Acute Respiratory tract Infections (ARIs) are most common cause of morbidity and mortality among children under five years of age. According to the World Health Organisation (WHO), ARI accounts for 30-60% of paediatric consultations at health facilities and attributes to almost 30-40% of admissions to hospitals [1]. Though majority of the viral acute respiratory infections like RV, Adenovirus and Influenza A virus in children are self-limiting and present as common cold like illness, however, various other risk factors like low birth weight, under nutrition, poor breast feeding, specific nutritional deficiencies, the infecting agent, co-infections and virulence of the pathogens determine its severity and need for hospitalisation [1].
In case of hospitalised patients, diagnosis of causative agents is of utmost importance for appropriate and specific management. ALRI is caused by bacteria like Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumonie etc or viral agents like Influenza A, B and C, Parainfluenza 1,2,3 and 4, RSV etc., may present with clinically indistinguishable syndrome, in absence of appropriate diagnostic test, patients are treated empirically with antibiotics leading to increased treatment cost and selection of antimicrobial resistant bugs [2-4].
There are few studies regarding profile of viral pathogens causing ALRI and their associated clinical presentation and seasonal variation in children under five years particularly in this geographical region [3,5]. With the availability of rapid molecular techniques like multiplex qPCR, simultaneous amplification of multiple pathogens in a single reaction mixture is possible. In this prospective study, conducted at a tertiary care centre, the study was aimed to characterise the viral spectrum in ALRI in hospitalised children under five years of age.
Materials and Methods
The present study was a prospective study which was conducted at the Paediatric ward of 1700 bedded hospital, a tertiary care facility affiliated to Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. Ethical clearance was taken from ethical committee of the institute, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi (IEC/VMMC/SJH/Thesis/October/2016). Before enrollment of the patient, Legally Authorised Representative (LAR) consent form was filled by either of the parent or guardian accompanying the child.
Inclusion criteria: During the study period of two years from June 2015 to May 2017 children aged ≤5 years of age attending the paediatric emergency or hospitalised with the signs and symptoms of ALRI like presence of fever, breathlessness, cyanosis, respiratory wheezing, cough and need of vasopressors were enrolled in the study.
Exclusion criteria: The clinical presentation, duration of hospital stay and presence of co-morbid conditions were recorded in a predesigned performa. Those children with chronic respiratory diseases or any history of respiratory infections in the previous 15 days were excluded from the study.
The diagnosis of ALRI was made by attending paediatrician based on clinical signs and symptoms. Only the cases of ALRI were enrolled into the study. Based on clinical presentation, the ALRIs cases were classified as less severe, severe and very severe ALRI according to WHO criteria [6]. A throat and nasal swab was collected using a sterile nylon flocked swabs and transported in Viral Transport Medium (VTM) at 4-8°C to the laboratory. Viral nucleic acid was extracted from 200μl sample in VTM using QIAamp One-For-All Nucleic Acid kit (by QIAGEN GmbH). Multiplex qPCR assays were performed on RotorGene 3000/6000/Q using primer probe mix (5 sets) of FTD respiratory pathogens 21 kit (Fast Track Diagnosis, Luxembourg) had been used for the detection of (18 viruses, two subtypes RSV A and B, Human Metapneumovirus (HMPV) A and B and Mycoplasma pneumoniae) influenza A, influenza A (H1N1) pdm09, influenza B, Human Coronavirus NL63 (HCoV-NL63), 229E (HCoV 229E), OC43 (HCoV-OC43) and HKU1 (HCoV HKU1), Human Parainfluenza Viruses 1, 2, 3, and 4 (HPIV- 1, 2, 3 and 4), (HMPV A/B), Human Rhinovirus Virus (HRV), RSV A/B, Human Adenovirus (HAdV), EV, Human Parechovirus (HPeV), and Human Boccavirus (HBoV). Total nucleic acid extraction and detection was done as per manufacturer instructions.
Statistical Analysis
All the data were analysed by using Statistical Package for the Social Sciences (SPSS) version 20.0. Continuous and categorical data were presented as mean±Standard Deviation (SD) and frequencies (percentages), respectively. A comparison of categorical variables between different virus group was performed by logistic regression. Multivariate analysis and singular value decomposition was adjusted for gender, age, history and underlying risk factors. The p-value was calculated and p-value <0.05 by chi-square method, were considered as statistically significant.
