Introduction
The method of radiotherapy has moved away from two-dimensional and three-dimensional conformal radiotherapy towards Volumetric-Modulated Arc Therapy (VMAT) for advanced carcinomas. VMAT treatments often result in significant clinical advantage, particularly when concave dose distributions are required as is often the situation since these tumours are in close proximity to several critical structures.
Aim
To investigate the potential clinical role of volumetric arc therapy on cervical cancer patients and its comparison with fixed-field Intensity-Modulated Radiotherapy (IMRT) was used as a benchmark.
Materials and Methods
This retrospective study was conducted on 15 cervical cancer patients selected for radiotherapy treatment. These patients were previously treated with sliding window IMRT techniques during January 2020 to November 2020. For dosimetric comparison of sliding window IMRT techniques with RapidArc, a new set of plans were created using VMAT/RapidArc technique. For each patient two plans were generated and in this way total 30 plans were analysed. The prescription dose to Planning Target Volume (PTV) was 50.4 Gy in 28 fractions (1.8 Gy/fraction) for the 6 MV photon beam. Comparison of each plan done on the basis of Organs at Risk (OAR) sparing, coverage index (C), Conformity Index (CI), Homogeneity Index (HI), dose Gradient Index (GI), and Unified Dosimetry Index (UDI). This study utilised UDI scoring for evaluation and comparison of RapidArc and IMRT plans. Treatment Time (TT) for patient comfort and the number of Monitor Units (MUs) for long-term side-effects was also taken into consideration. A paired two-tailed t-test was executed for the dosimetric study of volumetric arc modulation with RapidArc and its comparison with the IMRT technique in the radiotherapy treatment of cervical cancer patients. All the collected data was analysed using Statistical Package for Social Sciences (SPSS) version 20.0. The p-value <0.05 was contemplated for the level of statistical significance.
Results
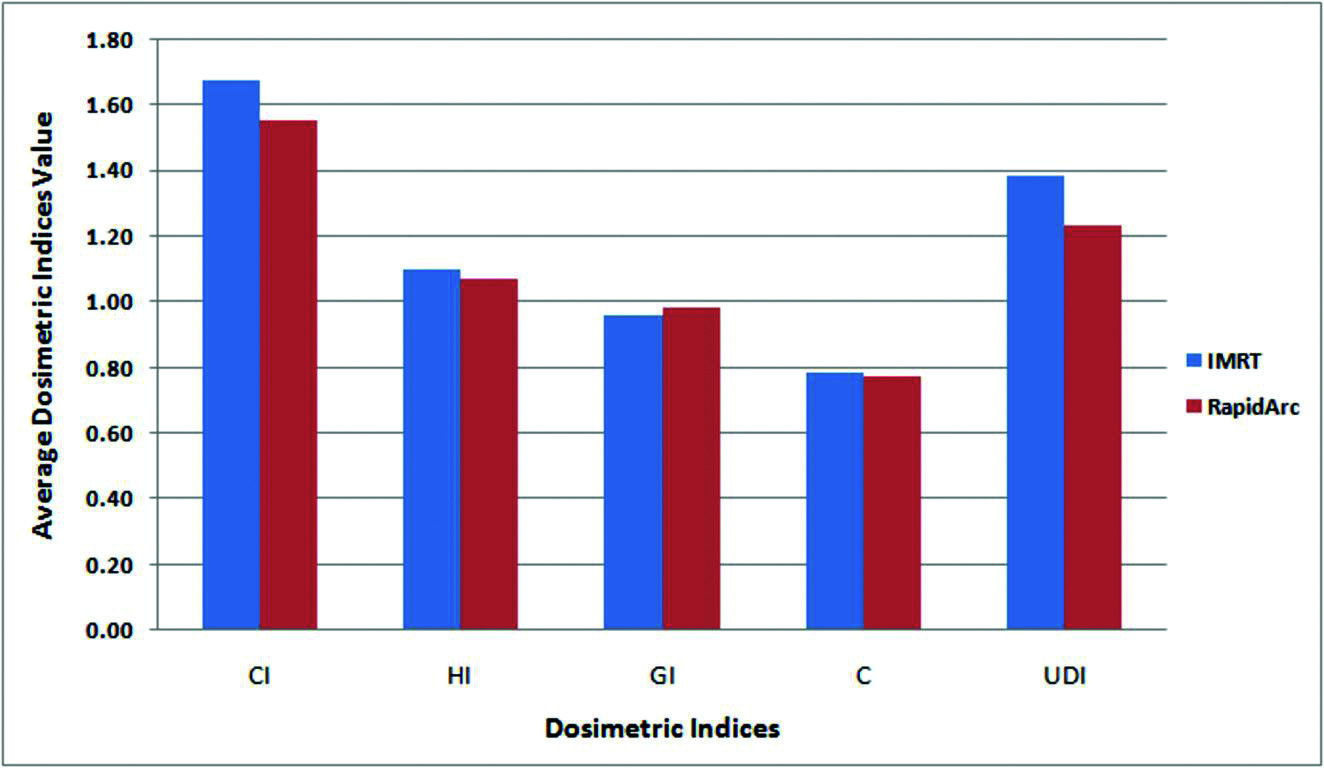
Comparable target coverage and better sparing of OARs were achieved with the RapidArc technique in comparison to IMRT. It was evident with results of present study, the values of CI (1.55±0.07), HI (1.07±0.07), GI (0.98±0.01) and UDI (1.25±0.11) of RapidArc technique showed significant difference from respective values of IMRT Technique (1.67±0.06, 1.10±0.06, 0.96±0.01 and 1.38±0.13). Values of MUs (1560.47±52.16) and treatment time (3.71±0.73 mins) were significantlly high in IMRT technique as compared to RapidArc technique (542.33±51.09 and 2.39±0.35 mins respectively).
Conclusion
From this study, it is clear that a similar planning goal can be achieved by RapidArc in comparison to fixed-field IMRT with less normal organ toxicity. RapidArc is a faster and precise treatment technique. The most significant change comes to see in the number of MUs and TT, which is much lesser in RapidArc.
