Adenomyosis and Co-existing Gynaecological Pathologies
Parul Garg1, Harjot Kaur2, Ishwer Tayal3, Shilpa4, Navjot Kaur5
1 Assistant Professor, Department of Pathology, Guru Gobind Singh Medical College, Faridkot, Punjab, India.
2 Professor, Department of Pathology, Sri Guru Ram Das Institute of Medical Sciences and Research, Amritsar, Punjab, India.
3 Assistant Professor, Department of Forensic Medicine and Toxicology, Guru Gobind Singh Medical College, Faridkot, Punjab, India.
4 Junior Resident 2nd Year, Department of Pathology, Guru Gobind Singh Medical College, Faridkot, Punjab, India.
5 Junior Resident 2nd Year, Department of Pathology, Guru Gobind Singh Medical College, Faridkot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Parul Garg, H. No. 81, Guru Gobind Singh Medical College Campus, Sadiq Road, Faridkot-151203, Punjab, India.
E-mail: pathology_parul45@ggsmch.org
Introduction
Adenomyosis is defined as presence of benign endometrial tissue comprising of both endometrial glands and stroma into the myometrium leading on to diffuse enlargement of the uterus. Adenomyosis co-exists with various pathologies such as leiomyomas, endometriosis, endometrial polyp, endometrial hyperplasia and carcinoma suggesting hyperestrogenism to be a factor in pathogenesis of adenomyosis.
Aim
To study the associated pathological conditions and histopathological patterns of endometrium in patients presenting with Abnormal Uterine Bleeding (AUB) due to adenomyosis.
Materials and Methods
This retrospective study was conducted in a tertiary care institute of Punjab, India for a period of two years (August 2018 to August 2020). All the patients who underwent hysterectomy were re-evaluated and cases diagnosed with adenomyosis were included in the study. Clinical details were recorded. A total of 101 patients were diagnosed with adenomyosis. These cases were reviewed for presenting symptoms and were associated with histological features of endometrium and other associated gynaecological pathologies. The quantitative variables were expressed as mean and qualitative variables as percentages.
Results
The age of the patients who had adenomyosis ranged from 29 to 79 years, majority were in the age group of 41-50 years. Abnormal uterine bleeding was the most common symptom. The histopathological examination revealed associated pattern of endometrium from proliferative endometrium to endometrial hyperplasia and endometrial carcinoma. Other gynaecological pathologies included leiomyoma, adenocarcinoma ovary, serous adenomas of ovary and Cervical Intraepithelial Neoplasia (CIN) grade 3. Co-existence with leiomyoma is most common. Hyperestrogenemia can be considered as a risk factor as it is associated with leiomyomas, endometrial hyperplasia, endometrial carcinoma or polyps.
Conclusion
Adenomyosis is one of the causes of AUB and this decreases the quality of life in women. It is also considered as a cause of infertility. The associated histopathological findings vary from leiomyoma, endometrial hyperplasia, endometrial polyps and rarely adenocarcinoma of endometrium and ovary. Meticulous and careful examination of gross and microscopic foci of adenomyosis and associated pathologies can help in better management of patients.
