Accuracy of 3D Curvilinear Measurements on Digital Models Generated by Light Emitting Diode Scanned Impressions: A Cross-sectional Study
Ismatfatema Mohsin Nayani1, Manish Suresh Agrawal2, Jiwanasha Manish Agrawal3, Shradhha Shetti4, Bhakti Bhalekar5, Akash Agarwal6
1 Postgraduate Student, Department of Orthodontics and Dentofacial Orthopaedics, Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India.
2 Professor, Department of Orthodontics and Dentofacial Orthopaedics, Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India.
3 Professor, Department of Orthodontics and Dentofacial Orthopaedics, Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India.
4 Assistant Professor, Department of Orthodontics and Dentofacial Orthopaedics, Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India.
5 Postgraduate Student, Department of Orthodontics and Dentofacial Orthopaedics, Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India.
6 Postgraduate Student, Department of Orthodontics and Dentofacial Orthopaedics, Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manish Suresh Agarwal, Jagdamba Niwas, Plot No. 1, Ekta Colony, Sangli-416416, Maharashtra, India.
E-mail: drmanishortho2011@gmail.com
Introduction
The advantages of digital models include customisation of appliances such as retainers, expanders, and indirect bracket setups for which measurements made along a curved line (curvilinear), would offer clinically more relevant information as opposed to linear measurements.
Aim
To evaluate and compare the accuracy of 3 Dimensional (3D) curvilinear measurements on Digital models generated from Light Emitting Diode (LED) scanned impressions, with manual measurements on study models.
Materials and Methods
The cross-sectional study consisted of maxillary arch rubber based impressions of eight patients based on inclusion criteria of intact dentition having complete set of teeth with erupted second molar. These impressions were scanned with LED scanner (Medit Identica) and converted to Stereolithography (STL) files to generate 3D models. With the help of Ansys software curvilinear measurements were obtained from these models. These impressions were poured in dental stone to prepare study models and manual measurements were directly carried out on it with the help of brass wire and digital caliper. Measurements were made on different locations on the dental arch in various directions as the labial and palatal surface of central incisors and canine on left side along the long axis of the tooth from the cusp tip to the gingival margin and the buccal and palatal surface between the two interdental contact points of 2nd premolars. Unpaired t-test was used to check the significant difference in means of different parameters.
Results
No significant differences were found between central incisors labial surface (p=0.845) and palatal surface (p=0.722) and the canine measurements labial surface (p=0.721) and palatal surface (p=0.544) on digital models compared to study models, whereas significant difference was observed in premolar measurements (p=0.008).
Conclusion
Stereolithography (STL) files obtained by LED scanning the impressions did not exhibit significant deformation or loss of information while curvilinear measurements were evaluated, and higher accuracy was seen in the premolar measurement on palatal surface with digital models.
Ansys, 3 Dimensional diagnosis and treatment planning, Reliability, Software
Introduction
The advances in computer sciences have resulted in increased usage of newer technologies in every field. Orthodontics has also been influenced by this phenomenon. Computer-based records have several advantages: easy access, need for less physical space, and ability to share information via the Internet with other professionals [1]. A 3D digital model scanning is an indirect imaging technique with advances in 3D orthodontic software’s, orthodontists can examine in all three planes, sagittal, vertical and transverse. This also has the advantage of allowing a “virtual treatment” and a “virtual setup” [2].
There are studies in the literature which have verified the accuracy of angular and linear measurements on 3D digital models with different software’s and found different results [3-9]. Although differences between both models exist, the digitally produced models can be reproduced and used clinically. Bell A et al., study stated that there was no statistically significant differences between linear measurements made on digital and conventional models [10]. But studies of measurements on curve surface or curvilinear measurement are not reported to our knowledge except Mack S et al., study in which they have measured curve surface of tooth using intraoral scanners [11].
The advantages of digital models include customisation of appliances such as retainers, expanders, and clear retainers [12], indirect bracket setups can be done with high precision decreasing the need for repositioning later in treatment, it provides convenient access to study the models, less space and maintenance compared to physical models and transfer of records without physical damage [1].
