Badminton is the most played sports in the world. It is a sport played using racquets to hit a shuttlecock across a net and played by two or four players on a rectangular court with a high net across the middle. It is played by all the ages of people. This game needs a combination of jumps, lunges, agility and rapid arm movements. While performing these movements the body may exhibit many musculoskeletal injuries during the game [1]. Hence, it is common for the badminton players to sustain various injuries during playing. Flexibility is an essential component of injury prevention and rehabilitation [2].
In the life of a normal human function or in doing activity of daily living muscular flexibility plays an important role. Flexibility is the ability of a joint or series of joints to move through an unrestricted, pain free range of motion. A limitation in the muscular flexibility leads to several musculoskeletal overuse injuries in players life and remarkably affect a person’s level of function [3,4]. Muscular tightness is frequently postulated as an intrinsic risk factor for the development of a muscle injury. When muscles are allowed sufficient time to accelerate and decelerate limb segments, connective tissues are spared and are therefore less prone to rupture. Thus, enhanced flexibility is associated with improved movement economy and reduced risk of injury [5]. People encounter various kinds of muscle tightness and always keep trying different modes of treatment for therapy.
A vertical jump is the act of jumping upwards into the air. It is an effective exercise for building both endurance and explosive power. The goal of vertical jump is reaching as high as possible, from the ground. A squat jump or countermovement jump is typically performed in the vertical jump from one or both the legs. The vertical jump is also commonly used as a test to estimate lower-body power as strength and conditioning exercise [6,7].
The MFR is a “curative” tool for treatment of the tightness. It is a manual therapy technique that uses applied pressure and stretching to muscles and fascia with the intent to improve movement of the muscles and the surrounding fascia [8,9]. The MFR is one of many techniques used to increase mobility in a joint or series of joints and also improve athletic performance [10]. It is using body weight or force onto an object such as a foam roller or lacrosse ball to place pressure along a muscle with the intent to target the adhesions in fascia to improve movement [11]. Performing MFR may be done through massages or through tools, usually done by a therapist, but more commonly, Self-MFR (SMR) is performed by individuals themselves. The MFR has recently become a common injury prevention strategy used in preactivity warm-up period to assist in improving muscle relaxation and tissue pliability through decreasing contractile activity and motor neuron excitability [12].
Materials and Methods
This was an intervantional study design with 60 subjects recruited with sample of convenience. The study was carried out from July 2018 to May 2019. Voluntary participation was obtained from each subject by getting the consent form signed and the ethical approval (letter no: 10/715/registrar/office/DPSRU/2018/9947) was taken from the Institutional Ethical Review Committee. The sample size was calculated with 95% confidence interval and 5% precision.
Inclusion criteria: Recreational badminton player with age group range between 20-30 years who played at least once in a month (1-2 hours per month) for last one year, were recruited.
Exclusion criteria: Subjects with any recent injury, neuromuscular disorder, recent trauma to the lower limb, any type of breathing problem and with any psychological dysfunctions were excluded from the study.
All the subjects were systematically assigned into three groups viz., Group-A with Quadriceps Muscle, Group- B with Hamstring Muscle and group-C with Calf muscle with 20 subjects in each group. Vertical jump height, Knee flexion angle (Quadriceps flexibility) were measured after modified Thomas test, PA (Hamstrings flexibility) measured by 90-90 straight leg raising test and distance from the wall (Calf flexibility) measured by Lunge test was measured before and after application of MFR.
Measurement of Vertical Jump Height
The Vertical jump test (Sargent jump) was used to measure vertical jump height, which basically involves measuring the difference between a person’s standing reach and the height to which he or she can jump and touch [18]. The basic Sargent jump has the subject stand facing a smooth, dark wall with both feet flat on the floor and toes touching the wall. He or she then reaches as high as possible and makes a mark on the wall (or wall-mounted jump board/chalkboard) with either hand with a piece of chalk or chalk dust. Holding the desired jump position with the preferred side to the wall, the subject jumps as high as possible and makes another mark at the peak of the jump. The vertical jump score is the difference between the two marks (recorded in inches or centimeters) [Table/Fig-1].
Vertical Jump height measurement.

