Renal and ureteral stones are the third most commonly encountered pathologies in urological practice after urinary tract infection and disease of prostate. Once widely recommended, ESWL, has lost its place as an important therapeutic modality despite its proven efficacy [1,2]. Endourological procedures such as Percutaneous Nephrolithotomy (PCNL) and Ureteroscopy (URS) are now the preferred modes of treatment. However, ESWL still remains a recommended treatment option for solitary renal stones of <2 cm in size [1,2].
A novel and simple nomogram, Triple-D scoring system was proposed by Tran TY et al., which constituted of three CT based metrics: stone dimension (volume), stone density (HU) and SSD [11]. Its efficacy has been validated in many retrospective studies [12,13]. Another scoring system proposed by Ichiyanagi O et al., Quadruple-D scoring system is an extension of Triple-D scoring system in which one score extra is given for stone in non lower polar region. This study showed the better prediction of SFR after ESWL but suggested further study to reinforce the findings [14]. Furthermore, no studies were conducted on Indian population. European Association of Urology (EAU) has recommended ESWL as first line therapy for all renal stones less than 1 cm, with URS as an alternative for selected cases and PCNL reserved for failure of former procedures [1,4].
This study was conducted to evaluate the clinical efficiency of the Quadruple-D scoring system in routine urological practice in Indian population especially for stones 1-2 cm in dimension after giving ESWL.
Materials and Methods
It was a prospective longitudinal study conducted on 120 patients, from April 2019 to July 2020. All these patients presented to the Outpatient Department (OPD) of a tertiary urology care centre in Kolkata, West Bengal, India.
Systemic random sampling technique was applied to select study subjects for study population with a sampling interval of two. The study was conducted as per the guidelines laid down by the declaration of Helsinki. The study protocol was approved by the Institutional Ethical Committee (RKC/577 dated 06.05.2019).
Inclusion criteria: The study subjects more than 18 years of age, patients with a negative report of urine culture, patients receiving ESWL for the first time for the targeted stone, patients with no anatomical urinary tract abnormalities were included.
Exclusion criteria: Patients with distal urinary tract obstruction, unavailable CT images before ESWL, pregnancy, staghorn stones, calyceal diverticular stones, coagulopathy, active urinary tract infection and endourological procedure prior to ESWL were excluded.
Sample size calculation: The sample size was calculated using the formula for descriptive study.
Where:
N-Sample Size, Z1-α/2(1.96)-Standard Normal deviation considering 95% Confidence level.
P-Expected Proportion of SFR as found in the study [15]. It is taken as 96.1%.
Q-(100-P)=3.9.
L-Precision in absolute term (3.5)
Using the above formula, the required sample size was 117. This study chose 120 study subjects.
They were divided into two groups.
Group A: Had stone free status three weeks after ESWL.
Group B: Had residual stone three weeks after ESWL.
Renal stones were evaluated before ESWL with plain abdominal radiography of Kidney, Ureter and Bladder (KUB) as well as helical Non Contrast CT scan (NCCT). The coagulation profile and urine culture sensitivity was also evaluated. Ellipsoid SV was measured using the formula SV=π/6×(anteroposterior×transverse×cranio-caudal diameters) in millimetres [11-13]. Stone density was measured in HU from NCCT and SSD was calculated as the average distance from the body surface to a targeted stone at zero degree, 45° and 90° on NCCT [8].
Quadruple-D score was calculated as the sum of the number of components matching the cut-offs of <150 mm3 for SV, <600 HU for stone density, <12 cm for SSD and location of calculi in the kidney. The location was allocated zero and one point depending whether the stone was placed at the lower calyces or other sites, respectively [14]. The scores ranged from zero (worst) to four (best) points [Table/Fig-1].
