Obesity has become a worldwide epidemic, and is increasing in prevalence at an alarming rate in the past few decades, especially in developing countries [1]. A larger and larger number of children and young adults are diagnosed with obesity and metabolic syndrome every year, and this is a matter of serious concern as far as public health is concerned. Abdominal adiposity or central adiposity or visceral adiposity is defined as the excessive accumulation of intra-abdominal fat and has been considered as an important risk factor for major chronic Non Communicable Diseases (NCDs). Abdominal obesity is a major component of the metabolic syndrome, which is known to cause metabolic and cardiac problems in persons of all age groups, and which is an early risk factor for morbidity and mortality in adulthood [2].
Although there are sophisticated methods for evaluating abdominal fat, from an epidemiological point of view, the anthropometric indicators are considered ideal for use in population studies due to their low cost and ease of use [3]. Waist Circumference (WC), WHR and WHtR are reliable and valid methods proposed for the detection of abdominal obesity; these measures are capable of detecting abdominal obesity at a value above a specific and sensitive cut-off point [4,5].
Physical inactivity is one of the causes for accumulation of visceral fat, and exercise has been proven to be effective in reducing both general and abdominal obesity [6]. Physical activity and exercise is encouraged to control obesity, and walking at a brisk pace has been recommended for weight reduction and for improving cardiovascular health. Retro walking or backward walking on a treadmill has been seen to have a higher energy expenditure than forward walking. This increased metabolic cost of retro walking has been postulated to be due to decreased stride length, increased stride frequency and the fact that during retro walking, the quadriceps muscles must contract concentrically rather than eccentrically, all of which leads to an increased energy expenditure [7].
One of the factors which limit exercise in people who are obese is the excess amount of stress placed on the weight bearing joints by exercises such as brisk walking. Retro walking has an advantage over forward walking in this aspect in that retro walking places a reduced stress on the lower limb joints when compared to forward walking [8]. Yet, the effectiveness of retro walking in modifying risk factors for NCD, when compared to forward walking has not yet been conclusively proven. With this in mind, a need was identified to study the effects of retro walking when compared to normal walking on abdominal obesity in young untrained adults and hence the present study was designed with this objective.
Materials and Methods
This study was a single-blind pre-post quasi experimental study without control, which was part of a larger study being conducted with the same objectives, and additional outcome measures [9]. Ethical approval was obtained from the Institutional Ethical Committee (ref no: SU/PT/EC-18/02) and the study was carried out for a period of 11 months from April 2019 to February 2020.
Sample size calculation: Sample size calculation was done with reference to the study conducted by Dangi A and Nirbhavane U, (2014) [10]. Only a convenient number of participants, and not the entire calculated sample, were added in the present study. One hundred and eleven men were recruited by using purposive sampling from the students of an all-male medical university college in Shaqra, Kingdom of Saudi Arabia.
Participation in the study was solicited by means of advertisement placed on the university notice boards and those who fulfilled the inclusion and exclusion criteria were recruited from those who expressed interest to participate in the study.
Inclusion criteria: The study included male subjects aged 18-25 years with WHR more than 1.
Exclusion criteria: Individuals who were undergoing any kind of formal exercise training were excluded, as were those receiving drugs for medical conditions and those with any cardiovascular, metabolic, respiratory, orthopaedic and neurological conditions contraindicating exercise testing and training were also excluded.
Before initial assessment, participants got a data bundle with detailed information about the study, which included the participant’s rights taking part in a research project and a written informed consent form. Once the written consent was obtained, the subjects were randomly allocated to two groups using sequentially numbered opaque sealed envelopes. The intervention names were written sequentially in opaque sealed envelopes, and after screening and consent, the name of the participant was written on the envelope and then the seal was broken, thus determining which group he was allocated to. The participants were screened using the American Heart Association/American College of Sports Medicine (AHA/ACSM) pre-participation questionnaire [11,12]. After that, outcome measures were assessed and interventions carried out.
The outcome measures of the study were BMI, WC, Hip Circumference (HC), WHR, and WHtR which were carried out before the intervention and after, by an assessor, trained by the authors and blinded to the objectives of the study and to the study arm to which the subjects were allotted.