Measurement of Hamstring Tightness
A 90-90 straight leg raising test was used to measure hamstring flexibility. The subject was requested to lie down supine on the plinth and the pelvis was strapped to the plinth for stabilisation. A half circle universal goniometer has been used to measure the PA of knee Range of Motion (ROM). The fulcrum of the goniometer was cantered over the lateral condyle of femur. The movable arm was assigned with alignment to the lateral malleolus as a reference and stationary arm on the femur using the greater trochanter as a reference. Therapist passively extended the tested knee as far as possible. The goniometer measured the angle of knee extension in degrees giving an indication of hamstring muscle length [19]. For normal flexibility in the hamstrings, knee extensor should be within 20° of full extension [Table/Fig-2].
Hamstring tightness measurement.
Measurement of Rectus Femoris Tightness
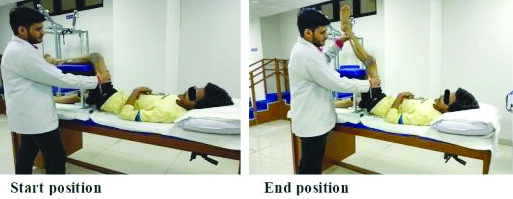
The Modified Thomas test was used to assess hip flexibility, specifically of the iliopsoas and quadriceps muscles. The participant was asked to lie in a supine position with the knees bent over the edge of the examination table. After that they were instructed to flex one knee upto the chest and hold it. At the same time, the angle of the test knee (opposite of the knee held to the chest) was to remain at 90 degree, and the hip and posterior thigh of the test leg were to remain in a stationary position and flat against the examination table. The assessment was scored as a fail if the test knee extended and moved to a position of less than 90 degree [Table/Fig-3] [20].
Rectus Femoris tightness measurement.

Measurement of Calf Tightness
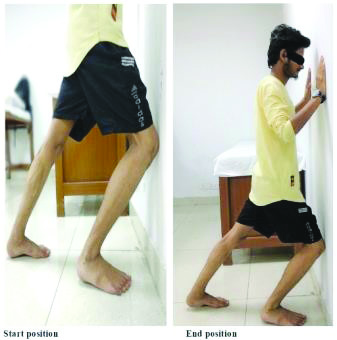
Lunge Test of ankle Doris flexion (DF)-ROM was used to measure calf flexibility. Participants were instructed to stand facing the wall with their great toe 6 inches from the wall on a tape measure affixed to the floor [Table/Fig-4]. From this position, the participants were asked to flex their hip and knee while dorsiflexing the ankle to lunge forward in an attempt to touch the anterior aspect of the knee to the wall while keeping the sole of the foot in full contact with the ground. If participants reached the wall with knee, they moved their great toe backward from the wall until they were as far from the wall as possible while maintaining full foot contact with the ground, with the anterior portion of the knee maintaining contact with the wall [21]. Using the tape measure on the floor, this distance was recorded in millimeters to indicate a single value of DF-ROM [22].
Measurement of calf tightness.
Application of Myofascial Release Technique
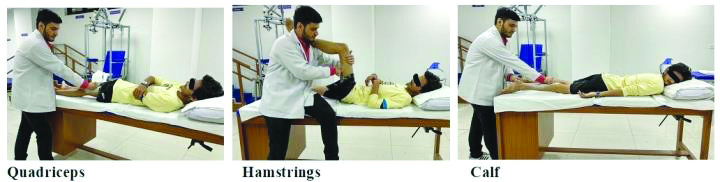
All the subjects were requested to lie in appropriate position on the plinth for specific muscle. The subject was placed in a supine position with the knees bent over the edge of the examination table for quadriceps, supine on the plinth and the pelvis was strapped to the plinth for stabilisation for hamstrings and prone for calf [Table/Fig-5]. While the subject was lying in the appropriate position, with hands placed on the surface of the body with the knuckles and descend into the soft tissue to contact the first barrier and engage the fascia by taking up the slack in the tissues finally move the fascia across the surface while staying in touch with the underlying layers. The subject then maintained pressure to stretch the barrier of the tissue and waited for approximately 3-5 minutes. As the barrier was released, the hand felt the motion and softening of the tissues [13]. The post-test outcome measure was done immediately after the MFR.
Statistical Analysis
All the statistical analysis was done with the help of Statistical Package for the Social Sciences (SPSS) software version 11.5. paired sample t-test was used to find the immediate effect within group. Analysis of Variance (ANOVA) was done to find out the between group. Level of significance was set at 5%.