Results
During the two year period, a total of 512 children aged ≤5 years with ALRI presenting in emergency or requiring hospitalisation were enrolled in the study and 195 were excluded due to inadequate sample or incomplete clinical history. A total of 317 patients with ALRI were further studied and investigated. Overall, highest number of ALRI cases were observed in children up to six months i.e., 38.9% (n=123) as given in [Table/Fig-1]. The mean age of ALRI was found to be 9±1 month and M:F ratio was 2:1 and median duration of hospital stay was three days.
Age wise distribution of ALRI cases.
| Age group (months) | No of cases of ALRIs (n=317) |
|---|
| 0-6 | 123 (38.9%) |
| 6-12 | 94 (29.4%) |
| 12-24 | 47 (14.8%) |
| 24-60 | 53 (16.9%) |
Co-relation of severity of ALRI and viral pathogen: Based on the PCR results, cases were divided into Group A: viral ALRI and Group B: non-viral ALRI. The multiplex qPCR detected one/more viruses in 185/317 children (58.3%). The association of viruses by severity of ALRI is shown in [Table/Fig-2]. It was observed that majority of the children with ALRI had less severe infection (210/317, 66%) and viruses were more commonly isolated from less severe ALRI 125/210 (59.5%) and this difference was statistically significant. The spectrum of various clinical presentation has been analysed along with detection of the virus in the ALRI cases is given in [Table/Fig-3].
Viral detection in various group of acute respiratory infections cases.
| Total (317) | Group A: Viral ALRI N=185 (58.3)* | Group B: Non-viral ALRI N=132 (41.7) | p-value |
|---|
| Less severe ALRI (N=210) | 125 | 85 | <0.05 |
| Severe ALRI (N=41) | 22 | 19 | >0.05 |
| Very severe ALRI (N=66) | 38 | 28 | >0.05 |
*fig in parenthesis indicate percentage (%)
Clinical presentation and virus detection.
| Patient characteristics | Group A Viral ARLI (n) | Group B Non-viral ARLI (n) | p-value |
|---|
| Age (Mean±SD) | 1.5±0.6 years | 2.2±0.8 years | |
| Sex M:F | 3:2 | 2:1 | |
| Cough | 167 (90.3%) | 123 (89.8%) | 0.42 |
| Difficulty breathing | 149 (80.5%) | 105 (76.6%) | 0.89 |
| Chest retraction | 61 (32.9%) | 47 (34.3%) | 0.63 |
| Lethargy | 20 (10.8%) | 10 (7.3%) | 0.44 |
| Convulsion | 2 (1.0%) | 0 (0%) | 0.51 |
| Underlying heart disease | 15 (8.1%) | 12 (8.8%) | 0.84 |
| Asthma | 25 (13.5%) | 17 (12.4%) | 1.00 |
| Recurrent hospitalisation | 20 (10.8%) | 11 (8.0%) | 0.56 |
| Crepitus/wheezing/rhonci | 162 (87.6%) | 110 (80.3%) | 0.32 |
| CRP positive | 21 (11.3%) | 14 (10.2%) | 0.86 |
| Chest X-ray showing infiltration/consolidation | 56 (30.2%) | 33 (24.1%) | 0.31 |
| Hospital stay (median) | 1.9 days | 2.6 days | 0.07 |
CRP: C-reactive protein
Identification of viral pathogens detected in 185 ALRI cases: The distribution of respiratory viral pathogens, including co-infections in ALRI cases is shown in [Table/Fig-4]. Among the children (n=185) positive for viral pathogens, single virus infections predominated 118/185 (63.8%) whereas infection with more than one virus were observed only in 67/185 (36.2%) cases only. The RSV was most frequently detected single viral infections causing ALRI i.e., in 21.6% (64/185) children. Most co-infections were observed with HRV 36/59. The most common virus detected in the study (including single and co-infection) was RSV in 96/185 (51.9%), followed by HRV 43/185 (23.2%). Among Influenza A viruses, H3N2 was detected in 9/185 (4.9%) and HINI was detected in 6/185 (3.2%) cases. Among the 67 co-infectioned ALRI cases as observed in the study, majority (47/67) were detected in children more than 1 year.