Before starting the interventions, subjects who were unfamiliar with forward or backward treadmill walking, as applicable, was provided basic training by a physical therapist until they could walk on the treadmill confidently, and without support. The participants in the retro walking treadmill training group participated in a supervised retro walking training program including five minutes each of warm-up and cool-down activities for four days a week for six weeks on a treadmill The subjects walked at 4 km per hour at a gradient of 10%, for a time period of fifteen minutes initially, progressing up to thirty minutes over the training period of six weeks [13,14].
The subjects allocated to the forward walking group underwent a supervised forward walking treadmill training program with parameters similar to that of the retro walking training program. (4 km per hour, gradient of 10%, 15-30 minutes of training and 5 minutes each of warm-up and cool-down, four times a week for six weeks).
The warm-up and cool-down exercise periods comprised of ankle-toe movements, gastroc-soleus stretching, hamstring stretching and heel-raise exercises, done for five minutes each. BMI was calculated by the Quetelet Index, i.e., the weight in kilograms divided by the square of height in meters (kg/m2) [15]. WC, HC, WHR and WHt were obtained by the method recommended by the World Health Organisation (WHO). WC was obtained at the highest point of the iliac crest, level with the anterior superior iliac spine, with a measuring tape, while standing [16]. HC was measured at its widest part of the buttocks or hip, with a measuring tape. WHR is the ratio of the circumference of the waist to the circumference of the hips. This was calculated as WC divided by HC, measured in the same units. WHtR of the subjects was measured by dividing their WC, measured by the method mentioned above, by their height, measured using a standard stadiometer, both measured in same units [16]. The outcomes were measured before the intervention, and after the six-week intervention period.
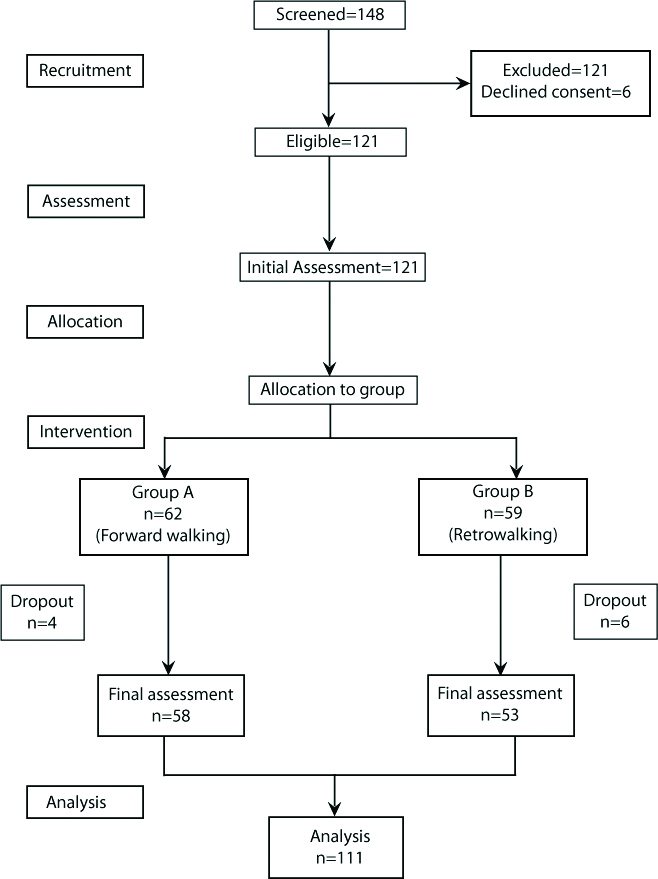
A total of 148 participants volunteered for participation in the study, out of which 21 were excluded for not fulfilling inclusion criteria and 6 participants declined to participate during the initial screening. A total of 121 participants were randomised into the two groups, out of which a further 10 dropped out during the intervention (developed acute infection=6, missed more than 3 consecutive exercise sessions=4). The final data was collected from 111 participants, 58 in the forward walking group, and 53 in the retro walking group. [Table/Fig-1] provides an overview of the progress of participants through the study.
