Sexual dimorphism is a combined result of genetic factors (e.g., hormone levels) and the environment (e.g., nutrition and cultural behaviours) [1]. In order to understand the causes and effects of prenatal environment in-utero, scientists required a “window” into uterine conditions. From the evolutionary and clinical standpoint, the hand is one such organ of the human body [2]. A number of researchers [3-5] have thus suggested that second to fourth digit length ratio (2D:4D) might be a marker of pre-natal androgen concentration in-utero. Higher concentration of pre-natal testosterone (in relation to oestrogen) may be indicated by longer ring (fourth) finger than index (second) finger and is defined as low digit ratio. In contrast, a high 2D:4D ratio potentially indicates a greater early oestrogen exposure. If variation in 2D:4D ratio is a phenotypic proxy for intrauterine sex steroid hormone exposure of the individual, then digit length ratio may predict correlations between 2D:4D and those diseases which follow sexually dimorphic patterns [6]. Chen H et al., has already established that phenotypic male sex to be associated with longer axial length of eyeball [7]. In other words, male sex hormones can affect the overall growth of the eyeball. There is also corroborative evidence [8-10] that suggests sex hormones having influence on ocular tissues. As 2D:4D ratio is an anthropometric window into the interplay of sex hormones in-utero, this tool may be tested to note if there is any correlation between the sexual dimorphism of axial length and the digit length ratio. Hence, population-specific database of measurements are most useful for reference.
Most of the studies on digit ratio have been conducted in other parts of the world, like Australia and America etc., [11,12] but in India research and documentation is scanty. In India only a single extensive study with 1500 subjects from central India is available [13] for determining the 2D:4D ratio in both the sexes. Generation of data of 2D:4D length ratio of the sample population can serve as reference for further research work, in Eastern India. Hence, this study aimed to fill in the lacuna that exists for a corroborative data in the eastern part of India, and the correlation of 2D:4D ratio and with various anthropometric parameters like height, BMI and ocular axial length. This study was a novel attempt to find out if 2D:4D ratio correlates with ocular axial length.
Materials and Methods
This cross-sectional study with simple random sampling was conducted in the Departments of Anatomy and Ophthalmology OPD of a tertiary care hospital and Medical College in West Bengal, India from March 2016 to February 2017. All the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (Approved by the Institutional Ethics Committee of the Burdwan Medical College, Burdwan-713104, West Bengal India, vide Memo No. BMC/PG/4417 Dated 14/12/2015) and with the Helsinki Declaration of 1975 that was revised in 2013.
Sample size calculation: Sample size was calculated with the help of online sample size calculator (http://www.raosoft.com/samplesize.html). Here confidence interval was set at 95%; and the acceptable margin of error was set between 4-5 percent. Hence, a sample size of 500 was obtained.
Inclusion criteria: Adult patients (≥20 years of age), with no physical deformity and having a sound mental condition, who would voluntarily cooperate with the examiner during various types of physical and ophthalmological assessments requiring attention span (like Ultrasonography (USG) Scan biometry, attended the ophthalmology OPD of the centre during the study time period and were willing to participate in the study by giving written consent were included in the study.
Exclusion criteria: Patients with history of ocular surgery, neurological disease/disorder, long term medications and ocular pathologies like glaucoma and cataract, or those having arthritis or finger injury or who were physically handicapped and/or mentally challenged (as determined by past medical records/history) were excluded from the study.
Written consent for participation in this study was taken in the language they preferred. A proforma outlining the following items: identity, history of present illness, past medical or surgical history and history of any chronic medication known to have oculotoxic or neurotoxic side-effects was filled out for each patient. A general physical survey was also done. The history and physical survey were primarily based on the set inclusion and exclusion criteria. The patients were asked to place both hands on a firm wooden table, with palm facing upwards and remove jewellery worn on fingers, if any. Length of index finger (2nd digit=2D) and ring finger (4th digit=4D) of both left and right hands, on the ventral surface were measured, from the metacarpophalangeal crease to tip of the finger, using digital Vernier callipers ([Table/Fig-1] Zhart Digital Vernier Caliper, manufactured by Zhart India with measuring range, 0-150 mm) and values were recorded.