Distribution of respiratory viruses detected from 185 ALRI cases (Including Co-Infection).
| Viruses detected by qPCR | No. of cases (n) |
|---|
| Monoinfections | (n=92) |
| H1N1 | 02 |
| Inf B | 11 |
| HRV | 07 |
| BV | 08 |
| RSV | 64 |
| Co-infections | (n=59) |
| H3N2+H1N1 | 02 |
| HRV+hmPV | 03 |
| HRV+RSV | 16 |
| HRV+H1N1 | 02 |
| HRV+BV | 13 |
| HRV+H3N2 | 02 |
| RSV+H3N2 | 05 |
| RSV+OC43 | 08 |
| RSV+PIV2+PIV3 | 03 |
| hmPV+OC43 | 04 |
| PIV1+PIV2 | 01 |
| Others*(includes both mono and co-infections of other viruses) | 34(26+8) |
*Other 10 viruses includes: Corona virus 229E, Corona virus NL63, HKV1, Corona virus OC43, Parainfluenza virus 1, Parainfluenza virus 2, Parainfluenza virus 3, Parainfluenza virus 4, Parechovirus and Enterovirus; HRV: Human rhinovirus; hmPV: Human metapneumovirus; BV: Bocavirus; RSV: Respiratory synticial virus; AV: Adeno virus
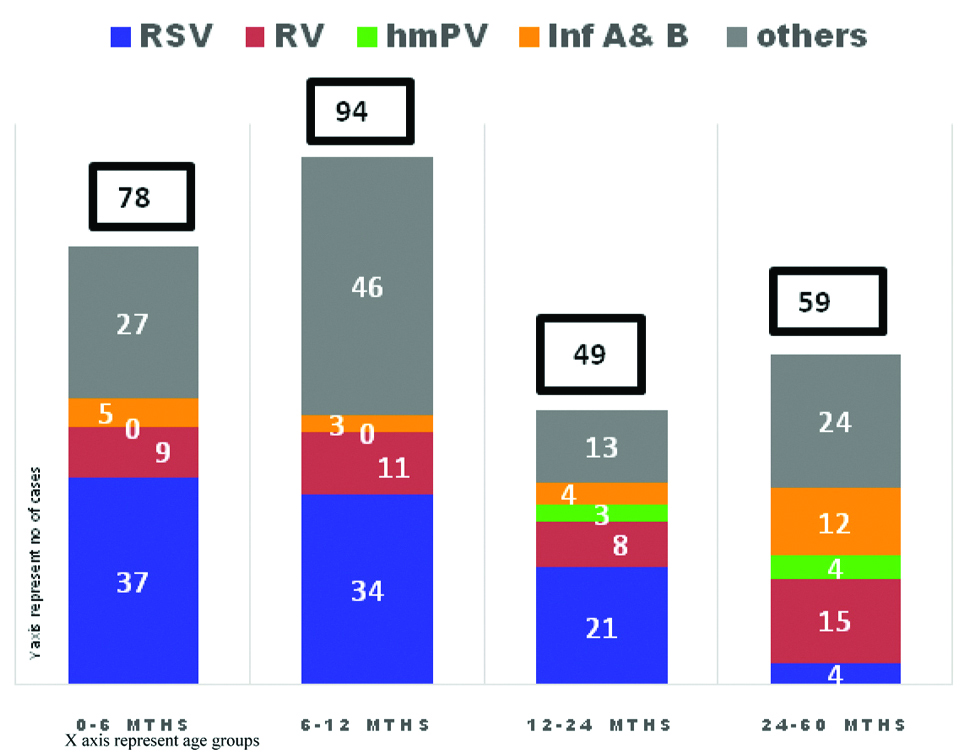
Age wise distribution of viral pathogens: The age wise distribution of the viral pathogens is shown in [Table/Fig-5]. Majority of the viral ALRI were observed in the children less than 1 year. RSV was most frequently isolated pathogen among infants with ALRI. It has been found that RSV had statistically significant (p<0.05) association with children age group 0 to 6 months, 6 to 12 months and 12 to 24 months i.e., p-value 0.04, 0.005 and 0.02, respectively. Influenza cases were more frequently observed in children older than two years of age.