Results
For this study, 60 participants were selected, from which 20 people were included in quadriceps, 20 in hamstring group and rest 20 in calf group. The MFR was administered to the appropriate muscles. Demographic data shows mean age for quadriceps (20.8±1.17 years), mean age for hamstring (21.25±1.60 years) and mean age for calf (20.7±1.14 years) [Table/Fig-6].
| Groups | Age (mean±SD) years | Male | Female |
|---|
| Quadriceps | 20.8±1.17 | 16 | 4 |
| Hamstring | 21.25±1.60 | 15 | 5 |
| Calf | 20.7±1.14 | 13 | 7 |
Paired t-test was applied for within group comparison of Group A, Group B and Group C for both legs. Result showed statistically significant improvement in vertical jump of quadriceps muscle (p=0.029), and the flexibility of both the legs (p=0.0001) [Table/Fig-7].
Paired sample t-test within quadriceps group.
| Quadriceps (Group A)/mean±SD | Pre | Post | t-value | p-value |
|---|
| Vertical jump height (cm) | 32.65±9.93 | 34.18±10.37 | 2.362 | 0.029 |
| Knee flexion angle left (°) | 26.00±8.82 | 20.00±6.68 | 5.339 | <0.001 |
| Knee flexion angle right (°) | 24.50±7.93 | 18.70±6.26 | 4.833 | <0.001 |
Paired sample t-test within hamstring group was done to find out difference of vertical jump height between pre and post MFR and the results showed significant differences in vertical jump height (p<0.001), PA for flexibility of both left side (p<0.001) and right-side (p<0.001) [Table/Fig-8].
Paired sample t-test within hamstring group.
| Hamstring (Group B)/mean±SD | Pre | Post | t-value | p-value |
|---|
| Vertical jump height (cm) | 35.93±7.71 | 39.01±7.14 | 4.691 | <0.001 |
| Popliteal angle left (°) | 20.75±10.16 | 11.80±9.60 | 7.734 | <0.001 |
| Popliteal angle right (°) | 21.90±10.76 | 13.35±8.45 | 7.140 | <0.001 |
Paired sample t-test within calf group was done to find out difference of vertical jump height between pre and post MFR and the results showed nonsignificant differences (p=0.455) for vertical jump but distance for flexibility of left-side (p<0.001) and right side (p<0.001) showed significant differences [Table/Fig-9].
Paired sample t-test within calf group.
| Calf (Group C)/mean±SD | Pre | Post | t-value | p-value |
|---|
| Vertical jump height (cm) | 28.07±9.56 | 27.55±8.18 | 0.763 | 0.455 |
| Distance (cm) from the wall left | 9.87±1.89 | 11.34±1.29 | 5.252 | <0.001 |
| Distance (cm) from the wall right | 10.07±1.95 | 11.48±1.90 | 4.228 | <0.001 |
The ANOVA between the quadriceps, hamstring and calf groups was done to find out difference of Vertical jump height. Myofasical release showed significant differences in vertical jump height (p=0.0001). flexibility (p=0.0001) [Table/Fig-10].
ANOVA between the groups.
| Variables | mean±SD | t-value | p-value |
|---|
| Quadriceps group | Hamstring group | Calf group |
|---|
| Vertical jump height (cm) | Pre | 32.65±9.93 | 35.93±7.71 | 28.07±9.56 | 3.746 | 0.030 |
| Post | 34.18±10.37 | 39.01±7.14 | 27.55±8.18 | 8.797 | <0.001 |
| Flexibility left | Pre | 26.00±8.82 | 20.75±10.16 | 9.87±1.89 | 21.971 | <0.001 |
| Post | 20.00±6.68 | 11.80±9.60 | 11.34±1.29 | 10.273 | <0.001 |
| Flexibility right | Pre | 24.50±7.93 | 21.90±10.76 | 10.07±1.95 | 19.438 | <0.001 |
| Post | 18.70±6.26 | 13.35±8.45 | 11.48±1.90 | 7.361 | <0.001 |
Discussion
The present study was designed in order to investigate the immediate effects of MFR technique on muscle flexibility, vertical jump height in recreational badminton players. The results of the present study showed statistically significant differences between the three groups of post intervention vertical jump height after the application of MFR.
