Focal Periphyseal Oedema: A Physiologic Finding in Paediatric Knee Pain
Susana Rosa1, Margarida Freitas2, Sara Antunes3, Rute Pereira4
1 Medical Resident, Department of Physical Medicine and Rehabilitation, Centro Hospitalar Universitário Lisboa Central, Lisbon, Portugal.
2 Medical Resident, Department of Physical Medicine and Rehabilitation, Hospital Garcia de Ort, Almada, Portugal.
3 Medical Resident, Department of Physical Medicine and Rehabilitation, Hospital Garcia de Ort, Almada, Portugal.
4 Medical Resident, Department of Physical Medicine and Rehabilitation, Hospital Garcia de Ort, Almada, Portugal.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Susana Rosa, Medical Resident, Department of Physical Medicine and Rehabilitation, Centro Hospitalar Universitário Lisboa Central, Lisbon, Portugal.
E-mail: susanafrosa@gmail.com
Knee pain is a common reason for adolescent calls or visits to a primary care clinician. The authors present a case of a 14-year-old male adolescent with progressive bilateral nociceptive somatic knee pain. The pain was worse with weight bearing, and relieved at rest. It was located over the medial joint line. The patient was treated conservatively with nonsteroidal anti-inflammatory drugs and a rehabilitation program. Magnetic Resonance Imaging (MRI) showed bone marrow oedema, and Focal Periphyseal Oedema (FOPE) diagnosis was made. After a total of 6 months of treatment, the patient was asymptomatic. The literature is limited to a few case reports and radiologic studies describing this symptomatic physeal pathology, not reporting physical examination or treatment. The goals of this case report were to elucidate physicians of this condition, a newly reported cause of knee pain in adolescent, and to elicit the importance of a patient-tailored rehabilitation program in the treatment of this finding. FOPE is a clinical entity that should not be ignored and must be treated for the patient’s comfort. It is a self-limited condition and has an excellent prognosis.
Adolescent, Musculoskeletal pain, Physis
Case Report
A 14-year-old male adolescent presented with gradually progressive left knee nociceptive somatic pain for about one month after starting practicing Muay Thai, with no history of trauma. Pain was worse with squatting, jumping and running. He visited an Orthopaedic Surgeon two months after the beginning of the symptoms. His previous medical history included juvenile acne treated with isotretinoin, which he had suspended four months prior that evaluation. On the physical examination, fever was absent, he had no local swelling/deformity or systemic complaints, he referred pain at the medial joint line of the left knee, no limitation of the range of motion, although experiencing pain in the last 10° of knee passive flexion and no joint instability, a grade 4 muscle strength in Medical Research Council’s scale [1] of knee flexors and extensors and a positive McMurray’s test was observed (a painful click over the medial joint line was noticed while internally rotating the left knee with the patient’s thigh flexed to 90° degrees and moving the knee gradually from the fully flexed position to the fully extended position) [2], raising the suspicion of meniscal injury, for which the initial MRI investigation was performed. He presented normal tactile and pain sensitivity, evaluated with pinprick and light touch tests. The patient was asked to grade his pain using the Visual Analogue Scale (VAS) [3] and he referred a score of 1/10 at rest and a score of 7/10 with jumping, squatting and while playing sports. As indicated by the Orthopaedic Surgeon, he stopped sports activity and started taking ibuprofen 400 mg twice a day, for 5 days.
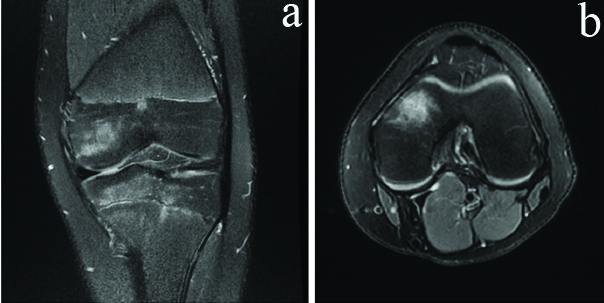
The MRI of the left knee showed hyper density in the anteromedial spongy bone of the internal femoral condyle, as well as in the internal anterior tibial plateau, reflecting bone oedema and assumed as contusion. There were no aspects that suggested fracture, although micro trabecular disruption was assumed, with bleeding associated with the oedema, without cortical discontinuity. Meniscal or ligament tears were excluded [Table/Fig-1].
Left knee showing a) Coronal fat-suppressed fast spin-echo T2 weighted image showing abnormal pattern of bone marrow oedema within both epiphysis and metaphysis centered about anteromedial central tibia; bone marrow oedema is also present in the medial femoral condyle. b) Axial fat-suppressed fast spin-echo T2-weighted image showing bone marrow oedema in the medial femoral condyle.
