treatments. No complications were reported after 12 months in three cases. No complication was reported after 24 months in one case. After 12 weeks, one article reported ankylosis and infraocclusion after replantation.
Conclusion
As a result of data heterogenicity and a short follow-up period of the articles, a clear relation between surface treatment and delayed replantation of an avulsed teeth could not be established. However, it can be safely concluded that surface treatment of avulsed teeth prior to delayed replantation results in a better prognosis and predictable outcomes.
Dental trauma, Extraoral dry time, Prognosis, Storage medium, Tooth avulsion
Introduction
Human beings are susceptible to trauma. Trauma to the teeth can vary from fracture involving only enamel to complete displacement of tooth out of the socket which is known as tooth avulsion or exarticulation [1].
The root surface of an avulsed tooth with an extraoral dry time of more than 60 minutes has high chances of contamination from dirt, soil, microbes, etc. This contaminated root surface could lead to infection or complications after replantation. Thus, removing the surface contamination to delay or avoid the complications are the main goals of replantation of avulsed tooth. The above goals can be achieved through surface treatment. The guidelines given by the American Academy of Pediatric Dentistry have evolved from 2007 to 2019 and the idea regarding surface treatment has changed with time [2-4].
Prognosis of an avulsed teeth after replantation depends on the time lag between storage and replantation, storage media, the stage of root completion, method of root canal treatment used i.e whether Root Canal Treatment (RCT) was done before or after replantation, whether RCT was performed immediately or after one week, and surface treatment of the teeth before replantation. As per the guidelines by International Association of Dental Traumatology (IDAT) in 2012, it was suggested that prognosis was considered to be good if the tooth is asymptomatic with normal mobility, and normal percussion sound, no radiographic of resorption or peri radicular osteitis, and the lamina dura was normal [3].
The avulsed tooth loses its Periodic Ligament (PDL) viability after 60 minutes of extraoral time, [2] leading to a theoretically poor prognosis. This leaves the clinician in a dilemma whether to perform replantation of the avulsed tooth. In case the clinician decides to perform delayed replantation uncertainty exists regarding the measures to be followed to have a predictable outcome and good prognosis. Thus, this systematic review was conducted to understand the relationship between surface treatment and outcomes of delayed replantation of avulsed tooth with an extraoral dry time of more than 60 minutes.
Materials and Methods
Protocol and Registration
The PRISMA guidelines 2009 were followed for writing the protocol and the systematic review was registered on PROSPERO. The (PROSPERO registration number: CRD42020222919) [5].
Research Question
The question was- ‘Does surface treatment affect the success of delayed replantation of permanent anterior teeth with extraoral dry time of more than 60 minutes?’
P-(POPULATION)- Avulsed permanent anterior teeth.
I-(INTERVENTION)- Replantation of an avulsed teeth after surface treatment.
C-(COMPARISON)- Various techniques and agents used for surface treatment.
O-(OUTCOME)- Complications such as ankylosis, resorption, and infraocclusion
Search Strategy
A search was performed on delayed replantation of avulsed anterior permanent teeth on electronic databases Medline/PubMed, Google Scholar, and Cochrane from the year 2000 to 2018. Manual searches were also performed on the articles retrieved during the electronic search. The MESH terms and keywords like tooth avulsion*, tooth fractures*, tooth injuries*, traumatology*, delayed replantation methods and delayed replantation standards with Boolean operators were used for data identification and screening. Two reviewers independently evaluated every article and in cases of divergence, the decision whether to select the case report, was reached through discussion.
[Table/Fig-1] shows the PRISMA flow diagram for the total number of articles selected for the systematic review.
Inclusion criteria
Case reports and case series on delayed replantation of avulsed teeth.
Replantation of permanent anterior teeth with closed apex.
Case reports and series in which extraoral dry time exceeds 60 minutes.
Case reports and series with extraoral root canal treatment performed on avulsed teeth before replantation.
Only published case reports and case series were considered.
Exclusion criteria
Case reports and case series on primary teeth and posterior teeth.
Cases with associated fracture.
Cases of teeth stored in storage media before replanting.
Articles in other languages other than English.