Digital Vernier Caliper taking measurement.

When there was more than one crease at the base of the digit, the most proximal crease was considered. The digit length ratio (2D:4D) was calculated by dividing length of index finger by length of ring finger. Then the patient was instructed to stand against the stadiometer (Prestige Height Measuring Scale for Adults and Children New Style Stadiometer) with measurement range of 20-210 cm, model no. Prestige-SM Manufactured by Hardik meditech, India.
The patient’s height was measured and recorded. Measurement was taken from the heels to the top of head, after subject stood erect and removed his/her shoes and socks. The patient was then asked to stand on the portable weighing machine (Alpha Digital Weighing Scale SRS400, Alphascale India.,) to record patient’s weight. BMI was calculated using appropriate formula [weight (in kilograms)/height2 (in meters)].
Each of the physical parameters were recorded independently by two authors (same pair each time) and the mean value was finally noted. The investigators had more than ten years of experience as anatomists, proficient in taking anatomical and anthropological data.
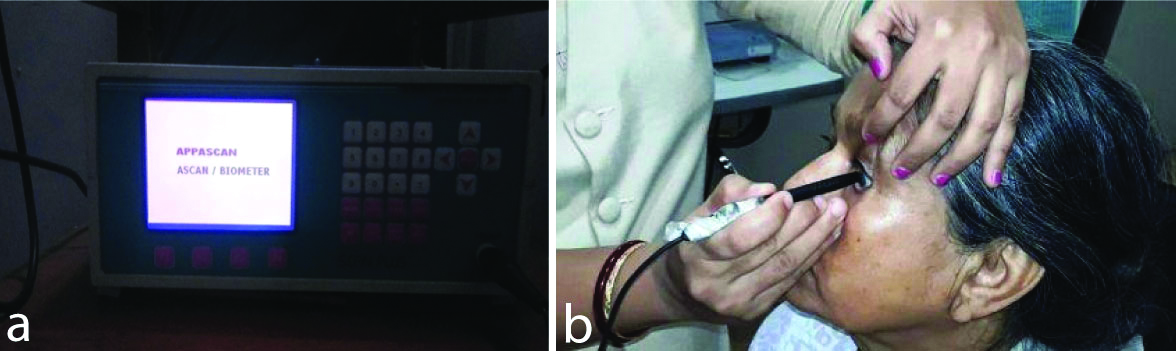
Then the Axial Length of eyeball (AL) was measured by an Ophthalmologist using A-scan biometry ultrasonography. Appascan Scan Plus AME-01A machine manufactured by Appasamy Associates, India, [Table/Fig-2a,b] with a sound velocity of 1550 m/s was used for all the patients, and six consecutive measurements (three recordings each were taken by the two ophthalmologist co-authors, having more than ten years of expertise in the subject and the mean value was recorded) were done by the manual direct contact technique.
a) Scan Biometry Machine; b) Showing measurement of axial length of eyeball using A-Scan biometry machine.
Statistical Analysis
All collected data were arranged in proper manner and analysed by appropriate statistical method on computer using windows excel sheet and SPSS version 16.0. A descriptive analysis was used for mean values during analysis. Unpaired t-test was used for determining possible group differences in 2D:4D length ratios. Pearson’s correlation coefficients were used for assessing the relationship between two variables. Significance level was set at p<0.05 with 95% confidence interval.