The impressions which are taken digitally with intraoral scanners are very accurate as compared to other options [9,13]. But when it comes to chair side time and patient tolerance then alginate impressions are still preferred [14,11]. There are very few studies assessing the accuracy of impression scanned models using surface measurements made along a curved line (curvilinear), which would offer clinically more relevant information as opposed to linear measurements constructed by only two points [11]. So, the aim of this study was to evaluate and compare the accuracy of 3D curvilinear measurements on digital models compared to dental study models.
Null Hypothesis
There is no statistically significant difference between curvilinear measurements obtained from 3D Digital models generated from LED scanned impression and manual measurements on study models.
Materials and Methods
The cross-sectional study was conducted in Bharati Vidyapeeth Dental College and Hospital, Sangli, Maharashtra, India, in the month of January 2018 and the time required was one and half month to complete the study. Ethical clearance was obtained from Institutional Ethical Committee (IEC approval number: BVDUMC&H/SANGLI/IEC/285/18) of Bharati Vidyapeeth (Deemed to be University) Dental College and Hospital Sangli, Maharashtra, India. The sample size was calculated before the study and it was estimated that a sample size of eight dental study models and digital models was needed to obtain a statistical power of 95% [11].
Inclusion and Exclusion criteria: The study sample comprised of eight rubber based impressions of maxillary arch based on inclusion criteria of intact dentition with complete set of teeth with erupted second molars. Exclusion criteria were presence of any prosthesis, restorations, fractured teeth, presence of any developmental anomalies or gingival pathologies.
Led Scanner Measurement
These maxillary arch impressions were scanned same day the impression was made with LED scanner (Medit Identica blue, Seoul, Korea) having twin camera with 1.3 mega pixel. Once the scan was complete, the raw images were converted to STL files to generate 3D dimensional models. With the help of the commercial software (Ansys Inc. version 19, Canonsburg, Pennsylvania, US) curvilinear measurements were obtained. The distance over a curved surface with shortest path of the curve is measured by the ruler tool.
Manual Measurement
Dental stone was poured in impressions and study models were prepared. Measurements on dental study models was done with brass wire which was marked from the beginning of the landmark ie., cusp tip to the gingival margin along the long axis of tooth for central incisor and canine and interdental contact points for 2nd premolar and carefully wrapped along the curve being measured. Once second landmark is reached another mark was placed. The brass wire was then straightened and the distance was measured with the help of digital caliper (aerospace).
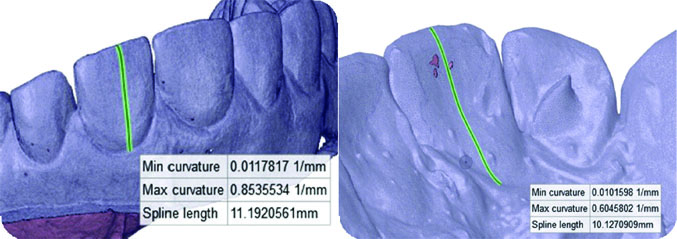
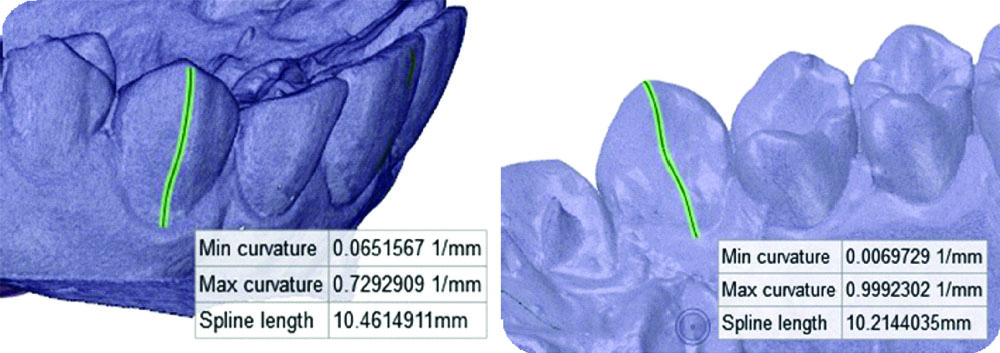
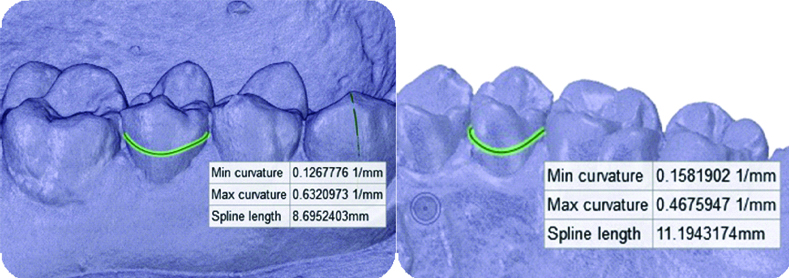
Measurements were performed in different aspects of the maxillary arch in various directions. The following curvilinear measurements were made: the labial and palatal surface of central incisors on left side along the long axis of the tooth from the cusp tip to the gingival margin [Table/Fig-1]; the labial and palatal surface of canines on left side along the long axis of the tooth from the cusp tip to the gingival margin [Table/Fig-2]; and the buccal and palatal surface between the two interdental contact points of 2nd premolars [Table/Fig-3]. All measurements were carried out by the same operator and evaluated to the nearest of 0.01 mm [11].