Flowchart showing the progress of participants through the study.
Statistical Analysis
The collected information was summarised by using mean and standard deviation. Parametric measures were used for testing significance, since the data was observed to be normally distributed when tested for normality using the Shapiro-Wilk method. To compare the outcome measures before and after the intervention paired t-test was used and to compare the outcomes between the two groups unpaired t-test was used. The level of significance was set as p<0.01. All analyses were carried out using Statistical Package for the Social Sciences (SPSS) software (IBM SPSS Version 20).
Results
The demographic and baseline characteristics of the study subjects including age height, weight, BMI, WC, WHtR, HC and WHR were recorded [Table/Fig-2]. BMI, WC, WHtR, HC, WHR before and after the treadmill training were recorded and values between both the groups were compared using Independent t-test [Table/Fig-3].
Demographic and baseline characteristics of subjects.
| Demographic and baseline characteristics | Retro walking group (N=53) | Normal walking group (N=58) |
|---|
| Mean | Std. Deviation | Mean | Std. Deviation |
|---|
| Age (years) | 21.58 | 2.17 | 22.67 | 1.98 |
| Height (cm) | 172.17 | 3.73 | 171.00 | 4.20 |
| Weight (kg) | 81.60 | 10.10 | 82.66 | 10.25 |
| BMI (kg/m2) | 27.54 | 3.105 | 28.34 | 3.93 |
| WC | 85.74 | 4.86 | 91.26 | 6.54 |
| WHtR | 0.50 | 0.03 | 0.53 | 0.043 |
| HC | 112.96 | 4.62 | 99.43 | 6.86 |
| WHR | 1.02 | 0.033 | 1.12 | 0.042 |
WHR: Waist-hip ratio; WHtR: Waist-height ratio; BMI: Body mass index; WC: Waist circumference; HC: Hip circumference; Std.: Standard
Comparison of outcome measures within and between groups.
| Outcome measures | Retro walking group (N=53) | Normal walking group (N=58) | p-value** |
|---|
| Pre | Post | p-value* | Pre | Post | p-value* |
|---|
| Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation |
|---|
| BMI | 27.54 | 3.10 | 25.55 | 2.81 | 0.001 | 28.34 | 3.933 | 26.89 | 4.03 | 0.001 | 0.046 |
| WC | 85.74 | 4.86 | 81.72 | 4.62 | 0.001 | 91.26 | 6.544 | 89.00 | 5.98 | 0.001 | 0.001 |
| WHtR | 0.4981 | 0.0288 | 0.4743 | 0.0276 | 0.001 | 0.5340 | 0.0432 | 0.5209 | 0.0406 | 0.001 | 0.001 |
| HC | 112.96 | 4.62 | 114.92 | 4.22 | 0.001 | 99.43 | 6.862 | 99.22 | 7.13 | 0.001 | 0.001 |
| WHR | 1.0211 | 0.0331 | 0.7111 | 0.0337 | 0.001 | 0.9183 | 0.0424 | 1.1241 | 0.0455 | 0.001 | 0.001 |
**Independent t-test is used to test the significance of pre-post differences between the groups; *Paired t-test is used to check the significance of pre-post difference within the groups; WHR: Waist-hip ratio; WHtR: Waist-height ratio; BMI: Body mass index; WC: Waist circumference; HC: Hip circumference; Std.: Standard; p<0.01 considered significant; p-value <0.05 considered significant
Discussion
The present study aimed at documenting the effects of a backward walking program compared to a forward walking program, on obesity measures namely BMI, WHR and WHtR. The WHO has suggested that measures of abdominal obesity or visceral or central obesity such as the WC and WHR are superior to measures of general obesity such as the BMI in detecting obesity related morbidity and risk for lifestyle diseases. Measures of visceral obesity could predict risk for cardiovascular disease, type 2 diabetes mellitus and all cause mortality much better than BMI. Furthermore, these measures used in combination with BMI could increase their capability for discrimination [16]. In this context, a study which documents the effect of a mode of exercise, in comparison with another one, on measures of central obesity gains importance.