The patient was referred to a Physical Medicine and Rehabilitation (PMR) department, and started a rehabilitation program for two months. It consisted of a three times a week 60-minute sessions. The program’s objectives were pain control, muscle strengthening of the knee flexor and extensor muscles and ankle stabiliser muscles. The program included myofascial release massage, transcutaneous electrical nerve stimulation and dynamic muscle strengthening exercises. He started with closed kinetic chain exercises and evolved to an open kinetic chain exercises. Proprioception training was added by the end of the program, using unstable surfaces, focused on knee muscle strength and pain control [Table/Fig-2].
Subject during double leg squat (dynamic strength of knee extensor and flexor muscles and ankle stabilisers muscles).

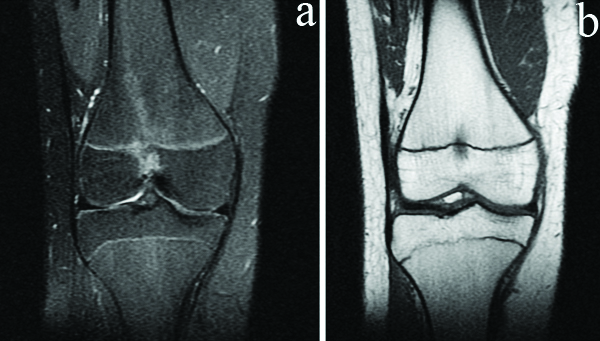
In the following PMR evaluation, he showed a gradual improvement of the symptoms and had fully recovered muscle strength. However, he referred a non specific pain in the right knee, worsening with impact and relieving at rest, with no ligament or meniscal positive signs on the examination. MRI was suggested, which revealed right knee had evidence of focal abnormal signal intensity noted at the distal femoral metaphyseal and epiphyseal bone marrow, indicating bone marrow oedema [Table/Fig-3].
Right knee showing a) Coronal fat-suppressed fast spin-echo T2-weighted image. A focal periphyseal oedema zone is evident in the distal femur. b) Coronal spin-echo T1-weighted image showing a hypointense bone marrow odema in the center of the femoral physis, extending into the adjacent metaphysis and epiphysis.
At this stage, due to the involvement of both knees, the patient was observed by a Rheumatologist but no inflammatory or autoimmune pathology were identified. This was hypothesised that isotretinoin could have musculoskeletal side-effects. Although isotretinoin treatment can be complicated by acute rhabdomyolysis with a secondary impairment of long bone healing due to muscle weakness, the patient had normal serum creatine phosphokinase. According to literature, a 16 to 20-week course of isotretinoin treatment at the recommended dose for severe acne has no clinically significant effect on lumbar spine and total hip bone mass density in the adolescent population [4]. For this reason, authors excluded a cause-and-effect relationship between isotretinoin uptake and knee pain in this patient.
In a re-evaluation appointment, discrete asymmetry of the lower limbs and a scoliotic posture was found. A long-leg radiograph confirmed an asymmetry of the lower limbs of about 1 cm and visible elevation of the right iliac crest [Table/Fig-4]. The patient started wearing an insole on the left shoe and he reported improvement in pain in the right knee and greater comfort during walking. He continued with the rehabilitation program adapted to the most recent complaints in the right knee for about 3 months. After a total of 6 months of treatment, the patient was asymptomatic, reporting a 0 score in VAS. Sports activities were gradually tolerated and he was able to perform daily activities. A FOPE diagnosis was made and the follow-up ended by that time.
Long-leg anteroposterior radiograph.

Discussion
A significant number of adolescents are affected by knee pain and related disabilities [5]. Usually, patients report activity-related knee pain with no prior history of knee trauma. Physical examination of these patients is often normal, radiographic evaluation may not demonstrate skeletal pathology and the diagnosis can be challenging. Most cases are associated to juvenile osteochondrosis and traction apophysitis affecting the extensor mechanism of the knee [6].
Authors here present a case that did not fall under any of the usual diagnosis, in addition to the fact that the diagnosis was not immediate. When the radiologic findings were identified, there were no stablished rehabilitation treatment protocol, since FOPE is a recent diagnosis. FOPE was first described in 2011 [7]. Since then, this diagnosis has been validated by several other publications, with similar cases of self-limiting, benign periphyseal oedema in the immature skeleton of adolescents provoked by stress of physeal closure as they approach fusion. It has been initially reported in the distal physis of femur and proximal physis of femur and tibia [8-11], but other authors published a case report of a child who was found to have a FOPE zone of the greater trochanteric apophysis, which had clinical and MRI findings similar to those previously described in the distal femur and proximal tibia physis [12].
FOPE zones are typically seen in 11-12-year-old females and in 13-14-year-old males. Clinically, patients may present a self-limited pain, with or without a history of acute injury [7,8,11]. Ueyama H et al., followed their patients for 2 years and there were no limb length discrepancies or malformation secondary to the FOPE lesion [10]. The exact cause of FOPE zones is still unknown. It is hypothesised to be a physiologic variant, maybe linked to early stages of physeal closure, probably a pain creator, and usually managed with support. However, other authors support the theory that trauma may play a role in its aetiology [9].