Age wise distribution of 4 common viral pathogens.
In cases of co-infections each virus counted seperately. Others includes-Corona virus 229E, Corona virus NL63, HKV1, Corona virus OC43, Parainfluenza virus 1-4, Parechovirus, Enterovirus, Bocavirus, Adeno virus
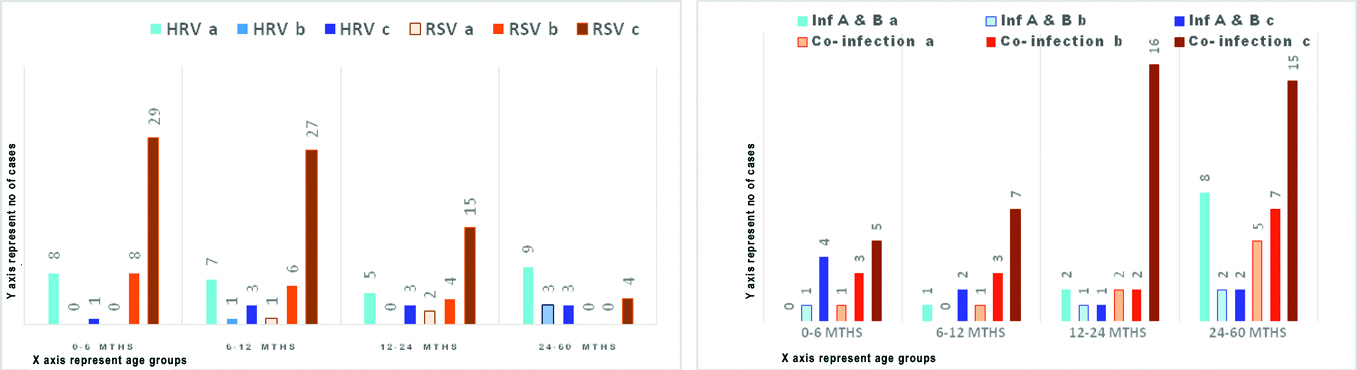
Agewise distribution of viral pathogen and its severity: As depicted in [Table/Fig-6a,b], severity of diseases varies with pathogen type, co-infections and age group. It was observed that RSV and co-infections were frequently associated with very severe ALRI, statistically significant (p<0.05) association was observed in infants and children with 2 to 5 years of age. In contrast, HRV infections seen in all age groups and usually presented as less severe ALRI. Influenza A and B infections were associated with less severe ALRI and very severe ALRI in children above two years and less than six months children respectively.
(a and b): Co-relation of agewise distribution of viral pathogen and its severity.
Note: Correlation of age wise distribution of respiratory viruses with severity of ALRI. Each respiratory pathogen illness is divided according to clinical severity into less severe ALRI, severe ALRI and very severe ALRI as represented by bar a, b and c, respectively
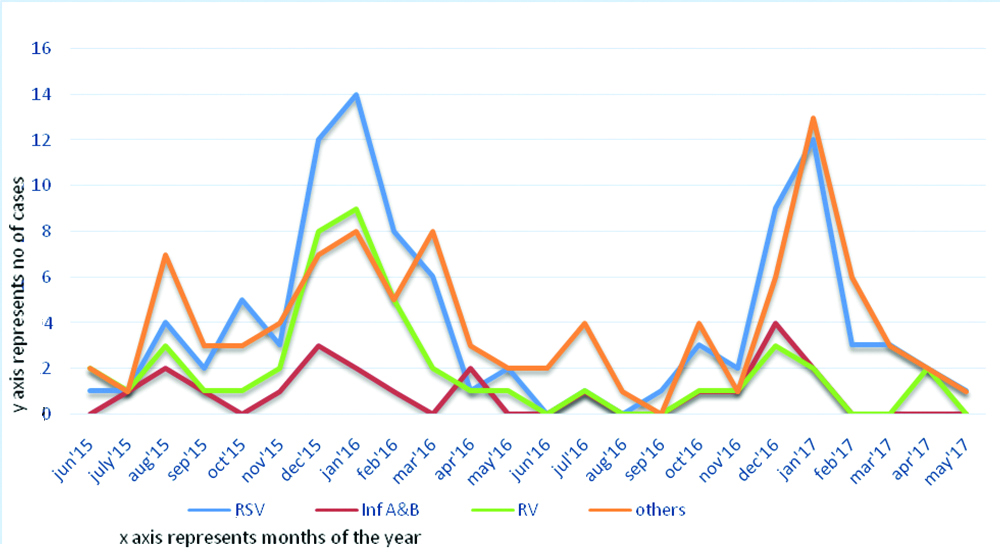
Seasonal distribution of viral ALRI: During the study, all respiratory viruses were predominant during the winter months though viral pathogens were isolated throughout the year as shown in [Table/Fig-7]. Maximum cases of RSV were observed in December and January and HRV also showed a similar pattern (data not shown).