Introduction
Cervical cancer is a widespread type of cancer all around the world [1-3]. Radiotherapy is the treatment of choice for definitive and postoperative management of cervical and endometrial cancer [4-7]. According to the staging of cancer, pelvic lymph node also include apart from the primary area. Due to this acute and late complications occur in genitourinary and gastrointestinal areas. The main principle of radiotherapy is providing a high dose to the tumour but as low as a reasonably achievable dose to the normal healthy organs to reduce long-term side-effects. Good tumour coverage can be achieved by normal conventional techniques but at the cost of higher OARs doses. Due to all these complications need for usage of advanced technology in treatment increased, these modern techniques can provide better target coverage and good sparing of OARs also. For these techniques, a plan quality can be analyzed by using many dosimetric indices. An ideal plan is defined as one with full uniform dose coverage, exactly conformed to the target, and stepwise fall off dose outside the target [8-11]. Akpati H et al., came with a new idea called a Unified Dosimetry Index (UDI) [12]. UDI scoring includes all four dosimetric indices such as coverage index (C), CI, HI, and dose GI. UDI scoring of every plan ranked and preferred the least scored plan as a better plan. Regarding the UDI, very little data is available for review.
The basic principle of IMRT is to radiate target from multiple directions to get a conformal dose to target and at the same time low dose to normal organs [13-16]. IMRT significantly reduces doses to bladder, bowel, and rectum in comparison to traditionally used techniques [17-21]. Fixed-field IMRT has a large beam-on time, due to this it takes a longer time to treat any patient. The number of MUs is also very large in IMRT techniques. The volumetric-arc therapy (VMAT or RapidArc) has capability to treat patients by gantry rotation in 360°. Limitations of IMRT plans can be easily overcome with arc technique and able to achieve more conformal dose in lesser time with lesser MUs. The primary algorithm of VMAT for planning and delivery was developed by Otto’s study [22]. RapidArc (Varian Medical System, Palo Alto, CA) allows continuous variation in gantry rotation speed, dose rate, and dynamic Multileaf Collimators (MLCs) during treatment [23]. These techniques can give single and multiple arcs with a variable dose rate [24]. Arc therapy has been applied for the various sites of the body like the prostate, oesophagus, cervix, and brain tumours [25,26]. Various studies suggested that better target coverage and better OARs are sparing in RapidArc [27].
This study utilised UDI scoring for evaluation and comparison of RapidArc and IMRT plans in the case of cervical cancer. The primary aim for this study was to investigate whether Eclipse Treatment Planning System (TPS) was capable of generating RapidArc plans with dose distributions that would have been clinically accepted if they had been generated by standard clinical IMRT.
Materials and Methods
This was the retrospective study done on data of 15 patients treated for cervical cancer at a tertiary care centre at Indraprastha Apollo Hospital, New Delhi. These patients were previously treated with sliding window IMRT techniques during January 2020 to November 2020.
Inclusion criteria: Data of patients of locally advanced carcinoma of the cervix with their International Federation of Gynaecology and Obstetrics (FIGO) stage IB-IIIB, who were earlier treated within the Department of Radiotherapy, Indraprastha Apollo Hospital, New Delhi during January 2020 to November 2020 on Novalis-Tx (Varian Linear Accelerator) with sliding window IMRT techniques were selected for this study [24].
Exclusion criteria: The patients beyond the FIGO staging range IB-IIIB were excluded from this study.
Patients were positioned with an immobilisation mask system. Continuous 3 mm Computed Tomography (CT) scans of the pelvis cancer patients were obtained with a spiral CT scanner (Siemens Biograph) in the supine position. Dose prescription to the PTV was 50.4 Gy in 28 fractions. The prescribed doses were given in 28 fractions (1.8 Gy/fraction), one fraction per day, and 5 fractions per week. Optimisation constraints for PTV and OARs were based on the Radiation Therapy and Oncology Group (RTOG) 0724 protocol [28].
Treatment Planning and Delivery
All techniques were generated by using Eclipse version 13 (Varian Medical Systems, Palo Alto, CA, USA) Treatment Planning System (TPS). The calculations were done with the High Definition (HD)-120 MLC. The plans were calculated with 6 MV photons. The number of fields was 9 for IMRT with 600 MU/min dose rate. For RapidArc, the triple arc (CW, CCW, and 90° CW) treatment field was split into 178 control points. The beam aperture was defined for each control point by MLC changes and gantry angle. The dose rate varied between 100 MU/min and a maximum of 600 MU/min. The algorithm used for planning purposes was Anisotropic Analytical Algorithm (AAA) [29-33]. During the RapidArc optimisation, the standard clinical IMRT objectives, in terms of target coverage and dose to OARs were used.
Plan Evaluation Parameters
Evaluation of plans was performed utilising standard Dose-Volume Histograms (DVHs). For PTV minimum, mean, and maximum doses were evaluated. According to the International Commission on Radiation Units and Measurements (ICRU) report 83 [34], D98% (minimum dose received by 98% of PTV volume) and D2% (maximum dose received by 2% of PTV volume) dose-volume parameters were evaluated for PTV. Apart from Dmax and Dmean, V40Gy parameters were also evaluated for rectum and bladder. For small bowel, Dmean and D200cc parameters were taken into considerations. Numbers of MUs and TT were also evaluated for patient comfort and long-term side-effects. Other calculated parameters were CI, HI, GI, coverage index (C), and UDI.
Statistical Analysis
Statistical Software Package for the Social Sciences (SPSS) version 20.0 (IBM Corporation, USA) was used for statistical analysis. Descriptive analysis was performed to determine the mean and Standard Deviation (SD) value of different dose-volume parameters of target, OARs and different dosimetric indices. A paired two-tailed t-test was performed to compare the IMRT technique with the RapidArc technique for radiotherapy treatment of cervical cancer patients. The p-value <0.05 was considered for the significance of statistical inferences.