This study is similar to the study by Barlow A et al., in which the rectus femoris, hamstring, and the gastrocnemius muscle are found to be active during the early take off phase while jumping the proximal gluteus maximus concentrically contract [14], resulting not only in the hip extension but also knee extension due to the pull of stiff cable (Rectus femoris) acting on femur distally, thus transferring the mechanical energy generated by Gluteus maximus to Quadriceps through Rectus femoris [15]. In addition to this report, it is revealed that the functional capacity of two joint muscles depends on the stronger contraction proximal muscle (gluteus maximus). The stronger the proximal muscle contracts, the maximal mechanical energy is redistributed to the distal two joint muscles to generate explosive leg extension during vertical jump [16]. Each muscle tendon complexes was represented by a Hill-type muscle model, comprised of a Contractile Element (CE), Series-Elastic Element (SE) and Parallel-Elastic Element (PE) [17]. Forces of series elastic element and parallel elastic element scaled quadratically with elongation, while CE force depended on fibre length of the muscle, the time-derivative of fibre length, and active state of the muscle [23]. Maximum muscle fibre contraction velocity is proportional to the optimum length of muscle fibre. Active state has first order dynamics defined by the neural stimulation to the muscle, which during jumping varies according to a single onset time per muscle [24]. The effects of changes to the cross-sectional area and muscle fiber optimum length of each muscle results into maximum vertical jump height [25]. These could have been the possible reasons for the observed improvements in the flexibility of quadriceps, hamstring and calf muscle groups intervened with MFR in the present study.
The vertical jump height increment due to MFR on quadriceps muscle is because of the maximally active knee extensors during landing and take-off phase of jump [26]. The active knee extensors absorb the energy which is generated by the ground reaction forces, will increase in the myoelectric activity as an piezoelectricity in the vertical jump which is supported by Hadzic V et al., 2010 [27]. Another study by Baker LB 2015 [28] supports the present study that the Golgi Tendon Organs (GTO) are mechanoreceptors located at muscle-tendon junction, which is a proprioceptive sensory receptor organ that senses the changes in muscle tension. When muscle contract at high tensions, the GTO is stimulated and it relaxes the muscles, due to this autogenic inhibition occurs, that can also lead to an increase in range of motion [29]. These factors might have played a potential role in enhancing the vertical jump height on the different muscle groups intervened with MFR in the present study.
The vertical jump height increment due to MFR on hamstring muscle is because the effects of MFR technique through which muscle tension relationship improves and ultimately provides greater torque leading to improvement in the vertical jump height [30,31].
The results of the present study showed that there was statistically significant difference of MFR on flexibility post (left and right side the study is supported by Schleip R et al., that the fibroblasts are supposedly stimulated through an electric charge when pressure is applied to the tissue, which is generally termed as Piezoelectricity [12]. Piezoelectricity is the electric charge that accumulates in certain solid materials (such as crystals, certain ceramics, and biological matter such as DNA) in response to applied mechanical stress [32,33]. The myoglobin is a fluid protein present in the muscle which is thick, or viscous in nature and under static conditions will flow over time when shaken, agitated, sheared or otherwise stressed [34]. Thixotropic effect is another recurring effect that supposedly explains the process in which the connective tissue responds in a fluid-like manner [35].
Thixotropic is a time-dependent shear thinning property which helps in increasing the range of motion after MFR [29,35]. Another effect seen after MFR is because of responses in the autonomic nervous system where it reduces the levels of cortisol concentration which will helps in reduction of physical stress. The stimulation of the fascia and in turn the mechanoreceptors could also be responsible for triggering the autonomic nervous system to contract the fascia through smooth muscle cells [36]. These contractions explain the relaxation effects of MFR and increases the blood flow and changes in the viscosity as a result it will reduce delayed onset of muscle soreness and increase the range of motion [12]. All these effects could have led to the relaxation of different muscle groups intervened with MFR and thus enhancing the range of motions in the present study.
Limitation(s)
Sample size was small as the duration of the study was fixed and limited by institution, and variations in body mass index, including height and weight.
Conclusion(s)
It can be concluded from the present study that there is immediate effect of MFR on increasing the muscle flexibility during vertical jump. The quadriceps and hamstring flexibility also increases during the vertical jump after the administration of MFR.