The labial and palatal surface of central incisors.
The labial and palatal surface of canine.
The buccal and palatal surface of second premolar.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) software (version 22.0; IBM, Armonk, NY) was used for statistical analysis. Measurements performed were six on three teeth on digital models and study models respectively. Mean and Standard Deviation (SD) were calculated. Unpaired t-test was used to check the significant difference in means of different parameters. Intra observer repeatability was evaluated using intraclass correlation analysis by repeating all measurements from five randomly selected models at a one month interval and all measurements were measured three time and mean average was recorded. Intra observer reliability of the measurements by a calibrated clinician resulted in a relatively small range of operator error with highly consistent repeated measurements. Intra observer error was assessed using Dalberg’s Formula. The level of significance was set at p-value <0.05 for all tests.
Results
Mean biases, Standard Deviation (SD), t-value and p-values for the paired method comparisons are shown in [Table/Fig-4]. There were no significant differences between central incisors labial surface (p=0.845) and palatal surface (p=0.722) and the canine measurements labial surface (p=0.721) and palatal surface (p=0.544) on digital models compared to study models. Whereas significant difference was observed in premolar measurements on palatal surface (p=0.008) with higher accuracy seen in digital models to conventional models as the plaster models were considered as gold standard and the measurement of digital models were compared with them.
Curvilinear measurements obtained on digital and conventional models.
| Tooth | Groups | N | Mean(mm) | Sth. Deviation | t-value | p-value |
|---|
| Central Incisor LD vs LC | LD | 8 | 10.22 | 1.33 | -0.199 | 0.845 |
| LC | 8 | 10.368750 | 1.4683853 |
| Central Incisor PD vs PC | PD | 8 | 9.910788 | 1.4742997 | 0.365 | 0.722 |
| PC | 8 | 9.683750 | 0.9611294 |
| Canine LD vs LC | LD | 8 | 9.922000 | 1.6121294 | 0.364 | 0.721 |
| LC | 8 | 9.633750 | 1.5561210 |
| Canine PD vs PC | PD | 8 | 9.375975 | 1.2596242 | 0.623 | 0.544 |
| PC | 8 | 8.938750 | 1.5361402 |
| Premolar BD vs BC | BD | 8 | 8.365038 | 0.7997291 | 0.954 | 0.356 |
| BC | 8 | 8.002500 | 0.7179684 |
| Premolar PD vs PC | PD | 8 | 10.925938 | 0.6577875 | 3.101 | 0.008 |
| PC | 8 | 9.761250 | 0.8342736 |
Level of significance p≤0.05; Unit of measurements (mm); Unpaired t-test used; LD: Labial of digital model; LC: Labial of cast study model; PD: Palatal of digital model; PC: Palatal of cast study model; BD: Buccal of digital model; BC: Buccal of cast study model
Discussion
Studies have been reported in dental literature regarding the accuracy and validity of digital models compared to dental study models in respect to reproducibility of dental landmarks, measurements of mesio-distal width of teeth, arch width which are linear measurements and as diagnostic aid for treatment planning [8-10,15], using impressions scanned with LED or laser scanner or using intraoral scanners to generate digital files. Mack S et al,. study on 3D surface accuracy of intraoral scanners using curvilinear measurements was first to our knowledge to measure curve surface and brought to our notice importance of it which offers clinically more relevant information as opposed to linear measurements [11].