Results
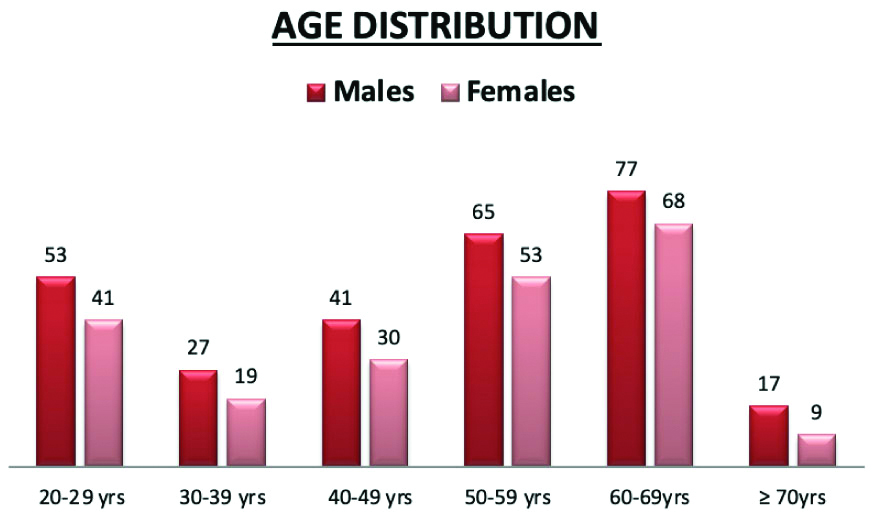
In the study population, 56% were males and 44% were females, (280 males and 220 females). [Table/Fig-3] showed that out of the 280 males of the study population, majority of them belonged to 60-69 years group (27.5%), followed by 50-59 years group (23.2%), and 20-29 years (18.9%). Similarly, out of the 220 females, majority belonged to age group 60-69 years (30.9%), followed by 50-59 years group (24.1%) and 20-29 years (18.6%). Mean age for males was 49.42 years and for females was 49.75 years.
Distribution of the males and females of the study population according to age groups.
From [Table/Fig-4] it can be seen that in males, the mean right hand 2D:4D ratio was 0.89±0.04 and for the left hand the mean 2D:4D ratio was 0.946±0.042. In females, the mean right hand 2D:4D ratio was 0.993±0.02 and the mean left hand 2D:4D ratio was 0.999±0.04. The figure shows that in males and females the 2D:4D digit length ratio is significantly different. Males had significantly lower value of 2D:4D ratio as compared to females both for the right as well as the left hands p<0.001.
Mean and Standard Deviations (SD) for digit length ratios (2D:4D) of right and left hands of the males (n=280) and females (n=220) of the study population.
| 2D:4D | Males Mean±SD | Females Mean±SD | t value (Unpaired t-test) | Standard error of difference | p-value |
|---|
| Right hand | 0.89±0.04 | 0.993±0.02 | 34.91 | 0.003 | <0.001** |
| Left hand | 0.964±0.042 | 0.999±0.04 | 14.30 | 0.004 | <0.001** |
**denotes highly significant values
In [Table/Fig-5] it is seen that, correlation of 2D:4D length ratio of right and left hands on height of males revealed moderate amount of significant negative correlation: (Right hand: r=-0.679, p<0.001; Left hand: r=-0.463, p<0.001). On the other hand, in females pearsons’s correlation coefficient, r for 2D:4D length ratios of right and left hands upon height were weakly positive but statistically significant. (Right hand: r=0.313, p<0.001; left hand: r=0.21, p<0.05).
The correlation between 2D:4D right hand and 2D:4D left hand with height (in meters) in males and females of the study population, using Pearson’s correlation coefficient (r), p-value significant at <0.05.
| Height | Males (n=280) | Females (n=220) |
|---|
| r | p | r | p |
|---|
| Right hand 2D:4D | -0.679 | <0.001** | 0.313 | <0.001** |
| Left hand 2D:4D | -0.463 | <0.001** | 0.210 | <0.05* |
**denotes highly significant values; *denotes significant p-values
Pearson’s Correlation [Table/Fig-6] of 2D:4D length ratio of right hand on BMI of males showed weak positive correlation (r=0.18), and the result was significant (p<0.05); for left hand also there was weak positive correlation (r=0.137) and significant p-value <0.05). In case of females, right and left hand 2D:4D correlated on BMI showed weakly negative correlation for both hands, but the values were not significant [Table/Fig-6].