Risk of Bias Assessment
For evaluating the risk of bias for case reports, no standard quality assessment tools are available. Case report belongs to descriptive studies because they report occurrences of a disease or a unique finding [6]. For judging the quality of case reports for systematic review there is only one tool, the JBI critical appraisal [7]. Two reviewers independently scored the selected papers for these criteria. The criteria shown in [Table/Fig-2] were used to attain the risk of bias [8-12].
| Study | Were patient’s demographic characteristics clearly described? | Was the patient’s history clearly described and presented as a timeline? | Was the current clinical condition of the patient on presentation clearly described? | Were diagnostic tests or assessment methods and the results clearly described? | Was the intervention(s) or treatment procedure(s) clearly described? | Were adverse events (harms) or unanticipated events identified and described? | Does the case report provide takeaway lessons? | Overall appraisal |
|---|
| Harris A et al., [8] | Yes | Yes | Yes | No | Unclear | Yes | Yes | Included |
| Anand S et al., [9] | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Included |
| Agarwal V et al., [10] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Included |
| Rahbar M and Hassani-Dehkharghani A, [11] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Included |
| Daga A et al., [12] | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Included |
Results
All the results of this systematic review are mentioned in [Table/Fig-3].
Results of Systematic Review.
| Author (Year) | Extraoral dry time | Surface treatment | Outcome |
|---|
| Harris A et al., [8] (2014) | 36 hours | Cleaning of the tooth surface was carried out by storing in 2.5% NaOCl for 20 min and later conditioned with citric acid for 5 min. Prior to reimplantation, the root surface was immersed in 2% acidulated phosphate fluoride gel for 5 min. | No Complication till 24 months |
| Anand S et al., [9] (2014) | 24 hours | The scaling and root planning were performed and the conditioning of the root was done with 10% phosphoric acid. The root was thoroughly washed for 10 seconds to remove the dead periodontal tissue. Then it was immersed in APF gel for 20 minutes followed by metronidazole solution again for 20 minutes. | After 12 weeks, the tooth developed mild infraocclusion (of about 1 mm) and progressive ankylosis but it remained functional and was esthetically acceptable. |
| Agarwal V et al., [10] (2016) | 30 hours | The avulsed tooth was debrided with saline irrigation to remove necrotic periodontal tissues and any other surface contaminants and was placed in a 2.4% acidulated sodium fluoride solution. | No Complication till 12 months |
| Rahbar M and Hassani-Dehkharghani A, [11] (2016) | 30 hours | The avulsed tooth was soaked in the hydrofluoric acid gel (Ultradent®) for 5 min to eliminate necrotic and dried PDL and then in doxycycline solution (doxycycline dissolved in water in a ratio of one to one) for 5 min. | No Complication till 12 months |
| Daga A et al., [12] (2018) | 72 hours | The root of the tooth was cleaned carefully with saline to remove any remnants of necrotic and dried periodontal tissue, and then kept in 2% sodium fluoride solution followed by placement in doxycycline antibiotic solution | No Complication till 12 months |
Discussion
According to our knowledge, this is the first systematic review on the relation between surface treatment and the outcome of replantation of avulsed teeth. In this systematic review, the extraoral dry time of the five cases varied from 24 hours to 72 hours as mentioned in [Table/Fig-3]. The prognosis is best for teeth replanted within five minutes after avulsion, thereafter the PDL is compromised if the delay is between five minutes to 60 minutes and the PDL becomes non viable when the total extraoral dry time is more than 60 minutes [2].
Avulsed tooth usually after trauma, fall on the ground and a tooth that has been out of the socket for more than 60 minutes, is likely to get contaminated with soil, dirt, microorganisms and handling by the operator, thus making cleaning, disinfecting and surface treatment of utmost importance. The rationale of surface treatment is to remove non viable PDL fibres, which might act as a source of infection and could result in inflammatory resorption. The non viable periodontal tissue could also trigger the undifferentiated mesenchymal cells of the socket and differentiate into osteoblast and lead to replacement resorption i.e., ankylosis. Thus, surface treatment of avulsed tooth plays a pivoted role in successful delayed replantation [1,13,14].
Andreasen JO and Andreasen FM recommended that the avulsed tooth should be soaked in 2.4% Acidulated Phosphate Fluoride (APF) solution for 20 minutes before attempting replantation [1]. As per the International Association of Dental Traumatology (IADT) 2007, protocol for replantation of an avulsed teeth after an extraoral dry time of over 60 minutes included immersing the tooth in a 2% sodium fluoride [NaF] solution for 20 minutes [2]. In IADT 2012 guidelines [3] and the recommended guidelines of the American Association of Endodontists for the treatment of Traumatic Dental Injuries 2013 [15], it was stated that surface treatment should be done with 2% NaF solution for 20 minutes but this procedure was just suggested and was not an absolute recommendation.