Quadruple-D scoring system (Maximum score: 4, Minimum score-0).
| Parameters | Score 1 | Cut-off value | Score 0 |
|---|
| Dimensions (mm3) | <150 | 150 | ≥150 |
| Density (HU) | <600 | 600 | ≥600 |
| Skin-stone distance (cm) | <12 | 12 | ≥12 |
| Lower pole distribution | No | | Yes |
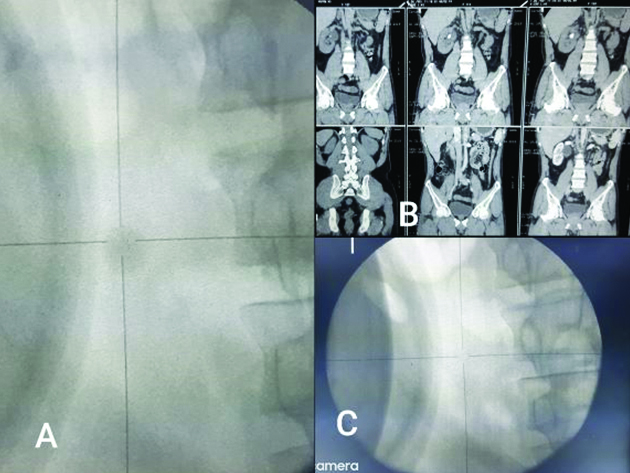
In this study, Dornier Compact Sigma manufactured by Dornier MedTech systems Gmbh, was used to generate electromagnetic shockwaves. The ESWL was performed with a gradual ramping up of shockwave energy at a fixed frequency rate of 60 shocks/minute. The patients underwent just a single ESWL session as part of this study. Treatment efficacy was studied using plain abdominal radiography of KUB, three weeks after ESWL [Table/Fig-2].
(A) Fluoroscopic image showing renal stone targeted by ESWL. (B) NCCT of the same patient showing stone in the renal pelvis. (C) Stone completely fragmented after ESWL.
Statistical Analysis
All the statistical analysis was done using IBM SPSS 26.0. Student’s t-test or Mann-Whitney U-test was used to compare continuous variables. Fisher’s-exact test and Chi-square test were used to analyse the cross charts between two categories. All p-values were based on two-sided statistical analysis. The p-value <0.05 were considered statistically significant.
Results