The correlation between 2D:4D right hand and 2D:4D left hand with BMI (in Kg/meters2) in males and females of the study population, using Pearson’s correlation coefficient (r), p-value significant at <0.05.
| BMI | Males (n=280) | Females (n=220) |
|---|
| r | p | r | p |
|---|
| Right hand 2D:4D | 0.18 | <0.05* | -0.068 | >0.05 |
| Left hand 2D:4D | 0.137 | <0.05* | -0.073 | >0.05 |
The difference between the male and female mean axial length of eyeballs was tested using unpaired t-test. It revealed that the two-tailed p-value was <0.001, by conventional criteria, this difference is considered to be extremely statistically significant [Table/Fig-7].
Showing the results of unpaired t-test used to test the difference between the male and female mean Axial Length (AL) of eyeballs (in mm), where, n is sample size, SD is standard deviation, p-value significant at <0.05.
| Gender | Axial length (mm) | t-test | p-value | Degrees of freedom | Standard error of difference |
|---|
| Male (n=280) | 23.28±0.601 | 15.04 | <0.001** | 498 | 0.084 |
| Female (n=220) | 22.02±1.23 |
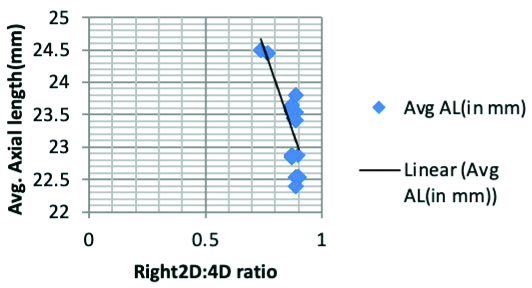
From [Table/Fig-8,9,10], it can be seen that, when 2D:4D length ratio of right and left hands are correlated with average axial length of eyeball in males, results revealed moderately negative significant correlation for the right hand and weakly negative but significant correlation for the left hand (right hand: r=-0.706, p<0.001; left hand: r=-0.25, p<0.05) that means, with increase in axial length of eyeball in males, there was a decrease in the 2D:4D digit ratio of both left and right hands.
The correlation between 2D:4D right hand and 2D:4D left hand with Average axial length of eyeball (in millimetres) in males and females of the study population, using Pearson’s correlation coefficient (r), p-value significant at <0.05.
| Average Axial length of eyeball (in millimetre) | Male (n=280) | Female (n=220) |
|---|
| r | p | r | p |
|---|
| Right hand 2D:4D | -0.706 | <0.001** | 0.145 | <0.05* |
| Left hand 2D:4D | -0.25 | <0.05* | 0.087 | >0.05 |
**denotes highly significant values; *denotes significant p-values
Scatter plot showing negative correlation between Average axial length (in mm) of eyeball and Right 2D:4D ratio in males.
Scatter plot showing negative correlation between average axial length (AL in mm) of eyeball and left 2D:4D ratio in males.