Abnormal uterine bleeding, Endometrial hyperplasia, Hyperestrogenemia, Hysterectomy, Leiomyoma
Introduction
Adenomyosis is defined as presence of benign endometrial tissue comprising of both endometrial glands and stroma into the myometrium. This leads on to diffuse enlargement of the uterus [1]. The histological diagnosis of adenomyosis is made by presence of endometrial tissue located at a distance range of 2 mm to 4 mm, or 1-2 low-power fields from the endometrio-myometrial junction [2]. The risk factors associated with adenomyosis are age of more than 40 years, multiparity, prior caesarean section, or uterine surgery [3,4]. Patient with adenomyosis presents with infertility, pain and AUB [5,6], but a third to half of the patients are asymptomatic [7]. It is considered a specific entity in classification of causes of AUB i.e., PALM-COEIN FIGO (Polyp; Adenomyosis; Leiomyoma; Malignancy and Hyperplasia; Coagulopathy; Ovulatory Dysfunction; Endometrial; Iatrogenic; and not yet classified- International Federation of Gynaecology and Obstetrics) [8]. There is a wide range of 8 to 20% of prevalence of adenomyosis in various studies from USA, Germany, Italy, Greece whereas it is 61.5% in Asian subcontinent [9]. Women undergoing Assisted Reproductive Technologies (ARTs) have a prevalence of 20% to 25% [5], whereas in those with a history of endometriosis, the percentage is widely variable, ranging from 20% to 80% [10,11]. Adenomyosis co-exists with various pathologies such as leiomyomas, endometriosis, endometrial polyp, endometrial hyperplasia and carcinoma. This suggests hyperestrogenism to be a factor in pathogenesis of adenomyosis [12,13]. Hyperestrogenic states leads on to non cyclic, anti-apoptotic activity of the basalis [14]. Diagnosis of adenomyosis is usually done on hysterectomy but nowadays MRI and transvaginal ultrasonography has helped in non invasive diagnosis of adenomyosis [8]. Despite the improvement of diagnostic tools, there is poor awareness of the condition [15]. The present study was done to relate the presenting symptoms of adenomyosis with histopathological findings of endometrium and to study its associated gynaecological pathologies.
Materials and Methods
This retrospective study was conducted in Department of Pathology, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India. The data over a period of two years; from August 2018 to August 2020 was collected and compiled in September and October 2020. All hysterectomy specimens received during this period were taken into consideration. Demographic and clinical details of the patient were collected from the histopathological requisition forms.
Inclusion criteria: All hysterectomies showing features of adenomyosis on microscopic examination were included in the study.
Exclusion criteria: Cases without adenomyosis and clinical details were excluded from the study.
Various clinical features of the patients along with associated pathological findings were evaluated.
Statistical Analysis
Clinical data was recorded, quantitative parameters were expressed as mean and qualitative parameters as percentage.
Results
A total of 101 hysterectomy specimens studied had adenomyosis as microscopic findings [Table/Fig-1,2]. The patients age ranged from 29 to 79 years. Majority of the cases were between 41-50 years, 48/101 (47.5%) [Table/Fig-3]. AUB was the most common symptom seen in patients 61/101 (60.3%) followed by prolapse in 18 cases (17.8%). Twenty-two patients (21.7%) were asymptomatic [Table/Fig-4]. Various endometrial patterns were studied [Table/Fig-5]. The most common endometrial pattern was proliferative endometrium seen in 40 (39.6%) cases. Secretory phase was seen in 17 cases [Table/Fig-5,6], atrophic in 15 cases and irregular in 23 cases. Endometrial hyperplasia was present in 04 cases (3.97%). Most common co-existing secondary pathology seen in hysterectomy specimens was presence of leiomyomata in 40 cases (39.7%) [Table/Fig-7] followed by endometrial polyp present in seven cases (6.9%) [Table/Fig-8]. Adenocarcinoma ovary was present in five cases and serous cyst adenoma in four cases [Table/Fig-9]. Sex cord stromal tumours were seen in three cases (two of granulosa cell tumour and one of fibrothecoma). Endometriosis of ovary, mucinous cystadenoma with pseudomyxoma peritonei and Cervical Intraepithelial Neoplasia (CIN) grade 3 were present in one case respectively.