In this study, 120 patients formed the study population after complying with the inclusion and exclusion criteria. Total 9.20% and 34.09% of the patients had stones in the lower calyx in groups A and group B, respectively. This difference was statistically significant.
The mean±SD (in mm3) ellipsoid SV was 396.44±163.23 and 395.81±227.52, 52 patients in group A and B, respectively. Using the Independent samples t-test, the p-value was 0.049 (<0.05), thus the difference in the stone volume in the two groups are statistically significant.
The mean±SD (in HU) stone density was 724.28±210.90 and 814.56±190.63 in group A and group B, respectively. Using the student’s t-test, the p-value was 0.001.
The mean±SD Quadruple-D score was 2.09±0.65 and 1.54±0.79 in group A and B, respectively. Using the Mann-whitney U-test, the p-value was <0.001. Thus, Quadruple-D score can be used as an important clinical tool to predict the success rate of ESWL [Table/Fig-3].
Comparison of the study population 3 weeks after ESWL.
| Parameters | Overall (n=120) Mean±SD | Group A (n=76)(Stone free)Mean±SD | Group B (n=44) (Residual stone) Mean±SD | p-value |
|---|
| Age (years) | 40.335±9.77 | 34.90±9.11 | 45.77±10.43 | 0.453* |
| Sex |
| Male | 75 (62.50%) | 47 (61.84%) | 28 (63.63%) | 0.845** |
| Female | 45 (37.50%) | 29 (38.15%) | 16 (36.36%) |
| BMI (kg/m2) | 24.62±1.06 | 24.36±1.12 | 24.89±1.00 | 0.327* |
| Laterality |
| Left | 67 (55.83%) | 43 (56.57%) | 24 (54.54%) | 0.829** |