Impression scanning with LED scanner was used in this study because of its easy availability and feasibility for impression making to orthodontist. Intraoral scanners are expensive, time consuming procedure, and its findings might be affected by blood, saliva, and patient movements in-vivo [16,17], Also, differences in the light reflected back to the scanner can affect the scanner’s ability to determine the actual depth of an object accurately.
The STL generated from scanning the rubber based impressions where used with commercial software for curvilinear measurements, were the ruler was set to measure the true shortest path of a curve. This software allows moving the images around the three axis of rotation and magnifying the images. Magnification is an excellent advantage compared with the plaster models, because anatomic details can be viewed more accurately [11]. In some studies, it was demonstrated that it is possible to scan a patient intraorally to build satisfactory orthodontic clasps and other alloy components and embed them in a resin base without physical models [11,18]. One study concluded that the custom trays which were fabricated digitally are a closer match with the models of the patients as seen by the reserved impression space [19,11]. In comparison with handmade trays, digitally manufactured custom trays were more accurate.
Critical appraisal for this study is use of physical models which requires traditional manufacturing processes, impression materials would be necessary to obtain study model replications of the patient’s dentition and pouring with dental stone which are prone to deformation [20].
Hassan WNW et al,. compared measurements of digital calliper on plaster models vs 3D software on models scanned by structured-light scanner and concluded that measurements made on scanned models were in good agreement with manually made plaster models [21]. Fleming PS et al., concluded from its review article of orthodontic measurements on digital study models compared with plaster models that digital models offer a high degree of validity, similar result was found in this study [22]. The present study findings were similar to the findings of Mack S et al., study suggesting that STL files did not exhibit significant deformation or loss of information as evaluated by curvilinear measurements, and would provide a reliable surface area for appliance fabrication [11]. Significant difference was obtained in the premolars palatal region digital models obtained might contain small discrepancies this can be partially explained by registration errors of the patched 3D surfaces [11,23]. Gül Amuk N et al,. [24] compared digital models obtained from plaster dental model scanning and dental impression scanning and showed high accuracy and reliability. Intra observer reliability of the measurements by a calibrated clinician resulted in a relatively small range of operator error with highly consistent repeated measurements. Park SH et al,. measured the curved arch length and curved arch length discrepancy on model scanned digital model and intraoral scanned digital model which exhibited high validity when compared with the plaster models [25].
Clinical implications: As there is same accuracy between 3D curvilinear measurements on digital models generated from LED scanned impressions as compared with manual measurements on study models, so we can replace the plaster models with digital scanned impression models. This reduces the need for storage and maintenance problem and limits the physical damage to plaster models. The digital models can be stored in computer hard drive and potable CDs or on central server. There digital models are excellent tool for patient education that can be used to illustrate the improvement in treatment.
Limitation(s)
The sample size of the study was small. Only one type of scanning method was used. Further, with more sample examination more accurate and reliable results can be obtained. In future comparison of different scanning methods for its reliability to conventional models can be done.
Conclusion(s)
The accuracy of measurements of curve surface on digital models was found similar to direct measurements on the dental casts with a caliper in relation to all measured tooth surface. Measurements of curve surface on digitised models showed higher accuracy in relation to premolar tooth as interdental embrasure areas can be accurately measured with digital measuring software where brass wire cannot reach manually. Clinically, digital models can be used for appliance fabrication and customisation of brackets for the respected patients. Different scanning options should also be checked for its reliability to produce curve surface.