Dose coverage is defined as 100% of the PTV receiving the prescribed dose. It gives a measure of how well the PTV is covered by the prescribed dose. A plan covered by 92% of prescribed dose is considered acceptable [35].
Coverage Index (C)=PTVPI/PTVWhere, PTVPI is the PTV receiving the Prescribed Isodose (PI).
The CI was first proposed in 1993 by RTOG and described in Report no. 62 of ICRU [36]. It is presented as a relation between the volume of the reference dose and target volume.
Conformity Index (CI)=VIR/TVWhere, VIR is the volume of reference dose and TV is the target volume.
According to the RTOG guidelines [37], ranges of CI values have been defined to determine the quality of conformation. Theoretically, 1 is an ideal value for CI. If the CI is situated between 1 and 2, the treatment is considered to comply with the treatment plan.
In 1993, RTOG proposed guidelines for routine evaluation of plans on several parameters and HI. The concept of HI was developed as an extension of the dosimetric analysis of the treatment plan.
Homogeneity Index (HI)=Imax/RIWhere, Imax is maximum isodose in the target, and RI is the reference isodose.
If the HI value is ≤2, treatment is considered to comply with the protocol, if this index is between 2 to 2.5, it is considered as a minor violation, but if the index exceeded 2.5, the violation of the protocol is considered to be major, but might nevertheless considered acceptable [38].
The dose GI can compare the plan of equal conformity but with different dose gradients. The quality of this dose gradient is quantified by GI. The dose GI is defined as the ratio of the volume receiving the PI line and the dose-volume receiving half of the PI line [39,40].
Dose gradient index (GI)=DVPI/DVHPIWhere, DVPI is the dose-volume of the PI; DVHPI is the dose volume of the half the prescribed dose.
The UDI consists of all four parameter that are described above [12]. It is a useful tool to decide on a perfect plan. For any perfect planning, all value of CI, HI, GI, and C should also be perfect. Change in any of the four components may change the value of UDI. UDI value close to 1 is desirable whereas a higher value of UDI is not desirable. Perfect planning have UDI value one [41]. All the four parameters have equal weightage in any planning so that UDI define as:
UDI=CI×C×HI×GIResults
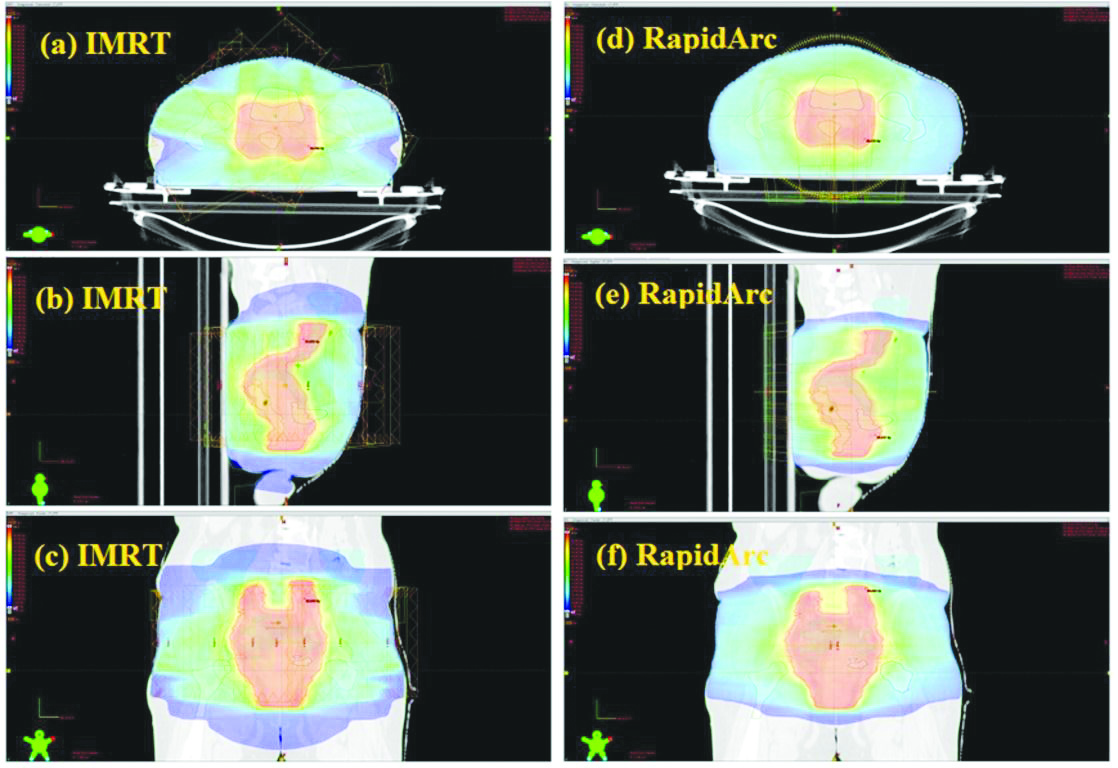
The colour wash of different doses in axial, coronal, and sagittal is shown in [Table/Fig-1]. From dose distribution, it can easily find out there is a dose reduction in the bladder and rectum in RapidArc plan. The same type of dose distribution was obtained for other patients also. Dosimetric assessments of both the treatment techniques are tabulated in [Table/Fig-2,3 and 4]. Doses to bladder, rectum, and small bowel were within the tolerance limit for both the plans as per recommended by RTOG guideline P0126 [42]. But from the [Table/Fig-2,3], it was clear that results were in favour of the RapidArc plan in respect to better OARs sparing at the cost of good PTV coverage as shown in [Table/Fig-5,6]. [Table/Fig-4] shows that number of MUs used by the IMRT plan was three times higher than Rapid plan (1560.47±52.16 for IMRT and 542.33±51.09 for RapidArc). Due to this, overall TT significantly increased for the IMRT plan, which was around 1.5 times higher than the RapidArc plan (3.71±0.73 for IMRT and 2.39±0.35 for RapidArc) [Table/Fig-7]. In the present study, a plan quality analyses by using different dosimetric indexes like HI, CI, ID, C, and UDI. The mean value of CI, HI, GI, and C for RapidArc plan were 1.55±0.07, 1.07±0.07, 0.98±0.01, and 0.78±0.03, respectively. The same index values for the IMRT plan were 1.67±0.06, 1.10±0.06, 0.96±0.01, and 0.78±0.04, respectively [Table/Fig-4]. From the above value of CI, HI, GI, and C it is clear that RapidArc plans are better in all the parameters [Table/Fig-8]. In Results of this UDI scoring are also in favour RapidArc plan (1.25±0.11 for RapidArc plans and 1.38±0.13 for IMRT plans).