| Right | 53 (44.16%) | 33 (43.42%) | 20 (45.45%) |
| Stone location |
| Upper Calyx | 3 (2.5%) | 2 (2.63%) | 1 (2.26%) | 0.014*** |
| Middle calyx | 12 (10%) | 7 (9.22%) | 5 (11.36%) |
| Lower calyx | 22 (18.33%) | 7 (9.22%) | 15 (34.09%) |
| Renal pelvis | 14 (11.67%) | 10 (13.15%) | 4 (9.09%) |
| PUJ | 69 (57.5%) | 50 (65.78%) | 19 (43.18%) |
| Stone volume | 396.12±195.37 | 396.44±163.23 | 395.81±227.52 | 0.049* |
| Mean CT attenuation (HU) | 769.42±200.76 | 724.28±210.90 | 814.56±190.63 | 0.001* |
| SSD (cm) | 11.59±0.9 | 11.39±0.94 | 11.79±0.86 | 0.422* |
| Quadruple-D score |
| Total | 1.81±0.72 | 2.09±0.65 | 1.54±0.79 | <0.001**** |
| Score 0 | 5 (4.16%) | 0 | 5 (11.36%) |
| Score 1 | 24 (20%) | 11 (14.47%) | 13 (29.55%) |
| Score 2 | 72 (60%) | 49 (64.47%) | 23 (52.27%) |
| Score 3 | 17 (14.17%) | 14 (18.42%) | 3 (6.82%) |
| Score 4 | 2 (1.67%) | 2 (2.63%) | 0 |
SSD: Skin-to-stone distance; PUJ: Pelvi-ureteric junction; HU: Hounsfield unit
*Independent Samples t-test; **Chi-Squared test; ***Fisher’s-exact probability test; ****Mann-Whitney U-test
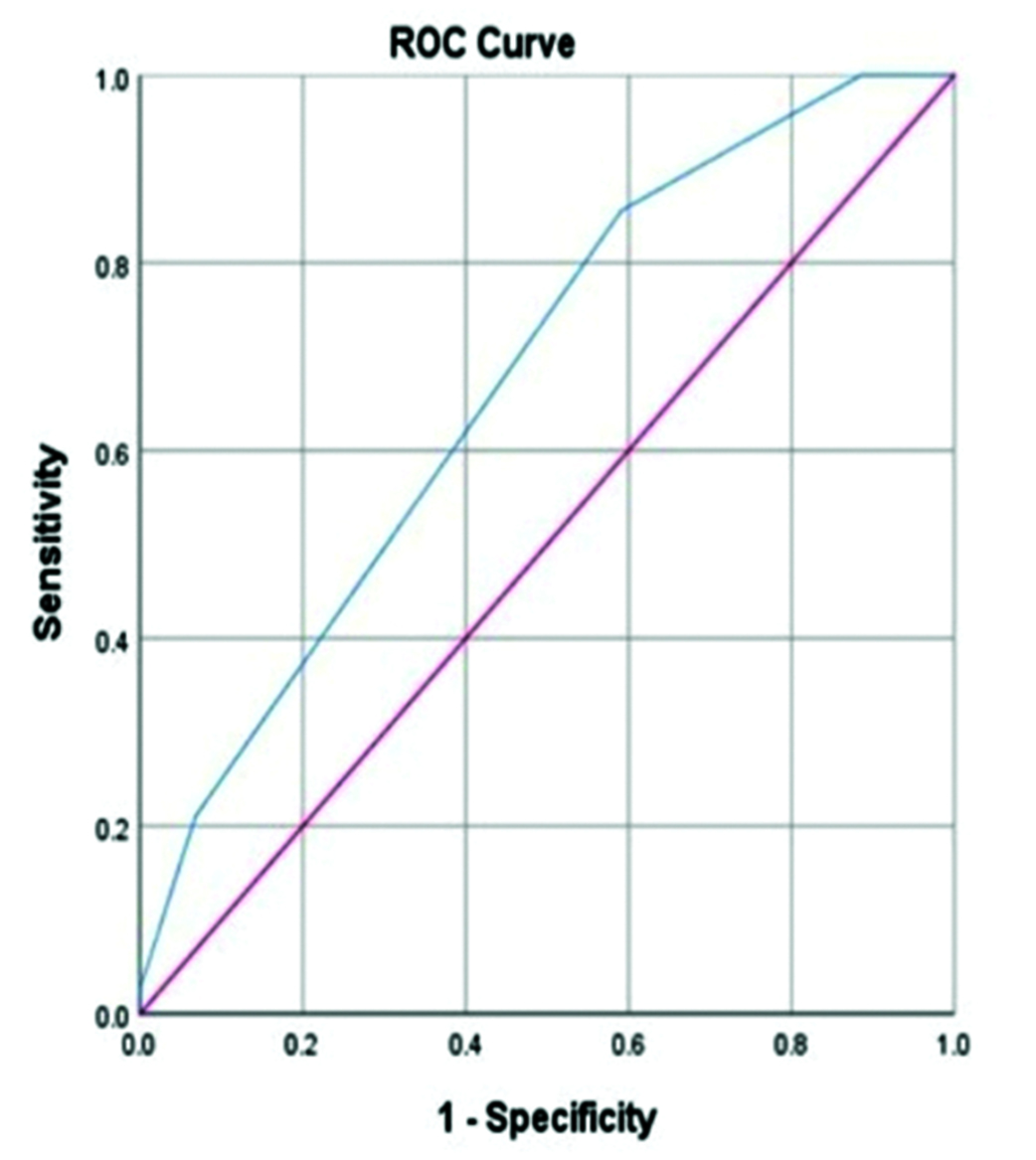
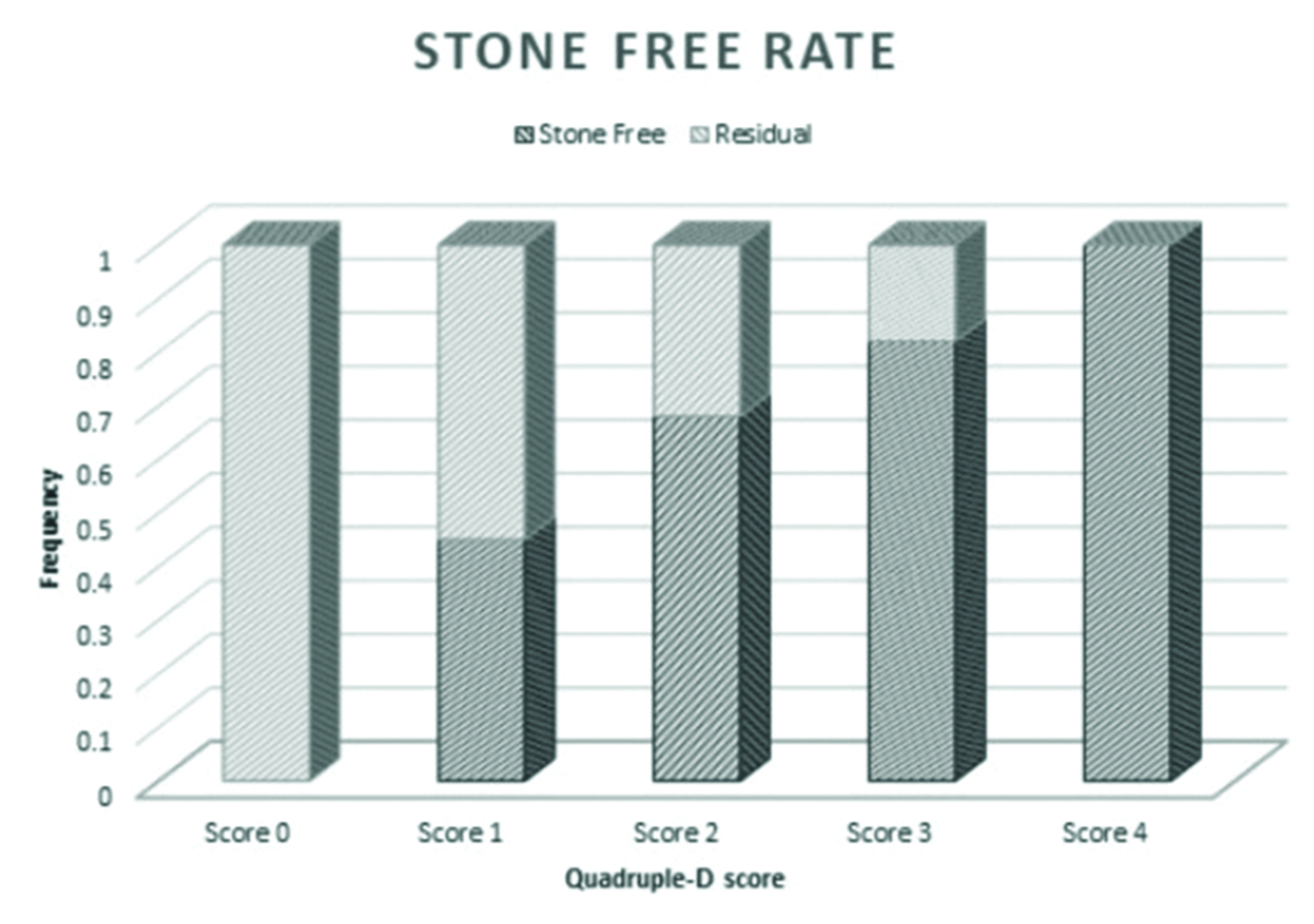
The AUC of Quadruple-D scoring system was 0.674 with 95% confidence interval of 0.57-0.77 (p=0.01). The Quadruple-D score of 0, 1, 2, 3 and 4 points showed SFR of 0%, 45.83%, 68.05%, 82.35% and 100%, respectively [Table/Fig-4,5].