The differential diagnoses of FOPE zones includes infiltrative bone tumours, osteomyelitis, and physeal injury on MRI [8]. Distinguishing FOPE zones or physeal injuries in some cases is difficult because of the variety of types of physeal injuries. This case supports the current data suggesting that FOPE is a self-limited condition that should be treated with conservative measures and spontaneous resolution and does not require any invasive investigation [8]. This condition should be considered for patients with unexplained atraumatic adolescent knee pain. It has a mixed hypothesis of aetiology; in this case, authors cannot relate to trauma or a normal physiologic process (Muay Thai previous practice could have played a role). Follow-up radiographs and repeat MRI are pointless, particularly when symptoms are improving [7].
Published clinical cases regarding FOPE are essentially descriptive of the imaging characteristics and do not focus on the physical examination or treatment [9,10,12]. To our knowledge, this is the first clinical description eliciting the importance of a patient-tailored rehabilitation program in the treatment of this finding. This case report presents a contribution to the literature because it helps a better understanding of clinical evolution of FOPE, which is still underdiagnosed. This diagnosis is important to avoid confusing normal growth with a pathological condition.
Conclusion(s)
Focal Periphyseal Oedema (FOPE) is a self-limited condition that most of the times evolves to spontaneous resolution. MRI is mandatory to exclude infiltrative bone tumours, osteomyelitis, osteochondrosis and traction apophysitis. Treatment includes analgesia and physiotherapy. These patients should be evaluated by a multidisciplinary team. Further research is needed to clarify the incidence, risk factors, clinical prognosis of FOPE and to create a specific rehabilitation protocol.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes (by parents)
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Feb 16, 2021
Manual Googling: Apr 01, 2021
iThenticate Software: Apr 14, 2021 (14%)
[1]. Medical Research CouncilAids to the investigation of pe-ripheral nerve injuries 1943 2nd edLondonHer Majesty’s Stationery Office [Google Scholar]
[2]. Hing W, White S, Reid D, Marshall R, Validity of the McMurray’s test and modified versions of the test: A systematic literature reviewJ Man Manip Ther 2009 17(1):22-35.10.1179/10669810979081825020046563 [Google Scholar] [CrossRef] [PubMed]
[3]. Stinson JN, Kavanagh T, Yamada J, Gill N, Stevens B, Systematic review of the psychometric properties, interpretability and feasibility of self report pain intensity measures for use in clinical trials in children and adolescentsPain 2006 125:143-57.10.1016/j.pain.2006.05.00616777328 [Google Scholar] [CrossRef] [PubMed]
[4]. DiGiovanna JJ, Langman CB, Tschen EH, Jones T, Menter A, Lowe NJ, Effect of a single course of isotretinoin therapy on bone mineral density in adolescent patients with severe, recalcitrant, nodular acneJ Am Acad Dermatol 2004 51(5):709-17.10.1016/j.jaad.2004.04.03215523348 [Google Scholar] [CrossRef] [PubMed]
[5]. Saesa M, Soares M, Knee pain in adolescents: Prevalence, risk factors, and functional impairmentBraz J Phys Ther 2017 21(1):07-14.10.1016/j.bjpt.2016.04.00128442078 [Google Scholar] [CrossRef] [PubMed]
[6]. Achar S, Yamanaka J, Apophysitis and osteochondrosis: Common causes of pain in growing bonesAm Fam Physician 2019 99(10):610-18. [Google Scholar]
[7]. Zbojniewicz AM, Laor T, Focal periphyseal edema (FOPE) zone on MRI of the adolescent knee: A potentially painful manifestation of physiologic physeal fusion?Am J Roentgenol 2011 197(4):998-1004.10.2214/AJR.10.624321940591 [Google Scholar] [CrossRef] [PubMed]
[8]. Beckmann N, Spence S, Unusual presentations of focal periphyseal edema zones: A report of bilateral symmetric presentation and partial physeal closureCase Rep Radiol 2015 2015:46501810.1155/2015/46501826640734 [Google Scholar] [CrossRef] [PubMed]
[9]. Bai RJ, Zhan HL, Liu Y, Qian ZH, Ye W, Li YX, Focal periphyseal edema zone on MRI and clinical significance of the adolescent kneeZhonghua Yi Xue Za Zhi 2016 96(25):1965-70. [Google Scholar]
[10]. Ueyama H, Kitano T, Nakagawa K, Aono M, Clinical experiences of focal periphyseal edema zones in adolescent knees: Case reportsJ Pediatr Orthop B 2018 27(1):26-30.10.1097/BPB.000000000000038827606713 [Google Scholar] [CrossRef] [PubMed]
[11]. Sakamoto A, Matsuda S, Focal periphyseal edema zone on magnetic resonance imaging in the greater trochanter apophysis: A case reportJ Orthop Case Rep 2017 7:29-31. [Google Scholar]
[12]. Speirs JN, Shields TG, Morrison MJ 3rd, Focal periphyseal edema: An uncommon cause of adolescent knee pain: A report of three casesJBJS Case Connect 2019 9(3):e039110.2106/JBJS.CC.18.0039131365360 [Google Scholar] [CrossRef] [PubMed]