Illustration of dose distribution for radiotherapy treatment of an example cervical cancer patient using nine fields IMRT (left side) in (a) axial view, (b) sagittal view, and (c) coronal view and similar CT cut planned by triple arc RapidArc technique (right side) in (d) axial view, (e) sagittal view, and (f) coronal view.
Dose values of Planning Target Volume (PTV) with their significance level in comparison of intensity-modulated radiotherapy (IMRT) technique with RapidArc technique.
| PTV parameters | Techniques | p-value (Paired t-test) |
|---|
| IMRT (Mean±SD) | RapidArc (Mean±SD) |
|---|
| Dmax (Gy) | 53.93±0.93 | 52.68±0.98 | <0.001 |
| Dmin (Gy) | 36.55±3.54 | 38.20±3.48 | <0.001 |
| Dmean (Gy) | 49.75±0.48 | 49.83±0.60 | 0.327 |
Dmax: Maximum dose; Dmin: Minimum dose; Dmean: Mean Dose
Dose values of Organs at risk (OARs) with their significance level in comparison of intensity-modulated radiotherapy (IMRT) technique with RapidArc technique [42].
| Organs at risk (OARs) | Parameters | Techniques | p-value (Paired t-test) |
|---|
| IMRT (Mean±SD) | RapidArc (Mean±SD |
|---|
| Rectum | Dmax (Gy) | 52.78±1.02 | 51.45±0.76 | <0.001 |
| Dmean (Gy) | 38.81±1.67 | 37.60±1.51 | 0.025 |
| V40Gy (%) | 34.71±2.15 | 33.50±1.91 | <0.001 |
| Bladder | Dmax (Gy) | 53.01±0.70 | 52.43±0.74 | 0.005 |
| Dmean (Gy) | 37.60±1.51 | 36.61±1.64 | <0.001 |
| V40Gy (%) | 52.43±0.74 | 28.67±3.21 | <0.001 |
| Small bowel | Dmean(Gy) | 22.58±2.58 | 21.54±1.96 | 0.002 |
| D200cc (Gy) | 40.44±3.35 | 39.13±3.25 | <0.001 |
p-value <0.05 considered significant
Treatment time, number of monitor units (MUs), and dosimetric indices with their statistical significance level in comparison of intensity-modulated radiotherapy (IMRT) technique with RapidArc technique.
| Parameters | Treatment techniques | p-value (Paired t-test) |
|---|
| IMRT (Mean±SD) | RapidArc (Mean±SD) |
|---|
| Treatment Time (min.) | 3.71±0.73 | 2.39±0.35 | <0.001 |
| Number of Monitor Units (MUs) | 1560.47±52.16 | 542.33±51.09 | <0.001 |
| Conformity Index (CI) | 1.67±0.06 | 1.55±0.07 | <0.001 |
| Homogeneity Index (HI) | 1.10±0.06 | 1.07±0.07 | <0.001 |
| Dose Gradient Index (GI) | 0.96±0.01 | 0.98±0.01 | <0.001 |
| Coverage Index (C) | 0.78±0.04 | 0.78±0.03 | 0.234 |
| Unified Dosimetry Index (UDI) | 1.38±0.13 | 1.25±0.11 | <0.001 |
p-value <0.05 considered significant
Illustration of PTV dosimetric parameters for IMRT and RapidArc treatment technique.
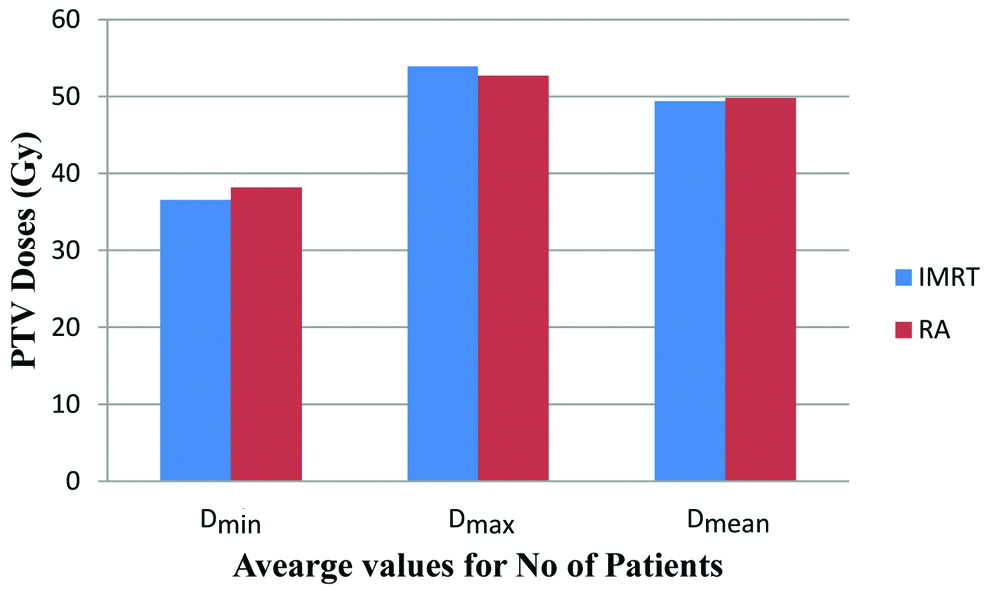
Illustration of different dosimetric parameters for Rectum (a), Bladder (b) and Small Bowel (c) between IMRT and RapidArc treatment technique.