ROC curve for Quadruple-D score.
AUC (Area Under the Curve): 0.674; 95% Confidence interval: 0.57-0.77
Stone Free Rate (SFR) based on Quadruple-D scoring system.
The age, sex, BMI, laterality of the stone and skin to stone distance were not statistically significant for the prediction of stone-free status.
Discussion
In this study, it was found that Quadruple-D score is a significant predictor of SFR after ESWL for 1-2 cm renal stones. With increasing Quadruple-D score, the SFR improved. These findings support the use of Quadruple-D scoring system to predict success of ESWL in the study population with renal stones between 1-2 cm.
The ROC curve analysis revealed a low AUC of 0.674 for Quadruple-D score for SFR prediction. In a similar study by Ichiyanagi O et al., the AUC of Quadruple-D score was 0.651. The SSD was not a significant factor predicating SFR [14]. This is because SSD, a component of Quadruple-D, is not a statistical significant factor for discriminating stone-free or residual outcomes after ESWL. Contrary to the present study, SSD and BMI, which are clinical indicators of obesity, have been reported as significant predictor of ESWL outcome in multivariate analysis [16,17]. The SSD or BMI were not related to the SWL outcomes in the present study, possibly because the study population consisted of mostly under privileged, low socioeconomic status patients (mean BMI of 24.62±1.06 kg/m2), reflecting racial background different from previous similar studies [8,16-18].
A lower pole location of renal stone was found to be a significant factor related to poor SFR after ESWL. An obtuse infundibulo-pelvic angle, long lower calyx (<1 cm) and narrow infundibulum (<5 mm) are depicted as unfavourable factors for ESWL success [1]. However, these details were not incorporated in Quadruple-D score for ease of use in clinical practice. Increased stone burden, lower polar location and increased SSD, all decrease success rate of ESWL and URS but has limited influence on PCNL outcomes [4]. So, for 1-2 cm renal calculi, stone and anatomical factors must be carefully considered when considering ESWL as a treatment modality. In a similar study, Ozgor F et al., revealed the importance of stone location in addition to Triple-D score for predicting ESWL success in their multivariate analysis [13].
In the present study, age was not a significant predictor of ESWL success rate. Contrary to this observation, age was reported as an independent predictor of ESWL outcomes in multivariate analyses [14,16,19]. In another prospective study [17], age and ESWL success rate reached a statistical significance in a univariate analysis but not in multivariate analysis. So, age is not considered a parameter of Triple-D and Quadruple-D scoring systems. There are also other studies where age was not found to have any significant impact on ESWL outcome [16,20-22]. In a study correlating the age with ESWL efficacy [23], it was seen that renal stones were difficult to fragment with ESWL in older patients than younger patients. There is also a higher probability of renal haematoma after ESWL, incidence of which increased with age. So, age might have an overall negative impact on SFR.
Many nomograms exist to predict successful outcome after ESWL [3,11,16,22,24,25]. Though these have excellent outcomes yet they are often too complex to calculate in clinical settings. In a nomogram by Kim JK et al., manual scoring system was formulated using four to six variables on graphical chart in a CT-dependent or independent manner [25]. Beside the four variables (sex, stone location, number and maximal diameter) hydronephrosis grade and stone CT attenuation were included in the CT dependent nomogram. Quadruple-D scoring system is practical and easy to use in clinical practice and remains externally validated.
Limitation(s)
The infundibulo pelvic angle, infundibular length and width of lower calyx and hydronephrosis were not assessed. It is not clear how to extrapolate Quadruple-D score for ureteral stones. Further studies are needed to confirm the validity of the present findings.
Conclusion(s)
Quadruple-D scoring system is still in its incipient stage of acceptance and further studies on this scoring system will definitely make a favourable impact in the management of nephrolithiasis. It is a user friendly and readily available clinical tool to predict the best modality of treatment in renal stone patients.
SSD: Skin-to-stone distance; PUJ: Pelvi-ureteric junction; HU: Hounsfield unit
*Independent Samples t-test; **Chi-Squared test; ***Fisher’s-exact probability test; ****Mann-Whitney U-test