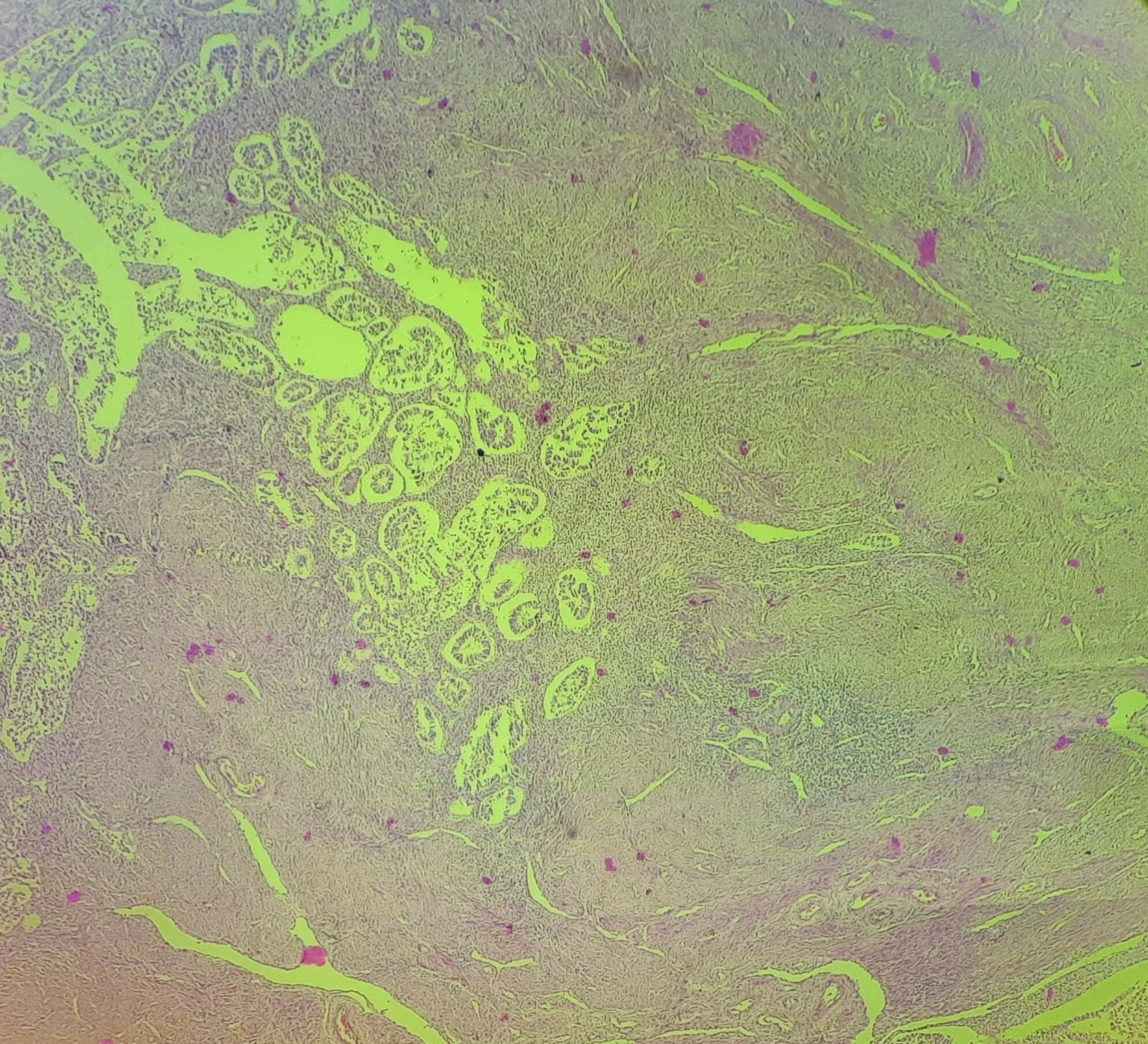
Endometrial gland and stroma infiltrating into the myometrium (H&E, 4X).
