A Rare Case of Fasciola hepatica and its Treatment
Harsha Vardhan Mahalingam1, Rajoo Ramachandran2, Venkatesh Bala Raghu Raji3, Prabhu Radhan Radhakrishnan4, Venkata Sai5
1 Assistant Professor, Department of Radiology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
2 Associate Professor, Department of Radiology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
3 Postgraduate Resident, Department of Radiology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
4 Associate Professor, Department of Radiology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
5 Professor, Department of Radiology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Rajoo Ramachandran, 3A, Anand Apartments, JP Avenue, Dr. Radhakrishnan Salai, Mylapore, Chennai, Tamil Nadu, India.
E-mail: drrajoor.publications@gmail.com
Fascioliasis is a re-emerging food-borne parasitic zoonosis which presents with nonspecific clinical symptoms. Definitive diagnosis requires demonstration of parasitic ova in stool which may often be elusive. Imaging plays a crucial role in raising the possibility of this diagnosis early in the disease course. Contrast-Enhanced Computed Tomography (CECT) of the abdomen was performed in a 44-year-old male with fever, right upper quadrant pain and dyspepsia. The patient later underwent an ultrasound-guided biopsy of liver lesions. The stool examination for ova was negative. Biopsy of the liver lesions showed ill-defined granulomas. Imaging plays a crucial role in establishing the early diagnosis of hepatic fascioliasis especially in nonendemic regions where the clinical suspicion for this diagnosis is low. This article places emphasis on the description of typical imaging features of this condition and the usage of additional investigative/testing techniques recommended by the Center for Disease Control and Prevention (CDC).
Computed tomography, Fascioliasis, Magnetic resonance imaging, Pyogenic abscess
Case Report
A 44-year-old male presented to our emergency department with fever for 10 days, dyspepsia for 5 days and pain in abdomen for 2 days. The fever was high grade and intermittent with no associated chills or rigor. The pain was localised to the right upper quadrant. He was a known diabetic and was on oral medication for the same for the last 4 years. On examination abdomen was soft and there was no mass palpable per abdomen. Local examination was unremarkable with no skin lesions in particular. His blood investigation revealed haemoglobin of 11.4 g/dL with high HbA1c levels of around 9.9 g/dL. Total counts were mildly increased (13000 cells/mL, normal range- 4000-11000 cells/mL) with mildly increased absolute eosinophil count (500, normal range- 0-400). His liver and renal function tests were within normal limits. Enzyme-Linked Immunoassay (ELISA) for Human Immunodeficiency Virus (HIV) was negative. Ultrasound abdomen (done outside) came out to be normal with no significant abnormality. Contrast-enhanced CT of the abdomen done in our institution showed multiple small confluent hypodense nodules in both lobes of the liver [Table/Fig-1], few linear hypodensities along with subcapsular hypodense lesions [Table/Fig-2]. These lesions were best seen on the venous phase of the CT. Also, there were few small nodules in basal segments of lower lobes of both lungs [Table/Fig-3]. Based on the morphology of the lesions suspicion of Fascioliasis was raised. However, duodenal aspirate and stool examination did not reveal any ova. Ultrasound-guided biopsy of the liver lesions showed ill-defined granulomas. Taking into account the presence of peripheral eosinophilia and typical hepatic and basal lung lesions, a working diagnosis of Fascioliasis was considered. The patient was treated with standard 2-dose regimen of oral Triclabendazole. He was discharged on day 3 and was treated on out-patient basis, with complete symptomatic recovery on day 6. Follow-up imaging was not done.