Fluoride was recommended for surface treatment as it hardens the tooth structure by converting hydroxyapatite into fluorapatite and helps to prevent or delay resorption. The use of 2% acidulated sodium phosphate fluoride has shown a fall in the incidence of inflammatory resorption and an increase in replacement resorption [16]. It has been demonstrated that treatment with alkaline substances, followed by acidic solutions of fluoride provides better results [17]. Various other agents such as dexamethasone, triple antibiotic paste, sodium fluoride, stannous fluoride, tetracycline, minocycline, enamel matrix derivatives fibroblast growth factor (bFGF or FGF-2), etc. have been recommended for surface treatment [18-23].
In this systematic review, all five articles [8-12] used fluoride products for surface treatment. Harris A et al., [8] soaked avulsed teeth in 2% acidulated fluoride solution for five minutes and Aggrawal V et al., [10] soaked avulsed teeth in 2.4% acidulated sodium fluoride solution (pH 5.5) for 20 minutes as per Andreasen’s recommendation [1]. Daga A et al., [12] soaked avulsed tooth in 2% acidulated sodium fluoride solution and later placed in doxycycline antibiotic. According to the authors, this was done because a decrease in the frequency of ankylosis and inflammatory root resorption has been reported after topical application of doxycycline [21]. Rahbar M and Hassani-Dehkharghani A [11] soaked avulsed tooth in the hydrofluoric acid and then in doxycycline solution for five minutes with no explanation or rationale mentioned in the article. Anand S et al., [9] used 2.4% acidulated sodium fluoride solution (pH 5.5) for 20 minutes and then immersed in the metronidazole solution for another 20 minutes. This was done with a rationale to minimise the bacterial load and prevent resorption.
The distribution of success varies largely in this systematic review. Out of five case reports, one case report did not describe any pathological change at the end of 24 months [8]. Three cases reports no complication after 12 months [10-12] and one article report mentioned ankylosis and infraocclusion (1 mm) after 12 weeks of replantation [9]. The development of inflammatory root resorption is related to damage of the periodontium at the time of trauma, the presence of bacteria within the root canal, the extent to which the viability of the periodontal ligament cells remaining on the root surface is maintained [22]. In adults, replacement resorption is usually seen within 1-3 years and in children, it is seen after 1-5 years. Inflammatory resorption and replacement resorption processes take time and usually are unpredictable, therefore long-term follow-up should be considered. Thus, any case of replantation should have a minimum follow-up of five years for the complication of replacement resorption to occur [23]. From this systematic review, we could conclude that the follow-up period of most of the case studies was not adequate for the complications to be evaluated properly.
Limitation(s)
This systematic review was based on case reports i.e. a form of observational study rather than randomised control trials. This systematic review merely analysed the different surface treatment methods used by the clinicians for delayed replantation of avulsed teeth and its effect on the prognosis of replanted teeth. Randomised controlled trials with a long follow-up period need to be carried out to establish a concrete relation between surface treatment and prognosis of delayed replantation of avulsed teeth.
Conclusion(s)
In this systematic review, there was a lot of variation in the methodology performed, agents, and concentrations of the agents used for surface treatment by the clinician for replantation of teeth. Due to data heterogenicity, a clear idea regarding technique, agents, and concentration of agents for surface treatment could not be established. As a result of short follow-up period in all the articles, the relationship between surface treatment and success of replantation could not be concluded. However, it can be safely concluded that surface treatment of avulsed teeth prior to delayed replantation shows better results and predictable outcomes.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? No
For any images presented appropriate consent has been obtained from the subjects. No
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 01, 2021
Manual Googling: Apr 29, 2021
iThenticate Software: May 27, 2021 (21%)
[1]. Andreasen JO, Andreasen FM, Avulsions. In: Andreasen JO, Andreasen FM, (Editors)Textbook and Colour Atlas of Traumatic Injuries to the Teeth 1994 CopenhagenBlackwell Munksgaard:383-25. [Google Scholar]