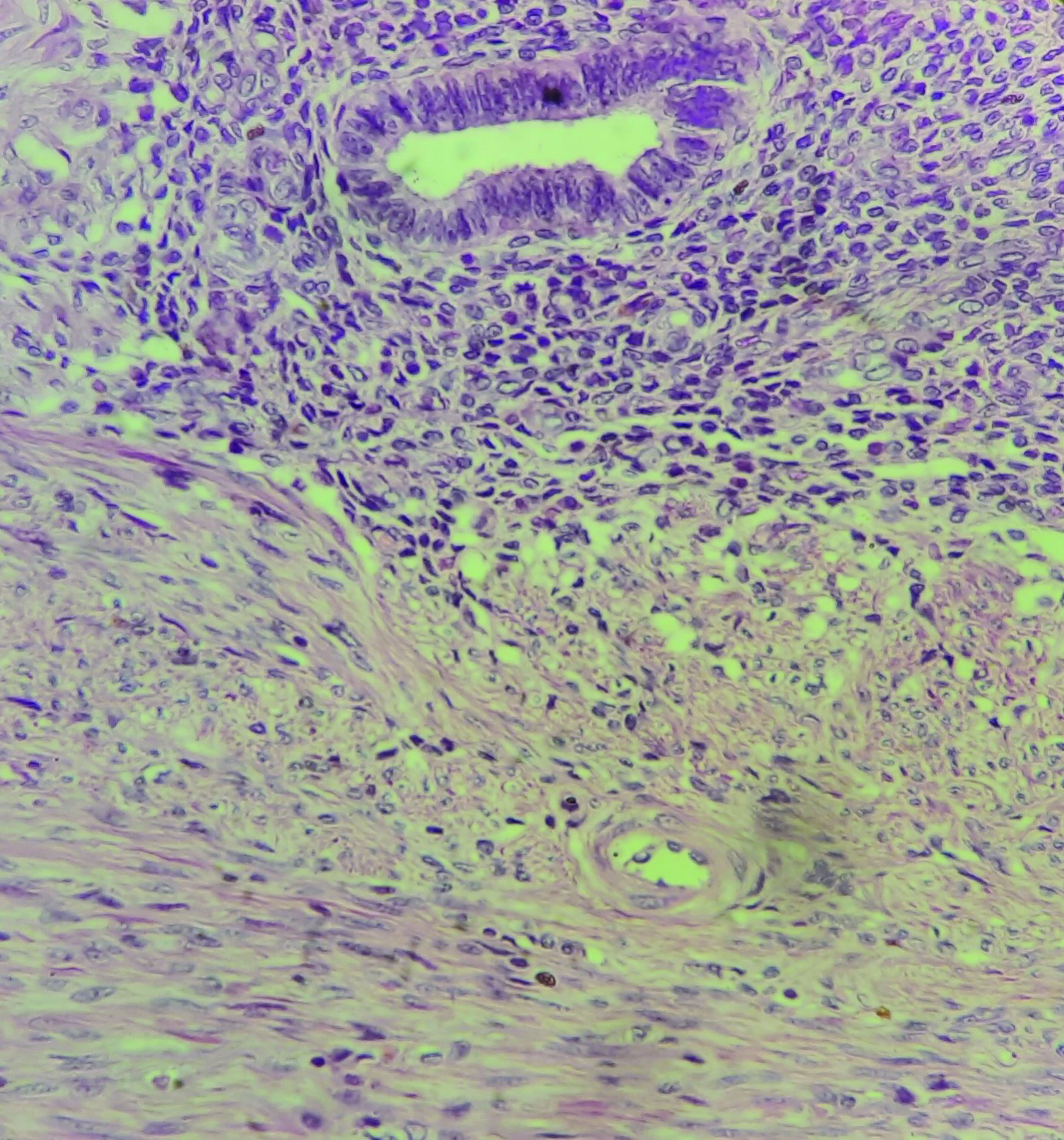
Endometrial gland and stroma in myometrium (H&E, 40X).
Frequency of adenomyosis in different age groups.
| Age group (years) | Number of cases | Percentage (%) |
|---|
| 21-30 | 2 | 1.98 |
| 31-40 | 24 | 23.76 |
| 41-50 | 48 | 47.52 |
| 51-60 | 19 | 18.82 |
| 61-70 | 6 | 5.94 |
| 71-80 | 2 | 1.98 |
| Total | 101 | 100 |
Presenting symptoms of patients with adenomyosis.
| Presenting symptoms | Number of cases | Percentage (%) |
|---|
| Abnormal uterine bleeding | 61 | 60.4 |
| Prolapse with pelvic pain | 18 | 17.8 |
| Asymptomatic | 22 | 21.8 |
Endometrial patterns associated with adenomyosis.