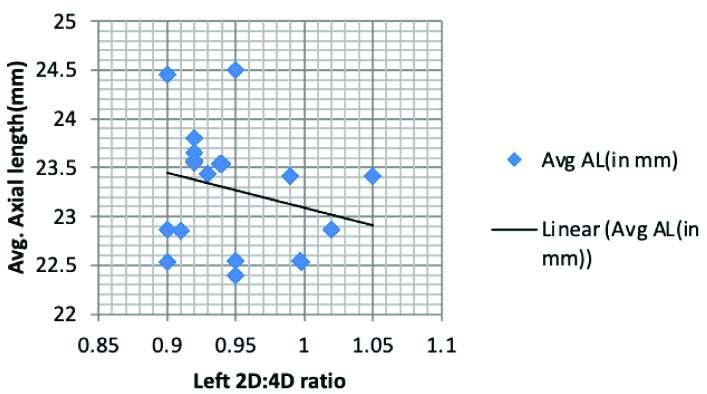
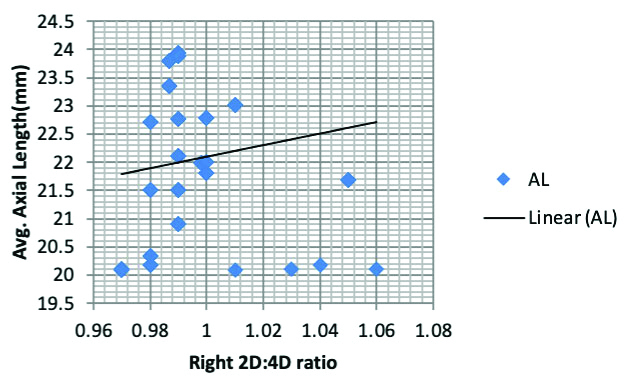
From the [Table/Fig-8,11], it can be seen that, when 2D:4D length ratios of right and left hands were correlated with average axial length of eyeball in females, the result revealed very weak positive but significant correlation for the right hand, but very weakly positive yet non-significant correlation for the left hand (Right hand: r=0.145, p=0.03; left hand: r=0.087, p=0.19.)
Scatter plot showing weakly positive correlation between average axial length (in mm) of eyeball and Right 2D:4D ratio in females.
Discussion
In this study, the males showed a lower digit ratio than the females, i.e., there was evidence of sexual dimorphism in the 2D:4D length ratio of males and females. The difference between the male and female mean 2D:4D ratios of both the right hand and left hands were highly significant p<0.001. These results were similar to the observations made by Ecker A and anthropologist George R who observed that females had a relatively longer index finger than males [14,15]. The evidence of sexual dimorphism in the 2D:4D length ratio of males and females as seen in this study is in conformity with the observations made by McFadden D and Shubel E, where participants were recruited from Texas [16]; and in the study by Fink B et al., where participants were from Austria and United Kingdom [17]; study by Bailey AA and Hurd PL whose subjects were from Canada [18]. McFadden D and Shubel E observed that the 2D:4D ratio was close to 1.0 in females and smaller than 1.0 in males [16]. Fink B et al., reported, that the 2D:4D digit length ratio was significantly lower in males compared to females [17]. Bailey AA and Hurd PL reported that men with more masculine, traits scores in their study had lower digit length ratios compared to females [18]. There however no correlation could be found between finger length ratio and any form of aggresive trait in females. There is a dearth of studies done in India on this subject, and the few that have been conducted were amongst population from Himachal Pradesh by Krishan K et al. Gujarat by Majumder J and Bagepally BS, Jalpaiguri (North Bengal) by Sen J et al. and from Central India by Maitra A et al., [13,19-21]. The study by Krishan K et al., indicated that significant sex differences exist in the index finger length and ring finger length and index and ring finger ratio [19]. The comparison of the other major Indian studies is listed below [Table/Fig-12].
Comparison of findings with other major Indian studies.
| Study | Place of study | Males 2D:4D | Females 2D:4D | Remark significant sexual dimorphism |
|---|
| Majumder J and Bagepally BS [20] | Gujrat, India | 0.98±0.04 | 1.00±0.04 | Yes |
| Sen J et al., [21] | North Bengal | 0.96-0.97 (R)0.96-0.97 (L) | 0.97 (R)0.96-0.97 (L) | No |
| Maitra A et al., [13] | Central India | 0.967±0.033 (R)0.963±0.037 (L) | 0.982±0.027 (R)0.974±0.034 (L) | Yes |
| Present study | South Bengal | 0.89±0.04 (R)0.964±0.042 (L) | 0.993±0.02 (R)0.999±0.04 (L) | Yes |
The height of the males of the present study population showed that 2D:4D length ratio of right and left hands on height of males revealed significant negative correlation, (r=-0.679 for Right side and r=-0.463 for left side), that means, with increase in height in males, there was a decrease in the 2D:4D digit ratio of both left and right hands. However, the strength of correlation was greater on the right side. This is indicative of the fact that the sexually dimorphic pattern in terms of height correlates well with digit ratio in males. The height of the females showed a weak but positively significant relation with height, (r=0.313 for Right hand: r=0.210 for Left hand). Study conducted by Barut C et al., showed that body height correlated negatively with right and left-hand digit ratios in the total sample (N=386); but differed from the present study since they found that men’s height correlated negatively [22], with the digit ratios only for the left hand, whereas women’s height negatively correlated with the digit ratios only for the right hand. Jacob M et al., in their study in a South Indian population noted that [23], Right hand 2D:4D Digit ratio had a weak negative correlation with height in males (r=-0.279 p<0.05) but a weak positive correlation in females (r= 0.235, p<0.05). They did not find any significant association between left hand digit ratio and height. However, Tester N and Campbell A showed that compared to women, men were significantly taller and had lower digit ratios [24]. But, unlike in the present study, they showed that in both men and women, only right hand digit ratio had negative and significant correlation with height.