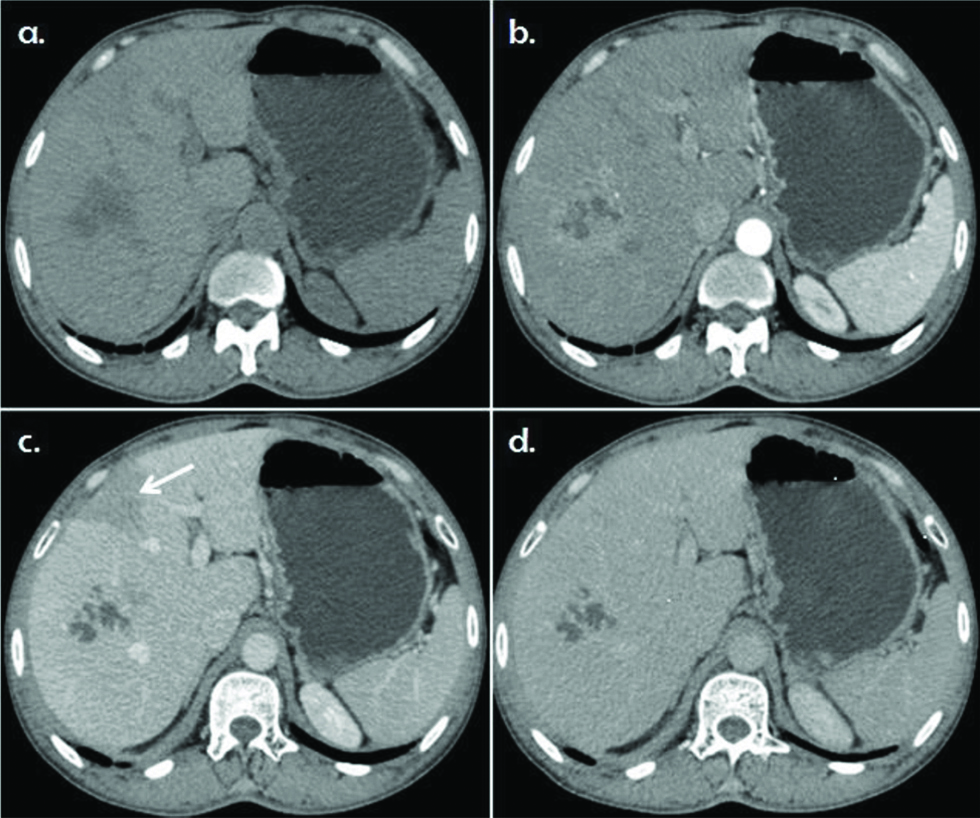
Axial sections of Contrast-Enhanced Computed Tomography (CECT) of the abdomen in a 44-year-old male diagnosed with fascioliasis. a) (unenhanced phase) shows an ill-defined hypodense area representing clustered lesions in the segment VII in the right lobe of liver; b) (arterial phase) and; c) (venous phase) show peripheral enhancement. Note the wedge parenchymal enhancement (white arrow) with capsular involvement in c), d) (delayed phase) show absent centripetal filling in of the contrast.
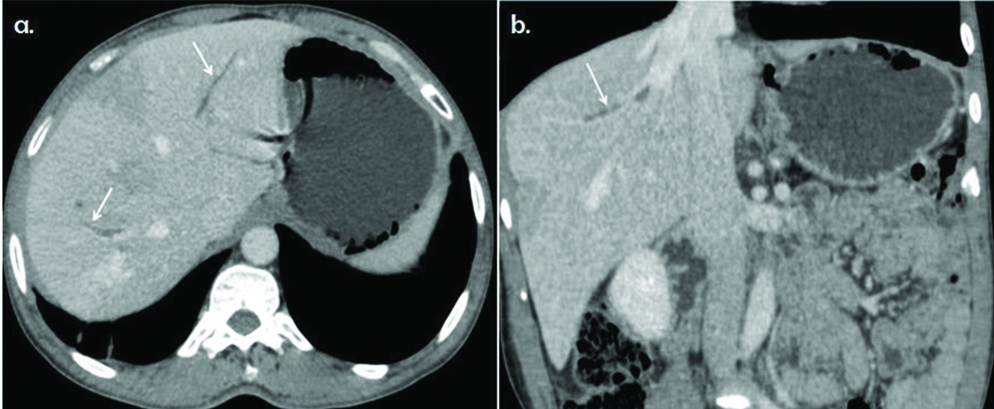
Contrast-Enhanced Computed Tomography (CECT) of the abdomen in venous phase in a 44-year-old male diagnosed with fascioliasis. a) oblique axial; b) oblique coronal show linear hypodensities in the liver parenchyma, representing the linear tracks secondary to the migration of larvae.
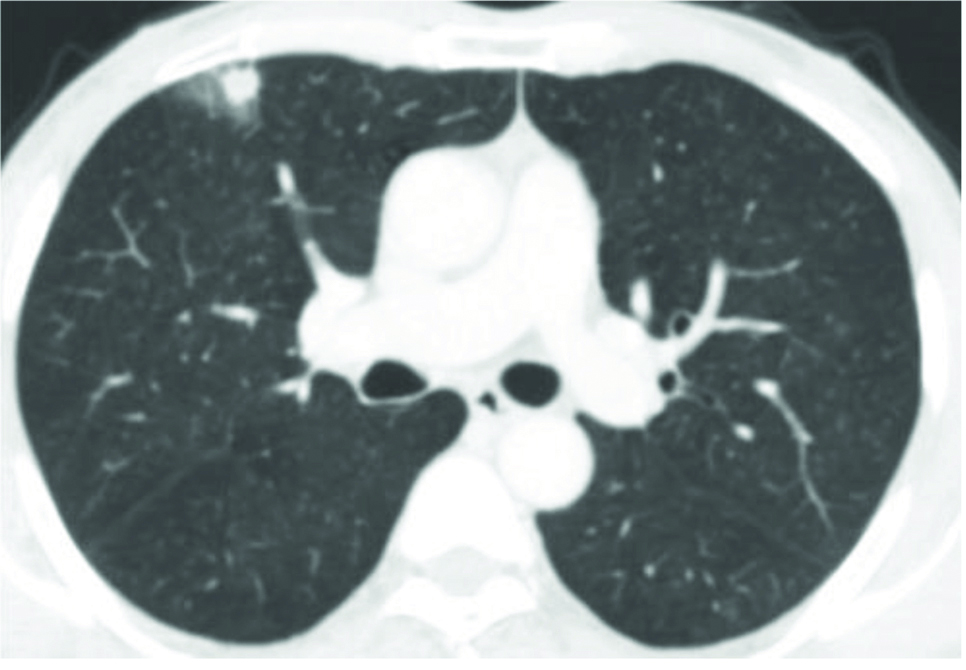
Axial section of computed tomography of the lungs in the lung window shows a solitary subpleural nodule in the right lung with surrounding ground-glass opacity.