| Endometrial changes | Number of cases | Percentage (%) |
|---|
| Proliferative endometrium | 40 | 39.60 |
| Secretory endometrium | 17 | 16.83 |
| Atrophic endometrium | 15 | 14.85 |
| Irregular endometrium | 23 | 22.77 |
| Endometrial carcinoma | 2 | 1.98 |
| Endometrial hyperplasia | 4 | 3.97 |
| Total | 101 | 100 |
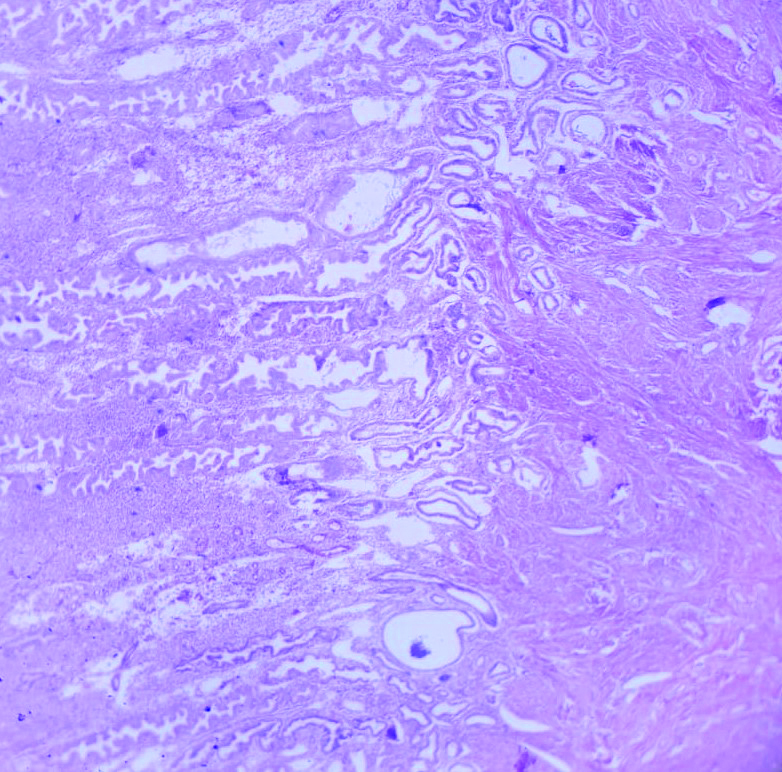
Secretory phase of endometrium in a patient with adenomyosis (H&E, 10X).
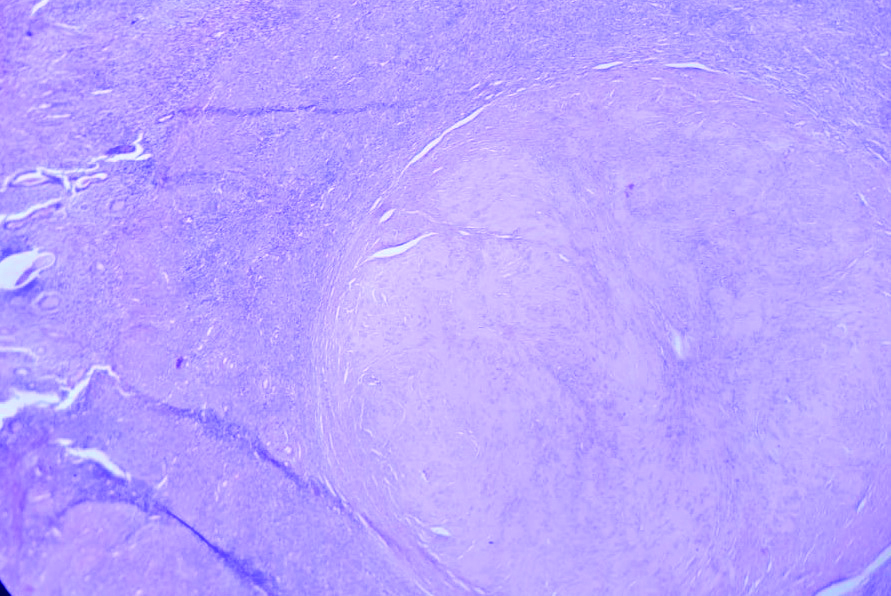
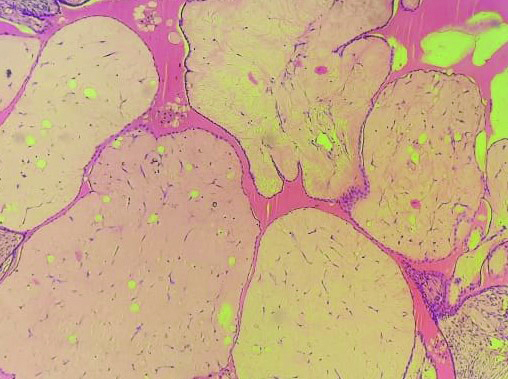
Leiomyoma (right side) along with adenomyosis (left upper corner) (H&E, E 10X).