In the present study, 2D:4D length ratio of right and left hands of males showed weak but positive and significant correlation with BMI (r=0.18 p<0.05 for Right hand and r=0.137 p<0.05 for Left hand). In case of females, right and left hand 2D:4D correlated with BMI showed very weak negative correlation for both hands, but the values were not significant. Barring a few exceptions, this study corroborates well with the findings of, Almasry S et al., where they noted that using the direct method of measurement [25], the 2D:4D was significantly correlated with BMI (r=0.138 p<0.05 for Right Hand and r=0.158 p<0.001) in males. However, there was very weak negative correlation but not statistically significant in females.
In the present study, we noted that axial length of eyeballs exhibited definite sexual dimorphism which corroborates with the findings of Hoffer KJ and Savini G [26]. In both the studies, it was found that the axial length of the eyeball is significantly more in case of males. The axial length of eyeballs of the males of the present study population showed a negative and significant relationship with 2D:4D length ratio for both the hands; (r=-0.706 p<0.001 for Right hand: and r=-0.25, p<0.05 for left hand). The association was moderately strong for the right hand.
In the females, 2D:4D digit length ratios of right and left hands and axial length of eyeball were related as follows: positive and significant for right hand only (r=0.145, p<0.05), but positive and non-significant for left hand. Krishnakumar M et al., reported that digit ratio (2D:4D) of myopes (who had longer axial length of eyeball) were lower when compared to non-myopes in both sexes [27]. The present study had some fundamental differences with the study made by Krishnakumar M et al., [27]. Firstly, they did not find any statistically significant difference between the digit ratio in males and females as opposed to us. Secondly, in the present case, the correlation of axial length and digit ratio differed in the two sexes whereas Krishnakumar M et al., noted that, refractive power of both the eyes (for which ocular axial length is a dependant variable) bear a significant negative correlation with digit ratio in both sexes. This study tried to establish that, 2D:4D digit ratio which is regarded as an anthropometric proxy marker for prenatal sex steroid exposure (which remains constant since birth) bears a significant negative correlation with average ocular axial length in males. However, in females, this correlation was not so well established for both the hands from this study.
Limitation(s)
The main limitation of this study was the small sample size and the time period, which need to be increased to come to more conclusive results.
Conclusion(s)
In this study, authors have tried to establish that 2D:4D ratio can be used as an anthropometric parameter which shows sexual dimorphism. It was found that there exists some correlation in the sexually dimorphic anthropological parameters like height and BMI with 2D:4D digit length ratios in males and females. Thus, a novel attempt was made to establish a correlation between the digit ratio and the sexually dimorphic parameter of ocular axial length. In this regard, a more direct and stronger correlation was found for male 2D:4D ratio and male ocular axial length. Future studies can be aimed at direct correlation between gonadal hormonal assays and 2D:4D ratio, with the aim to establish this marker for early and mass screening of diseases which show typical sexual dimorphisms.
**denotes highly significant values
**denotes highly significant values; *denotes significant p-values
**denotes highly significant values; *denotes significant p-values