[2]. Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F, Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teethDent Traumatol 2007 23(3):130-36.10.1111/j.1600-9657.2007.00605.x17511833 [Google Scholar] [CrossRef] [PubMed]
[3]. Andersson L, Andreasen JO, Day P, Guidelines for the Management of Traumatic Dental Injuries: 2. Avulsion of Permanent TeethDent Traumatol 2012 28:88-96.10.1111/j.1600-9657.2012.01125.x [Google Scholar] [CrossRef]
[4]. Fouad AF, Abbott PV, Tsilingaridis G, Cohenca N, Lauridsen E, Bourguignon C, International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teethDent Traumatol 2020 36(4):331-42.10.1111/edt.1257332460393 [Google Scholar] [CrossRef] [PubMed]
[5]. https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=222919 [Google Scholar]
[6]. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D, The CARE guidelines: Consensus-based clinical case report guideline developmentJ Clin Epidemiol 2014 67(1):46-51.10.1016/j.jclinepi.2013.08.00324035173 [Google Scholar] [CrossRef] [PubMed]
[7]. https://jbi.global/critical-appraisal-tools [Google Scholar]
[8]. Harris A, Reshmi J, George S, Issac JS, Delayed reimplantation: A case reportJ Int Oral Health 2014 6(5):104-07. [Google Scholar]
[9]. Anand S, Masih U, Yeluri R, Re-implantation of an avulsed maxillary incisor after prolonged dry storage in a fourteen year old adolescent: A Case Report 2014 1(1):01-05. [Google Scholar]
[10]. Agrawal V, Agrawal A, Srikumar GPV, Sharma V, Hans MK, Success of Delayed Replantation of an Avulsed Tooth: A Case ReportJ Int Oral Health 2016 8(11):1039-42. [Google Scholar]
[11]. Rahbar M, Hassani-Dehkharghani A, Replantation of an Avulsed Tooth 30 Hours after Traumatic InjuryJ Int Oral Health 2016 8(8):879-82. [Google Scholar]
[12]. Daga A, Gaddalay S, Pathan M, Badgire S, Delayed Replantation of Avulsed Tooth After 3 Days Extra-Oral Time and 1-Year Follow-UpInternational journal of scientific research 2016 5(9):641-43. [Google Scholar]
[13]. Trope M, Yesiloy C, Koren L, Moshonov J, Friedman S, Effect of different endodontic treatment protocols on periodontal repair and root resorption of replanted dog teethJEndod 1992 18:492-96.10.1016/S0099-2399(06)81349-X [Google Scholar] [CrossRef]
[14]. Finucane D, Kinirons M, External inflammatory and replacement resorption of luxated and avulsed replanted permanent incisors: Are view and case presentationDent Traumatology 2003 19(3):170-74.10.1034/j.1600-9657.2003.00154.x12752540 [Google Scholar] [CrossRef] [PubMed]
[15]. The Recommended Guidelines of the American Association of Endodontists for The Treatment of Traumatic Dental Injuries- https://www.aae.org/specialty/wp-content/uploads/sites/2/2019/02/19_TraumaGuidelines.pdf [Google Scholar]
[16]. Panzarini SR, Gulinelli JL, Poi WR, Sonoda CK, Pedrini D, Brandini DA, Treatment of root surface in delayed tooth replantation: A review of literatureDent Traumatol 2008 24(3):277-82.10.1111/j.1600-9657.2008.00555.x18410388 [Google Scholar] [CrossRef] [PubMed]
[17]. Bjorvatn K, Massler M, Effect of fluorides on root resorption in replanted rat molarsActa Odontol Scand 1971 29(1):17-29.10.3109/000163571090263195280613 [Google Scholar] [CrossRef] [PubMed]
[18]. Ravi KS, Pinky C, Kumar S, Vanka A, Delayed replantation of an avulsed maxillary premolar with open apex: A 24 months follow-up case reportJ Indian Soc Pedod Prev Dent 2013 31:201-24.10.4103/0970-4388.11797124021335 [Google Scholar] [CrossRef] [PubMed]
[19]. Kum KY, Kwon OT, Spängberg LS, Kim CK, Kim J, Cho MI, Effect of dexamethasone on root resorption after delayed replantation of rat toothJ Endod 2003 29:810-13.10.1097/00004770-200312000-0000614686811 [Google Scholar] [CrossRef] [PubMed]
[20]. Selvig KA, Bjorvatn K, Claffey N, Effect of stannous fluoride and tetracycline on repair after delayed replantation of rootplaned teeth in dogsActa Odontol Scand 1990 48:107-12.10.3109/000163590090058652188476 [Google Scholar] [CrossRef] [PubMed]
[21]. Cvek M, Cleaton-Jones P, Austin J, Lownie J, Kling M, Fatti P, Effect of topical application of doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisorsEndod Dent Traumatol 1990 6:170-76.10.1111/j.1600-9657.1990.tb00413.x1723382 [Google Scholar] [CrossRef] [PubMed]
[22]. Tuna EB, Yaman D, Yamamato S, What is the Best Root Surface Treatment for Avulsed Teeth?Open Dent J 2014 8:175-79.10.2174/187421060140801017525317212 [Google Scholar] [CrossRef] [PubMed]
[23]. Iqbal MK, Bamaas N, Effect of enamel matrix derivative (EMDOGAIN) upon periodontal healing after replantation of permanent incisors in beagle dogsDent Traumatol 2001 17(1):36-45.10.1034/j.1600-9657.2001.170107.x11475769 [Google Scholar] [CrossRef] [PubMed]