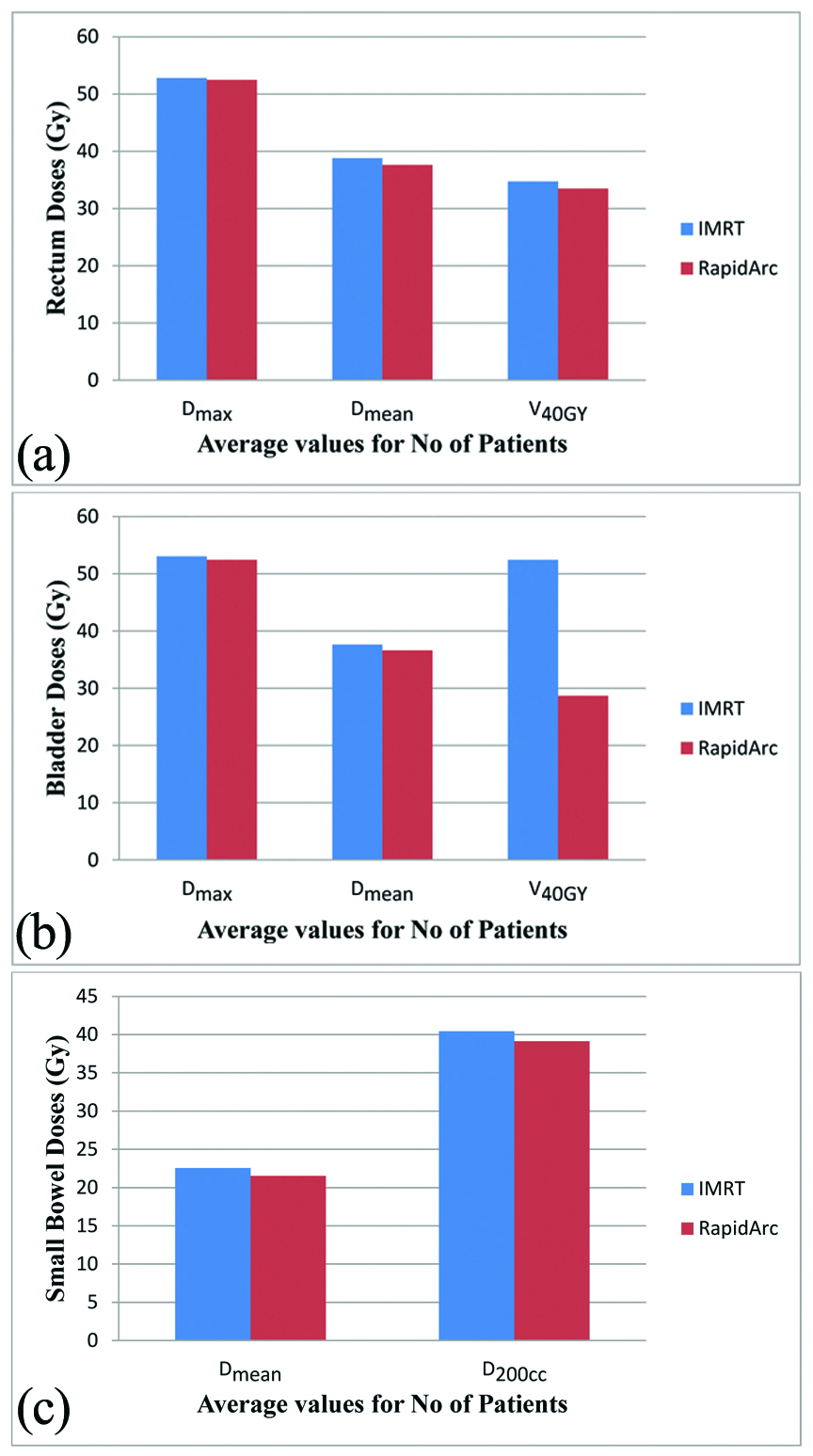
Illustration of treatment time (a) and number of monitor Units (b) comparison between IMRT and RapidArc plans.
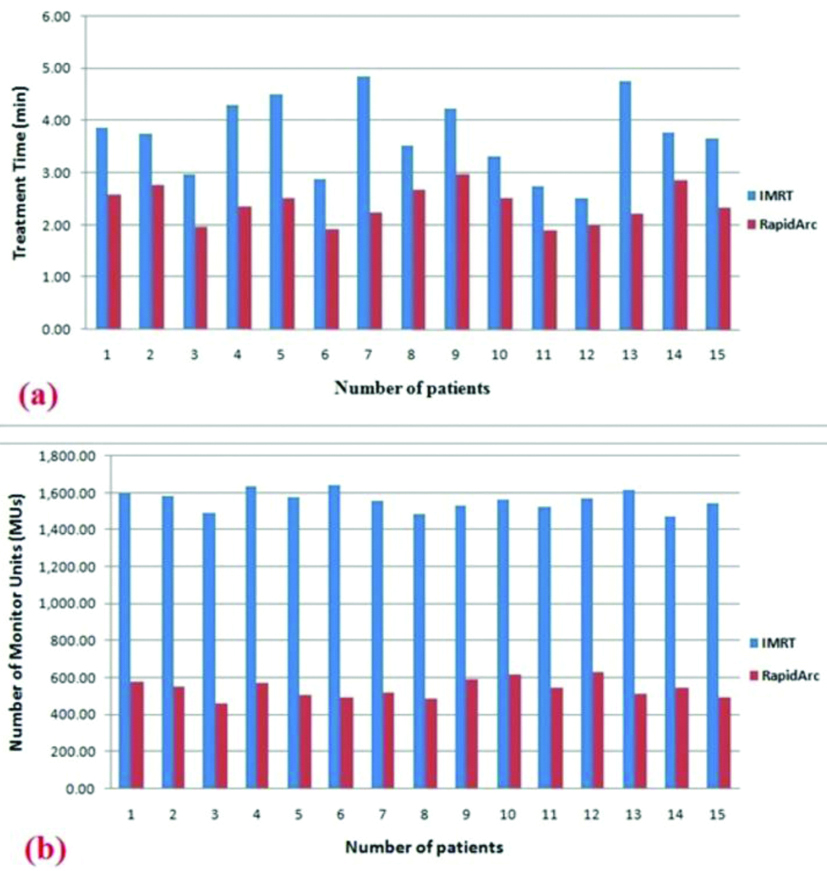
Illustration of dosimetric indices comparison between IMRT and RapidArc plans.