Other gynaecological pathologies associated with adenomyosis.
| S. No. | Gynaecological pathologies associated with adenomyosis | Number of cases |
|---|
| 1 | Leiomyoma | | 40 |
| 2 | CIN III | | 01 |
| 3 | Adenocarcinoma ovary | | 05 |
| 4 | Serous cyst adenoma | | 04 |
| 5 | Sex cord stromal tumours | Granulosa | 02 |
| Fibrothecoma | 01 |
| 6 | Endometriosis of ovary | | 01 |
| 7 | Endometrial polyp | | 07 |
| 8 | Mucinous cystadenoma with pseudomyxoma peritonii | | 01 |
| Total | | 62 |
Serous adenoma ovary in a case of adenomyosis (H&E, 10X).
Discussion
Adenomyosis is a common incidental finding in hysterectomy specimens. But recent advancement in diagnostic techniques like Magnetic Resonance Imaging (MRI) and Ultrasonography has improved the diagnosis. In 1860, Carl Von Rokitansky coined the term cystosarcoma adenoids uterinum for adenomyosis. Later on, Bird CC et al., described the condition as benign endometrial tissue (glands and stroma) present ectopically in the hyperplastic and hypertrophied myometrium [13].
The various pathogenic factors involved in adenomyosis are sex steroid hormone receptors, inflammatory molecules, extracellular matrix enzymes, growth factors, and neuroangiogenic factors [16-18]. According to the most common theory, adenomyosis results from the invagination of basalis endometrium into the myometrium through an altered or interrupted Junctional Zone (JZ) [16,19] which represents a highly specialised hormone-responsive structure located in the inner third of the myometrium [20].
Adenomyosis is seen most commonly in age group of 41-50 [21,22]. Similar finding were seen in our study with 47.5% cases. Similar findings were noted in study by Shivananjiah C et al., and Ali A et al., with 50% and 73.7% cases, respectively in 41-50 years age group [21,22].
Patients with adenomyosis can be either asymptomatic or may present with symptoms like dysmenorrhea, dyspareunia, chronic pelvic pain, abnormal vaginal bleeding and infertility [23,24]. In present study, AUB was the most common symptom seen in 61/101 (60.4%) followed by prolapse in 18 cases (17.8%). Twenty-two patients (21.8%) were asymptomatic [Table/Fig-4].
In the present study, the most common endometrial pattern was proliferative endometrium seen in 40 cases (39.6%). Similar findings were noted by Shivananjiah C et al., with proliferative endometrium in 59.1% cases and Dayal S and Nagrath A in 44.4% of the cases [21,25]. In present study, 40 cases (39.6%) cases had co-existing leiomyoma. These findings were similar to study done by Sagar N et al., (41.4%) while Mehla S et al., showed a very low percentage (13.3%) of co-existence of adenomyosis and leiomyoma [7,26]. Many studies have reported the co-existence in a range of 15-57% cases [27]. Two studies showed a significant association between adenomyosis and endometrial hyperplasia [9,28]. In present study, only 04/101 (3.9%) cases were found to have endometrial hyperplasia. Adenomyosis is linked to hyperestrogenic states like endometrial polyps and endometrial carcinoma [29]. In present study, seven cases showed endometrial polyp (6.9%) and only two cases showed endometrial carcinoma.
Adenomyosis and endometriosis often co-exist in same patient showing a prevalence from 20 to 80% [10,11]. In our study, this co-existence is very low, only one case out of 101 (0.99%) showed the co-existence.
The most important factor in pathogenesis of adenomyosis seems to be hyperestrogenemia and it is associated with many gynaecological diseases. The present study was done to evaluate the clinical presentation of adenomyosis. Also, the endometrial changes and other gynaecological diseases associated with adenomyosis were also studied.
Limitation(s)
In the present study, the sample size may not represent a target population.