Monthly distribution of viral identification throughout study period from June’15 to May’17.
Discussion
The high global burden of ARIs emphasise the importance of identification of various pathogens especially viruses for clinical management. This prospective study on viral ALRI in hospitalised children under five years identifies the viral aetiology and study its correlation with severity, age and seasonal distribution. A total of 317 hospitalised ALRI cases, aged under five years were enrolled for the study. Based on WHO criteria [6] of clinical severity cases were classified as given in the [Table/Fig-2]. Many a times based on severity empirical therapy given may lead unnecessary antibiotic use, antibiotic resistance, longer hospitalisation and indirectly to nosocomial infection and burden to the health care system. This can be reduced by use of multiplex qPCR, which allows detection of multiple pathogen in single test and it also allows rapid diagnosis and precise clinical practice [3].
In this study, viruses were predominant cause of ALRI and detected in 185/317 (58.3%) cases caused by one or more viruses. These findings are comparable to previous reports describing high prevalence of single and mixed viral infections [2,3]. The majority of the viral infections presented with less severe ALRI. Although the present study did not quantify the infective virus but it has been observed that severity of the disease is determined by viral load [3,4].
A comparison of clinical presentations among children with respiratory viral infections by different viruses unveiled some similarities in their presentations. The mean age group of the children in which virus has been detected was found to be 1.5±0.6 years and much younger to non-viral ALRI group. This was explained in study by Bharaj P et al., that respiratory viral load is more in children under 1.5 years which makes its detection easier [3]. Even though for various other clinical parameters the p-value was not statistically significant but it can be clearly seen that there is greater chance of virus detection in the presence of symptoms like cough, chest retraction, additive breath sound, increased C-Reactive Protein (CRP) and abnormal chest X-ray. Again median duration of hospital stay of 2.6 days was longer for non-viral ALRI in comparison to 1.9 days for ALRI group. A study done by Mishra P et al., in eastern part of India also describes similar demographic and clinical presentation in viral ALRI group [7]. They found higher number of children presenting with preceding bronchiolitis were significantly associated with total viral infections.
The availability of high cost of tests like qPCR has improved the understanding of the role of respiratory viruses as pathogens in hospitalised children. The predominant viral pathogens detected in this study were RSV in 34.5% and HRV (co-infection) in 19.4% cases, respectively. In India, the rates of RSV detection in various hospital- based studies done in children vary from 5-54% [5,8,9]. This differences in rates of RSV detection in these studies are due to different study cohort, and the method used for RSV diagnosis. A study by Malhotra B et al., done in Rajasthan of India which is geographically closer to present study area showed that in children under five years age, Human metapneumo virus was the predominant virus detected in 25.7% children followed by 19.9% influenza A (H1N1) pdm09. In contrary, RSV was found as low as 4.41% [8]. The authors have attributed this to low number of children enrolled in the age group of 0-12 months as RSV infection was more common in them.