Discussion
RapidArc therapy trial gives a large degree of freedom by providing many control points (178) for dynamic dose delivery during gantry rotation. In comparison to RapidArc, IMRT plans provide dose delivery only at fixed beam angles only. Due to this, IMRT plans may skip some best possible beam angles during dose delivery. This type of problem can be easily overcome by using RapidArc [42]. Many supporting studies have been provided their results in favour of fixed-field IMRT in comparison to conventional planning techniques [17-21]. Oliver M et al., and Nicolini G et al., studies show that at the same PTV coverage, RapidArc can generate a plan with better homogeneity and conformity [43,44]. There is a significant reduction in doses for rectum, small bowel, and bladder.
RapidArc uses all feasible angles for optimisation to generate the best possible plan at a prescribed dose to PTV and doses to OARs accordingly [45]. An extra arc can be easily used for complex and large target volume like gynecological tumours because the numbers of MUs and TT significantly increased if authors used IMRT techniques for the same type of patients. In such a case, a RapidArc technique is a better alternative than fixed-field IMRT techniques. GI is also improved with the RapidArc plan which shows dose fall off. UDI scoring is a good technique for comparing multiple plans. It can help in deciding a better plan in respect of many parameters. A lower value of UDI shows a better plan. Results show that both the techniques can generate clinically acceptable plan but RapidArc gives better values compared to IMRT techniques.
Limitation(s)
This dosimetric study was retrospective in nature and performed with only fifteen patients of cervical cancer.
Conclusion(s)
A RapidArc technique shows better target coverage, homogeneity, and conformity in comparison with fixed-field IMRT techniques. There is a sharper dose fall-off for the RapidArc plan with a comparative dose to surrounding organs like bowel rectum and bladder. These all parameters combined and give better UDI scoring in favour of RapidArc. The potential benefit of Rapid Arc in respect of patient comfort is shorter TT and in long-term side-effect is lesser MUs. This study shows that a RapidArc can be an alternative where it’s required in favour of patient comfort as well as clinically benefit also. A prospective study should be performed with larger data set to validate the recommendations of this study.
Dmax: Maximum dose; Dmin: Minimum dose; Dmean: Mean Dose
p-value <0.05 considered significant
p-value <0.05 considered significant
[1]. Jemal A, Siegel R, Xu J, Ward E, Cancer statistics, 2010CA Cancer J Clin 2010 60:277-300.10.3322/caac.2007320610543 [Google Scholar] [CrossRef] [PubMed]
[2]. Kim JH, Choi JH, Ki EY, Lee SJ, Yoon JH, Lee KH, Incidence and risk factors of lower-extremity lymphedema after radical surgery with or without adjuvant radiotherapy in patients with FIGO stage I to stage IIA cervical cancerInt J Gynecol Cancer 2012 22(4):686-91.10.1097/IGC.0b013e318246695022398707 [Google Scholar] [CrossRef] [PubMed]
[3]. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM, Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer 2010 127(12):2893-917.10.1002/ijc.2551621351269 [Google Scholar] [CrossRef] [PubMed]
[4]. Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Wárlám-Rodenhuis CC, Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial CarcinomaLancet 2000 355(9213):1404-11.10.1016/S0140-6736(00)02139-5 [Google Scholar] [CrossRef]
[5]. Green JA, Kirwan JM, Tierney JF, Symonds P, Fresco L, Collingwood M, Survival and recurrence after concomitant chemotherapy and radiotherapy for cancer of the uterine cervix: A systematic review and meta-analysisLancet 2001 358(9284):781-86.10.1016/S0140-6736(01)05965-7 [Google Scholar] [CrossRef]
[6]. Grigsby PW, Update on radiation therapy for endometrial cancerOncology (Williston Park) 2002 16:777-95. [Google Scholar]
[7]. Lukka H, Hirte H, Fyles A, Thomas G, Elit L, Johnston M, Concurrent cisplatin-based chemotherapy plus radiotherapy for cervical cancer-A meta-analysisClin Oncol (R Coll Radiol) 2002 14(3):203-12.10.1053/clon.2002.007612109823 [Google Scholar] [CrossRef] [PubMed]
[8]. Wagner TH, Bova FJ, Friedman WA, Buatti JM, Bouchet LG, Meeks SL, A simple and reliable index for scoring rival stereotactic radiosurgery plansInt J Radiat Oncol Biol Phys 2003 57(4):1141-49.10.1016/S0360-3016(03)01563-3 [Google Scholar] [CrossRef]
[9]. van’t Riet A, Mak AC, Moerland MA, Elders LH, van der Zee W, A conformation number to quantify the degree of conformality in brachytherapy and external beam irradiation: Application to the prostateInt J Radiat Oncol Biol Phys 1997 37(3):731-36.10.1016/S0360-3016(96)00601-3 [Google Scholar] [CrossRef]
[10]. Paddick I, A simple scoring ratio to index the conformity of radiosurgical treatment plans. Technical noteJ Neurosurg 2000 93(Suppl 3):219-22.10.3171/jns.2000.93.supplement_3.021911143252 [Google Scholar] [CrossRef] [PubMed]