Walking is a universally popular exercise mode and is related to several health benefits while minimising the possibility of overstress or injury. Walking has been proved to have multiple health benefits including changes in body composition, aerobic fitness and improvement in overall health [17]. In the present study, both forward walking and retro walking has been seen to reduce significantly all the obesity measures which have been studied, though retro walking was seen to be more effective across outcomes. Dangi A and Nirbhavane U, had found backward walking on a walking track to be as effective as forward walking in decreasing BMI, WHR and body fat percentage [10]. In some other studies as well, treadmill walking, both forward and backward, has been found to be able to decrease BMI, WC and blood pressure and improve the exercise capacity of various populations [18,19].
Also, in the present study, retro walking or backward walking has been seen to have an increased effect on the obesity measures when compared to forward walking. The reason could be the novelty of the exercise, which demands more attention, thus increasing the metabolic load and thus the energy expenditure. Thomas KS et al., have documented that, at similar intensities, retro walking places more perceptual, metabolic and cardiovascular demand on the body when compared to forward walking [14]. Backward walking also challenges dynamic balance in a better manner than forward walking thus recruiting a larger number of neurons into the process of walking [20].
The findings of Cha HG et al., have implicated that backward walking causes an increased stimulation of the lower limb muscles and thus a higher consumption of energy in the lower limb [21]. They also found that the quadriceps femoris and other muscles around the knee are stimulated in a more balanced manner by backward walking than by forward walking [11]. Other authors like Terblanche PE et al., have observed positive changes in body composition and improved levels of cardiovascular fitness with a retro walking program [22]. The height challenge placed by retro walking on the various body systems causes increased energy expenditure when compared to forward walking. This increase in energy expenditure leads to a decreased level of adiposity in the body, thus causing a reduction in adiposity measures such as BMI, WHtR and WHR, as observed in the results of the current study.
Retro walking places a lesser amount of stress on the lower limb joints when compared to forward walking [8]. This is an important aspect to be considered when prescribing exercise in obese persons, since they are more prone to lower limb injury during exercise. Another advantage of backward walking is that it can expend more energy in a shorter time, making the exercise more time-effective, and more likely to be complied [23]. The present study adds to the body of currently available evidence which documents the benefits of retro walking by presenting a reduction in measures of visceral adiposity, which is an important measure of cardiovascular and metabolic risk. Backward walking also has the advantage of being less stressful to the lower limb weight bearing joints, thus reducing the chances of injury during exercise, especially in persons who are obese or overweight. Exercise which modifies obesity, as seen in the present study, is the same type of exercise that can have an effect on modifying risk for lifestyle diseases. Owing to these advantages and practicality of use, backward walking can be a useful addition to any exercise program which aims to modify cardiovascular risk factors and obesity [24,25]. The strengths of the present study include the relatively high sample size and the documentation of the effect backward walking has on measures of visceral adiposity, which, together with the BMI, are excellent markers of metabolic and cardiovascular risk.
Limitation(s)
The limitations are the lack of monitoring of diet of the patients, which could potentially affect abdominal obesity, and non-use of direct measures of energy expenditure or body composition.
Conclusion(s)
In conclusion, the present study results demonstrate that a backward walking program could reduce central obesity more than a forward walking program of similar intensity could. This is important information to be taken into consideration when designing an exercise program to modify cardiovascular risk factors in young individuals. Future studies could be randomised controlled trials which can assess the long term effect of backward walking on cardiovascular risk factors.
WHR: Waist-hip ratio; WHtR: Waist-height ratio; BMI: Body mass index; WC: Waist circumference; HC: Hip circumference; Std.: Standard
**Independent t-test is used to test the significance of pre-post differences between the groups; *Paired t-test is used to check the significance of pre-post difference within the groups; WHR: Waist-hip ratio; WHtR: Waist-height ratio; BMI: Body mass index; WC: Waist circumference; HC: Hip circumference; Std.: Standard; p<0.01 considered significant; p-value <0.05 considered significant