Level of significance p≤0.05; Unit of measurements (mm); Unpaired t-test used; LD: Labial of digital model; LC: Labial of cast study model; PD: Palatal of digital model; PC: Palatal of cast study model; BD: Buccal of digital model; BC: Buccal of cast study model
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jul 25, 2020
Manual Googling: Jan 27, 2021
iThenticate Software: Apr 14, 2021 (24%)
[1]. Marcel T, Three-dimensional on-screen virtual modelsAm J Orthod Dentofacial Orthop 2001 119:666-68.10.1067/mod.2001.11650211395713 [Google Scholar] [CrossRef] [PubMed]
[2]. Hajeer MY, Millett DT, Ayoub AF, Siebert JP, Applications of 3D imaging in orthodontics: Part IJ Orthod 2004 31(1):62-70.10.1179/14653120422501134615071154 [Google Scholar] [CrossRef] [PubMed]
[3]. Quimby ML, Vig KW, Rashid RG, Firestone AR, The accuracy and reliability of measurements made on computer-based digital modelsAngle Orthod 2004 74(3):298-303. [Google Scholar]
[4]. Leifert MF, Leifert MM, Efstratiadis SS, Cangialosi TJ, Comparison of space analysis evaluations with digital models and plaster dental castsAm J Orthod Dentofacial Orthop 2009 136(1):16.e1-4.10.1016/j.ajodo.2008.11.01919577140 [Google Scholar] [CrossRef] [PubMed]
[5]. Asquith J, Gillgrass T, Mossey P, Three-dimensional imaging of orthodontic models: A pilot studyEur J Orthod 2007 29(5):517-22.10.1093/ejo/cjm04417974542 [Google Scholar] [CrossRef] [PubMed]
[6]. Mullen SR, Martin CA, Ngan P, Gladwin M, Accuracy of space analysis with e models and plaster modelsAm J Orthod Dentofacial Orthop 2007 132(3):346-52.10.1016/j.ajodo.2005.08.04417826603 [Google Scholar] [CrossRef] [PubMed]
[7]. Stevens DR, FloresMir C, Nebbe B, Raboud DW, Heo G, Major PW, Validity, reliability, and reproducibility of plaster vs digital study models: Comparison of peer assessment rating and Bolton analysis and their constituent measurementsAm J Orthod Dentofacial Orthop 2006 129(6):794-803.10.1016/j.ajodo.2004.08.02316769498 [Google Scholar] [CrossRef] [PubMed]
[8]. Redlich M, Weinstock T, Abed Y, Schneor R, Holdstein Y, Fischer A, A new system for scanning, measuring and analyzing dental casts based on a 3D holographic sensorOrthod Craniofac Res 2008 11(2):90-95.10.1111/j.1601-6343.2007.00417.x18416750 [Google Scholar] [CrossRef] [PubMed]
[9]. Sousa MV, Vasconcelos EC, Janson G, Garib D, Pinzan A, Accuracy and reproducibility of 3-dimensional digital model measurementsAm J Orthod Dentofacial Orthop 2012 142(2):269-73.10.1016/j.ajodo.2011.12.02822858338 [Google Scholar] [CrossRef] [PubMed]
[10]. Bell A, Ayoub AF, Siebert P, Assessment of the accuracy of a three-dimensional imaging systems for archiving dental study modelsJ Orthod 2003 30(3):219-23.10.1093/ortho/30.3.21914530419 [Google Scholar] [CrossRef] [PubMed]
[11]. Mack S, Bonilla T, English JD, Cozad B, Akyalcin S, Accuracy of 3-dimensional curvilinear measurements on digital models with intraoral scannersAm J Orthod Dentofacial Orthop 2017 152(3):420-25.10.1016/j.ajodo.2017.05.01128863923 [Google Scholar] [CrossRef] [PubMed]
[12]. Kravitz ND, Groth C, Jones PE, Graham JW, Redmond WR, Intraoral digital scannersJ Clin Orthod 2014 48(6):337-47. [Google Scholar]