[11]. Baltas D, Kolotas C, Geramani K, Mould RF, Ioannidis G, Kekchidi M, A Conformal Index (COIN) to evaluate implant quality and dose specification in brachytherapyInt J Radiat Oncol Biol Phys 1998 40(2):515-24.10.1016/S0360-3016(97)00732-3 [Google Scholar] [CrossRef]
[12]. Akpati H, Kim C, Kim B, Park T, Meek A, Unified dosimetry index (UDI): A figure of merit for ranking treatment plansJ Appl Clin Med Phys 2008 9(3):280310.1120/jacmp.v9i3.280318716596 [Google Scholar] [CrossRef] [PubMed]
[13]. Ahmed RS, Kim RY, Duan J, Meleth S, De Los Santos JF, Fiveash JB, IMRT dose escalation for positive para-aortic lymph nodes in patients with locally advanced cervical cancer while reducing dose to bone marrow and other organs at riskInt J Radiat Oncol Biol Phys 2004 60(2):505-12.10.1016/j.ijrobp.2004.03.03515380585 [Google Scholar] [CrossRef] [PubMed]
[14]. Duthoy W, De Gersem W, Vergote K, Boterberg T, Derie C, Smeets P, Clinical implementation of intensity-modulated arc therapy (IMAT) for rectal cancerInt J Radiat Oncol Biol Phys 2004 60(3):794-806.10.1016/j.ijrobp.2004.04.01615465196 [Google Scholar] [CrossRef] [PubMed]
[15]. Duthoy W, De Gersem W, Vergote K, Coghe M, Boterberg T, De Deene Y, Whole abdominopelvic radiotherapy (WAPRT) using intensity-modulated arc therapy (IMAT): First clinical experienceInt J Radiat Oncol Biol Phys 2003 57(4):1019-32.10.1016/S0360-3016(03)00663-1 [Google Scholar] [CrossRef]
[16]. Georg P, Georg D, Hillbrand M, Kirisits C, Pötter R, Factors influencing bowel sparing in intensity modulated whole pelvic radiotherapy for gynaecological malignanciesRadiother Oncol 2006 80(1):19-26.10.1016/j.radonc.2006.04.01416766068 [Google Scholar] [CrossRef] [PubMed]
[17]. Guckenberger M, Baier K, Richter A, Vordermark D, Flentje M, Does intensity modulated radiation therapy (IMRT) prevent additional toxicity of treating the pelvic lymph nodes compared to treatment of the prostate only?Radiat Oncol 2008 3:310.1186/1748-717X-3-318190681 [Google Scholar] [CrossRef] [PubMed]
[18]. Mundt AJ, Lujan AE, Rotmensch J, Waggoner SE, Yamada SD, Fleming G, Intensity-modulated whole pelvic radiotherapy in women with gynecologic malignanciesInt J Radiat Oncol Biol Phys 2002 52(5):1330-37.10.1016/S0360-3016(01)02785-7 [Google Scholar] [CrossRef]
[19]. Portelance L, Chao KS, Grigsby PW, Bennet H, Low D, Intensity-modulated radiation therapy (IMRT) reduces small bowel, rectum, and bladder doses in patients with cervical cancer receiving pelvic and para-aortic irradiationInt J Radiat Oncol Biol Phys 2001 51(1):261-66.10.1016/S0360-3016(01)01664-9 [Google Scholar] [CrossRef]
[20]. Roeske JC, Lujan A, Rotmensch J, Waggoner SE, Yamada D, Mundt AJ, Intensity-modulated whole pelvic radiation therapy in patients with gynecologic malignanciesInt J Radiat Oncol Biol Phys 2000 48(5):1613-21.10.1016/S0360-3016(00)00771-9 [Google Scholar] [CrossRef]
[21]. Wong E, D’Souza DP, Chen JZ, Lock M, Rodrigues G, Coad T, Intensity-modulated arc therapy for treatment of high-risk endometrial malignanciesInt J Radiat Oncol Biol Phys 2005 61(3):830-41.10.1016/j.ijrobp.2004.06.25315708263 [Google Scholar] [CrossRef] [PubMed]
[22]. Otto K, Volumetric modulated arc therapy: IMRT in a single gantry arcMed Phys 2008 35(1):310-17.10.1118/1.281873818293586 [Google Scholar] [CrossRef] [PubMed]
[23]. Teoh M, Clark CH, Wood K, Whitaker S, Nisbet A, Volumetric modulated arc therapy: A review of current literature and clinical use in practiceBr J Radiol 2011 84(1007):967-96.10.1259/bjr/2237334622011829 [Google Scholar] [CrossRef] [PubMed]
[24]. Ashamalla H, Tejwani A, Parameritis I, Swamy U, Luo PC, Guirguis A, Comparison study of intensity modulated arc therapy using single or multiple arcs to intensity modulated radiation therapy for high-risk prostate cancerRadiat Oncol J 2013 31(2):104-10.10.3857/roj.2013.31.2.10423865007 [Google Scholar] [CrossRef] [PubMed]
[25]. Mayo CS, Ding L, Addesa A, Kadish S, Fitzgerald TJ, Moser R, Initial experience with volumetric IMRT (RapidArc) for intracranial stereotactic radiosurgeryInt J Radiat Oncol Biol Phys 2010 78(5):1457-66.10.1016/j.ijrobp.2009.10.00520207494 [Google Scholar] [CrossRef] [PubMed]
[26]. Yin L, Wu H, Gong J, Geng JH, Jiang F, Shi AH, Volumetric-modulated arc therapy vs. c-IMRT in esophageal cancer: A treatment planning comparisonWorld J Gastroenterol 2012 18(37):5266-75. [Google Scholar]
[27]. Cozzi L, Dinshaw KA, Shrivastava SK, Mahantshetty U, Engineer R, Deshpande DD, A treatment planning study comparing volumetric arc modulation with RapidArc and fixed field IMRT for cervix uteri radiotherapyRadiother Oncol 2008 89(2):180-91.10.1016/j.radonc.2008.06.01318692929 [Google Scholar] [CrossRef] [PubMed]
[28]. Chemotherapy and pelvic radiation therapy with or without additional chemotherapy in treating patients with high-risk early-stage cervical cancer after radical hysterectomy. Available from: https://clinicaltrials.gov/ct2/show/NCT00980954 [Google Scholar]