The other important understanding from this study was the age specific differences in various viral pathogens and their association with severity. In this study, prevalence of respiratory pathogens were found to be higher in infants with more predilection to RSV. This is in concordance with other studies where RSV contributes ALRI as high as 68% and 97% in 12 months and 24 months respectively [9,10]. So, infant suffering from ALRI must be tested for RSV to prevent severity and to start specific treatment, and hMPV was characteristically detected in children above one year. Interestingly, HRV was seen prevalent in all age group of children. In contrast, the study by Visseaux B et al., from France had reported HRV are major aetiology for ALRI in children less than 15 years [11].
The clinical presentation of the two most common viral pathogens, RSV and HRV was quiet different. RSV infections were associated with severe and very severe ALRI in infancy and in contarst HRV infections were associated with less severe diease irrespective of the age group in children less than five years. Although majority of Influenza A and B cases were detected in children above two years but it was clearily understood that whenever found in infants caused very severe ALRI. According to a meta-analysis done by Lukšić V et al., among all hospitalised children below five years of age found severe ALRI caused by Adeno virus, Influenza virus and Parainfluenza virus accounted for 8.8%, 7.0% and 5.8%, respectively [12] which is quiet contrary to findings of this study. But again it can be attributed to geographical areas of the studies taken for meta-analysis. Present study findings are similar to the studies of neighbouring area done by Bharaj P et al., and Malhotra B et al., [3,8].
The third important understanding of the study was the seasonal association of the various viruses which is important for prevention, diagnosis and treatment of infection in a timely manner. In the study, it was observed that there is peak in all viral respiratory pathogens during autumn and winter seasons of this region, as expected from temperature climate changes. Globally, RSV epidemics start in the South moving to the North [12,13]. Similar to other studies from same region of India, in this study also RSV detection primarily increased during September and October and this finding was very similar to the observation made in five year long community based in the country [14]. However as reported by Paul SP et al., in present study also authors observed the peaks for HRV were in winter but HRV cases were reported through out the year suggesting that HRV is a year round cause of ALRI in children causing hospitalisation [15].
The wider availability of molecular diagnosis techniques has allowed the detection of more than one virus in single test. The importance of viral co-infections in the pathogenesis of ALRI is unclear; furthermore, there is paucity of data from India on the possible impact of age on viral co-infection prevalence. The current study suggests presence of more than one virus in paediatric patients admitted to hospital with ALRI is frequent and is frequently observed after first year of age. These findings were similar to previously reported studies using multiplex PCR for diagnosis [9,16,17]. The clinical significance of these co-infection observed in this study (shown in [Table/Fig-6b]), was that higher percentage of children with mixed infections had severe and very severe ALRI in children above 1 year age. These findings supported the study of Wang H et al., which had explained that this co-infection might lead to more severe disease [4]. This study gives the brief idea that although RSV tends to cause severe illness but other respiratory virus co-infections can aggravate the illness.
Limitation(s)
One of the major limitations of the study that there was lack of correlations of clinical outcome with the viral aetiologies. The quantification of viral aetiology could have given us idea about the the quantity of virus with the severity of disease.
Conclusion(s)
There is no doubt that the wide availability of multiplex PCR for viral diagnosis has improved the understanding of burden and clinical presentation of various viruses in ALRI especially in children. The identification of virus/viruses makes the treatment more precise and effective, thereby, contribute to shorter hospital stay, less use of empirical antibiotics, lesser nosocomial infection, and reduces emergence of resistant bugs. However, the utility of these expensive test in clinical practice and their impact on antibiotic prescribing rates remains to be investigated further as data is limited. But this test plays significat role in preventing severity of illness especially in scenerio of outbreaks like H1NI or RSV.
*fig in parenthesis indicate percentage (%)
CRP: C-reactive protein
*Other 10 viruses includes: Corona virus 229E, Corona virus NL63, HKV1, Corona virus OC43, Parainfluenza virus 1, Parainfluenza virus 2, Parainfluenza virus 3, Parainfluenza virus 4, Parechovirus and Enterovirus; HRV: Human rhinovirus; hmPV: Human metapneumovirus; BV: Bocavirus; RSV: Respiratory synticial virus; AV: Adeno virus