[13]. Wiranto MG, Engelbrecht WP, Tutein Nolthenius HE, van der Meer WJ, Ren Y, Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressionsAm J Orthod Dentofacial Orthop 2013 143(1):140-47.10.1016/j.ajodo.2012.06.01823273370 [Google Scholar] [CrossRef] [PubMed]
[14]. Grünheid T, McCarthy SD, Larson BE, Clinical use of a direct chairside oral scanner: an assessment of accuracy, time, and patient acceptanceAm J Orthod Dentofacial Orthop 2014 146(5):673-82.10.1016/j.ajodo.2014.07.02325439218 [Google Scholar] [CrossRef] [PubMed]
[15]. Naidu D, Scott J, Ong D, Ho CT, Validity, reliability and reproducibility of three methods used to measure tooth widths for Bolton analysesAust Orthod J 2009 25(2):97-103. [Google Scholar]
[16]. Flügge TV, Schlager S, Nelson K, Nahles S, Metzger MC, Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scannerAm J Orthod Dentofacial Orthop 2013 144(3):471-78.10.1016/j.ajodo.2013.04.01723992820 [Google Scholar] [CrossRef] [PubMed]
[17]. Hack GD, Patzelt SB, Evaluation of the accuracy of six intraoral scanning devices: An in-vitro InvestigationADA Prof Prod Rev 2015 10(4):01-05. [Google Scholar]
[18]. Al Mortadi N, Jones Q, Eggbeer D, Lewis J, Williams RJ, Fabrication of a resin appliance with alloy components using digital technology without an analog impressionAm J Orthod Dentofacial Orthop 2015 148(5):862-67.10.1016/j.ajodo.2015.06.01426522047 [Google Scholar] [CrossRef] [PubMed]
[19]. Chen H, Yang X, Chen L, Wang Y, Sun Y, Application of FDM three-dimensional printing technology in the digital manufacture of custom edentulous mandible traysSci Rep 2016 6:1920710.1038/srep1920726763620 [Google Scholar] [CrossRef] [PubMed]
[20]. Torassian G, Kau CH, English JD, Powers J, Bussa HI, Marie Salas-Lopez A, Digital models vs plaster models using alginate and alginate substitute materialsAngle Orthod 2010 80(4):474-81.10.2319/072409-413.120482351 [Google Scholar] [CrossRef] [PubMed]
[21]. Hassan WNW, SA Othman, CS Chan, Ahmad R, Ali SNA, Rohim AA, Assessing agreement in measurements of orthodontic study models: Digital caliper on plaster models vs 3-dimensionl software on models scanned by structured light scannerAmerican Journal of Orthodontics and Dentofacial Orthopedics 2016 150(5):886-95.10.1016/j.ajodo.2016.04.02127871715 [Google Scholar] [CrossRef] [PubMed]
[22]. Fleming PS, Marinho V, Johal A, “Orthodontic measurements on digital study models compared with plaster models: A systematic review”Orthod Craniofac Res 2011 14:01-16.10.1111/j.1601-6343.2010.01503.x21205164 [Google Scholar] [CrossRef] [PubMed]
[23]. van der Meer WJ, Andriessen FS, Wismeijer D, Ren Y, Application of intra-oral dental scanners in the digital workflow of implantologyPLoS One 2012 7:e4331210.1371/journal.pone.004331222937030 [Google Scholar] [CrossRef] [PubMed]
[24]. Gül Amuk N, Karsli E, Kurt G, Comparison of dental measurements between conventional plaster models, digital models obtained by impression scanning and plaster model scanningInt Orthod 2019 17(1):151-58.10.1016/j.ortho.2019.01.01430772351 [Google Scholar] [CrossRef] [PubMed]
[25]. Park SH, Byun SH, Oh SH, Lee HL, Kim JW, Yang BE, Evaluation of the reliability, reproducibility and validity of digital orthodontic measurements based on various digital models among young patientsJ Clin Med 2020 9(9):272810.3390/jcm909272832846984 [Google Scholar] [CrossRef] [PubMed]