Conclusion(s)
Dysfunctional uterine bleeding is a major gynaecological problem which decreases the quality of life of a woman and adenomyosis is one of the major causes of it. Adenomyosis is associated with various histopathological findings which vary from leiomyoma, endometrial hyperplasia, endometrial polyps and rarely adenocarcinoma of endometrium and ovary. Proper diagnosis and treatment of adenomyosis and associated pathologies is important as it can help in better quality of life for females.
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? NA
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Nov 13, 2020
Manual Googling: Feb 25, 2021
iThenticate Software: Apr 01, 2021 (10%)
[1]. Brucker SY, Huebner M, Wallwiener M, Stewart EA, Ebersoll S, Schoenfisch B, Clinical characteristics indicating adenomyosis co-existing with leiomyomas: A retrospective questionnaire based studyFertil Steril 2014 101:237-41.10.1016/j.fertnstert.2013.09.03824188881 [Google Scholar] [CrossRef] [PubMed]
[2]. Tetikkurt S, Çelik E, Ta H, Cay T, Iik S, Usta AT, Co-existence of adenomyosis, adenocarcinoma, endometrial and myometrial lesions in resected uterine specimensMol Clin Oncol 2018 9(2):231-37.Epub 2018 Jun 1810.3892/mco.2018.166030101029 [Google Scholar] [CrossRef] [PubMed]
[3]. Vercellini P, Viganò P, Somigliana E, Daguati R, Abbiati A, Fedele L, Adenomyosis: Epidemiological factorsBest Pract Res Clin Obstet Gynaecol 2006 20(4):465-77.10.1016/j.bpobgyn.2006.01.01716563868 [Google Scholar] [CrossRef] [PubMed]
[4]. Li X, Liu X, Guo SW, Clinical profiles of 710 premenopausal women with adenomyosis who underwent hysterectomyJ Obstet Gynaecol Res 2014 40(2):485-94.10.1111/jog.1221124148010 [Google Scholar] [CrossRef] [PubMed]
[5]. Puente JM, Fabris A, Patel J, Patel A, Cerrillo M, Requena A, Adenomyosis in infertile women: Prevalence and the role of 3D ultrasound as a marker of severity of the diseaseReprod Biol Endocrinol 2016 14(1):6010.1186/s12958-016-0185-627645154 [Google Scholar] [CrossRef] [PubMed]
[6]. Naftalin J, Hoo W, Pateman K, Mavrelos D, Foo X, Jurkovic D, Is adenomyosis associated with menorrhagia?Hum Reprod 2014 29(3):473-79.10.1093/humrep/det45124408315 [Google Scholar] [CrossRef] [PubMed]
[7]. Sagar N, Tomar R, Balhara K, Mallya V, Mandal M, Khurana N, Histopathological association of adenomyosis with various gynaecological pathologiesAnnals of Pathology and Laboratory Medicine 2020 7(5):A221-23.10.21276/apalm.2825 [Google Scholar] [CrossRef]
[8]. Vannuccini S, Petraglia F, Recent advances in understanding and managing adenomyosisF1000 Res 2019 8:F100010.12688/f1000research.17242.130918629 [Google Scholar] [CrossRef] [PubMed]
[9]. Bergholt T, Eriksen L, Berendt N, Jacobsen M, Hertz JB, Prevalence and risk factors of adenomyosis at hysterectomyHum Reprod 2001 16:2418-21.10.1093/humrep/16.11.241811679531 [Google Scholar] [CrossRef] [PubMed]
[10]. Di Donato N, Montanari G, Benfenati A, Leonardi D, Valentina Bertoldo V, Giorgia Monti G, Prevalence of adenomyosis in women undergoing surgery for endometriosisEur J Obstet Gynecol Reprod Biol 2014 181:289-93. [Google Scholar]
[11]. Eisenberg VH, Arbib N, Schiff E, Goldenberg M, Seidman DS, Soriano D, Sonographic signs of adenomyosis are prevalent in women undergoing surgery for endometriosis and may suggest a higher risk of infertilityBiomed Res Int 2017 2017:8967803 [Google Scholar]