[29]. Bragg CM, Wingate K, Conway J, Clinical implications of the anisotropic analytical algorithm for IMRT treatment planning and verificationRadiother Oncol 2008 86:276-84.10.1186/1748-717X-8-16423826854 [Google Scholar] [CrossRef] [PubMed]
[30]. Fogliata A, Vanetti E, Albers D, Brink C, Clivio A, Knöös T, On the dosimetric behaviour of photon dose calculation algorithms in the presence of simple geometric heterogeneities: Comparison with Monte Carlo calculationsPhys Med Biol 2007 52(5):1363-85.10.1088/0031-9155/52/5/01117301460 [Google Scholar] [CrossRef] [PubMed]
[31]. Knöös T, Wieslander E, Cozzi L, Brink C, Fogliata A, Albers D, Comparison of dose calculation algorithms for treatment planning in external photon beam therapy for clinical situationsPhys Med Biol 2006 51(22):5785-807.10.1088/0031-9155/51/22/00517068365 [Google Scholar] [CrossRef] [PubMed]
[32]. Roeske JC, Mundt AJ, Halpern H, Sweeney P, Sutton H, Powers C, Late rectal sequelae following definitive radiation therapy for carcinoma of the uterine cervix: A dosimetric analysisInt J Radiat Oncol Biol Phys 1997 37(2):351-58.10.1016/S0360-3016(96)00490-7 [Google Scholar] [CrossRef]
[33]. Ulmer W, Pyyry J, Kaissl W, A 3D photon superposition/convolution algorithm and its foundation on results of Monte Carlo calculationsPhys Med Biol 2005 50(8):1767-90.10.1088/0031-9155/50/8/01015815095 [Google Scholar] [CrossRef] [PubMed]
[34]. International Commission on Radiation Units and MeasurementsPrescribing, Recording, and Reporting Photon-Beam Intensity-Modulated Radiation Therapy (IMRT). ICRU Report 83Journal of ICRU 2010 10(1)Page NP10.1093/jicru/ndq002 [Google Scholar] [CrossRef]
[35]. Krishna GS, Srinivas V, Ayyangar KM, Reddy PY, Comparative study of old and new versions of treatment planning system using dose volume histogram indices of clinical plansJ Med Phys 2016 41(3):192-97.10.4103/0971-6203.18948927651566 [Google Scholar] [CrossRef] [PubMed]
[36]. International Commission on Radiation Units and MeasurementsPrescribing, Recording, and Reporting Photon-Beam Therapy (Supplement to ICRU 50). ICRU Report 62Journal of ICRU 1999 [Google Scholar]
[37]. Small W, Bosch WR, Harkenrider MM, Yashar CM, Winter KA, Gaffney DK, NRG Oncology/RTOG Consensus guidelines for delineation of clinical target volume for intensity modulated pelvic radiation therapy in postoperative treatment of endometrial and cervical cancer: An updateInternational Journal of Radiation Oncology, Biology, Physics 2021 109(2):413-24.10.1016/j.ijrobp.2020.08.06132905846 [Google Scholar] [CrossRef] [PubMed]
[38]. Kataria T, Sharma K, Subramani V, Karrthick KP, Bisht SS, Homogeneity Index: An objective tool for assessment of conformal radiation treatmentsJ Med Phys 2012 37(4):207-13.10.4103/0971-6203.10360623293452 [Google Scholar] [CrossRef] [PubMed]
[39]. Krishnan J, Shetty J, Rao S, Hegde S, Shambhavi C, Comparison of rapid arc and intensity-modulated radiotherapy plans using unified dosimetry index and the impact of conformity index on unified dosimetry index evaluationJ Med Phys 2017 42(2):14-17.10.4103/jmp.JMP_112_1628405103 [Google Scholar] [CrossRef] [PubMed]
[40]. Paddick I, Lippitz B, A simple dose gradient measurement tool to complement the conformity indexJ Neurosurg 2006 105:194-201.10.3171/sup.2006.105.7.19418503356 [Google Scholar] [CrossRef] [PubMed]
[41]. Calvo-Ortega JF, Delgado D, Moragues S, Pozo M, Casals J, Dosimetric comparison of intensity modulated radiosurgery with dynamic conformal arc radiosurgery for small cranial lesionsJ Can Res Ther 2016 12:852-57.10.1186/1748-717X-4-2719630947 [Google Scholar] [CrossRef] [PubMed]
[42]. Michalski JM, Moughan J, Purdy JA, Bosch W, Bahary JP, Lau H, Initial results of a phase III randomized study of high-dose 3DCRT/IMRT versus standard dose 3D-CRT/IMRT in patients treated for localized prostate cancer (RTOG 0126)Int J Radiat Oncol Biol Phys 2014 90(5):126310.1016/j.ijrobp.2014.10.035 [Google Scholar] [CrossRef]
[43]. Oliver M, Ansbacher W, Beckham WA, Comparing planning time, delivery time and plan quality for IMRT, RapidArc and TomotherapyJ Appl Clin Med Phys 2009 10(4):306810.1120/jacmp.v10i4.306819918236 [Google Scholar] [CrossRef] [PubMed]
[44]. Nicolini G, Clivio A, Fogliata A, Vanetti E, Cozzi L, Simultaneous integrated boost radiotherapy for bilateral breast: A treatment planning and dosimetric comparison for volumetric modulated arc and fixed field intensity modulated therapyRadiat Oncol 2009 4:2710.1186/1748-717X-4-2719630947 [Google Scholar] [CrossRef] [PubMed]
[45]. Sharma MK, Mitra S, Saxena U, Bhushan M, Shrivastava H, Simson DK, Is volumetric modulated arc therapy (RapidArc) better than intensity modulated radiotherapy for gynecological malignancies? A dosimetric comparisonJ Cancer Res Ther 2014 10(4):883-88.10.4103/0973-1482.13820825579523 [Google Scholar] [CrossRef] [PubMed]