[12]. Arunachalam B, Manivasakan J, A clinicopathological study of adenomyosisJ Clin Diagn Res 2012 6:428-30. [Google Scholar]
[13]. Bird CC, McElin TW, Manalo Estrella P, The elusive adenomyosis of the uterus-revisitedAm J Obstet Gynecol 1972 112:583-93. [Google Scholar]
[14]. Bergeron C, Amant F, Ferenczy A, Pathology and physiopathology of adenomyosisBest Pract Res Clin Obstet Gynaecol 2006 20(4):511-21. [Google Scholar]
[15]. Van den Bosch T, Van Schoubroeck D, Ultrasound diagnosis of endometriosis and adenomyosis: State of the artBest Pract Res Clin Obstet Gynaecol 2018 51:16-24. [Google Scholar]
[16]. Vannuccini S, Tosti C, Carmona F, Huang SJ, Chapron C, Guo SW, Pathogenesis of adenomyosis: An update on molecular mechanismsReprod Biomed Online 2017 35(5):592-601. [Google Scholar]
[17]. Carrarelli P, Yen CF, Arcuri F, Funghi L, Tosti C, Wang TH, Myostatin, follistatin and activin type II receptors are highly expressed in adenomyosisFertil Steril 2015 104(3):744-52 e1. [Google Scholar]
[18]. Carrarelli P, Yen CF, Funghi L, Arcuri F, Tosti C, Bifulco G, Expression of inflammatory and neurogenic mediators in adenomyosisReprod Sci 2016 24(3):369-75. [Google Scholar]
[19]. García-Solares J, Donnez J, Donnez O, Madeleine Dolmans M, Pathogenesis of uterine adenomyosis: Invagination or metaplasia?Fertil Steril 2018 109(3):371-79. [Google Scholar]
[20]. Brosens I, Derwig I, Brosens J, Fusi L, Benagiano G, Pijnenborg R, The enigmatic uterine junctional zone: The missing link between reproductive disorders and major obstetrical disorders?Hum Reprod 2010 25(3):569-74. [Google Scholar]
[21]. Shivananjiah C, Nayak A, Swarup A, Honappa S, Swaminathan KR, Pathadan DS, Histopathological pattern of endometrium in AdenomyosisIndian Journal of Obstetrics and Gynecology Research 2016 3(2):101-03. [Google Scholar]
[22]. Ali A, The incidence of adenomyosis in hysterectomiesPak J Med Res 2005 44:38-40. [Google Scholar]
[23]. Sun YL, Wang CB, Lee CY, Wun TH, Lin P, Lin YH, Transvaginal sonographic criteria for the diagnosis of adenomyosis based on histopathologic correlationTaiwan J Obstet Gynecol 2010 49(1):40-44. [Google Scholar]
[24]. Graziano A, Lo Monte G, Piva I, Caserta D, Karner M, Engl B, Diagnostic findings in adenomyosis: A pictorial review on the major concernsEur Rev Med Pharmac Sci 2015 19(7):1146-54. [Google Scholar]
[25]. Dayal S, Nagrath A, Pattern and frequency of endometrial and ovarian pathologies with adenomyosis uteri in patients who attended the tertiary care hospital among rural population of North IndiaMAC Journal of Medical Sciences 2015 1(3):147-50. [Google Scholar]
[26]. Mehla S, Singh M, Chutani N, Clinicopathological correlation of adenomyosis and leiomyoma in hysterectomy specimens as the cause of abnormal uterine bleeding: A retrospective studySch J App Med 2014 2:3320-23. [Google Scholar]
[27]. Taran FA, Weaver AL, Coddington CC, Stewart EA, Characteristics indicating adenomyosis co-existing with leiomyomas: A case-control studyHum Reprod 2010 25(5):1177-82. [Google Scholar]
[28]. Parazzini F, Mais V, Cipriani S, Busacca M, Venturini P, Determinants of adenomyosis in women who underwent hysterectomy for benign gynecological conditions: Results from a prospective multicentric study in ItalyEur J Obstet Gynecol Reprod Biol 2009 143:103-06. [Google Scholar]
[29]. Verit FF, Yucel O, Endometriosis, Leiomyoma and Adenomyosis: The risk of gynecologic malignancyAsian Pac J Cancer Prev 2013 14(10):5589-97. [Google Scholar]