Discussion
Fascioliasis is a foodborne zoonotic infestation caused by liver flukes, Fasciola hepatica and Fasciola gigantica. These parasites infect herbivorous mammals and humans after ingestion of metacercaria which are found in water or attached to aquatic plants. Human Fascioliasis is more common in developing countries especially in South America, North Africa, Western Europe and West Asia [1]. No incidence or prevalence data is available for human Fascioliasis in India. A study of infestation in animals from north India showed prevalence rates of around 10% in cattle, around 5% in snails (Lymnea auricularia) and F. gigantica infection being more than F. hepatica [2].
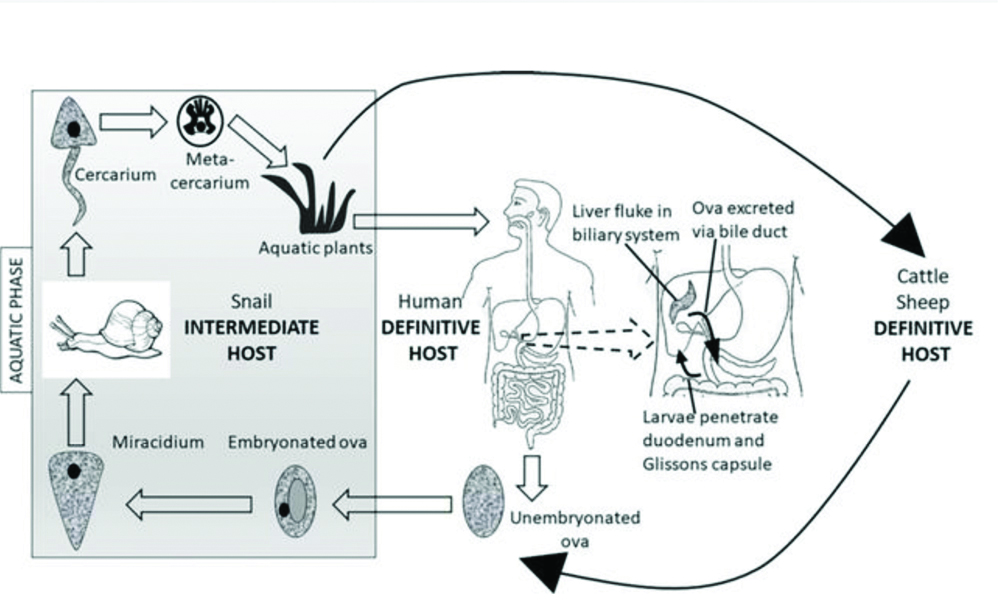
Based on symptomatology the disease in human can be divided into two phases-hepatic or parenchymal (acute) and biliary (chronic) [3]. The life cycle of liver flukes requires 2 hosts-definitive hosts (humans and herbivorous mammals) harboring the adult flukes and intermediate hosts (freshwater snails). The adult flukes live in the biliary system of the definitive host and ova are excreted in feces via the biliary system. When the ova (eggs) come into contact with water they hatch into miracidia which infect snails. They develop into cercaria which leave the snail as free-swimming forms, deposit on aquatic plants and encyst into metacercariae. On ingestion of these infested aquatic plants by the definitive host, the metacercaria hatch into larvae in the duodenum, penetrate the bowel wall, migrate via the peritoneal cavity and liver capsule. They burrow through the liver parenchyma to reach the biliary system [Table/Fig-4]. This comprises the acute phase of the disease. Within the biliary system, the immature larvae mature into adult flukes and in time, start producing eggs. These eggs are in turn reach the intestine and are excreted via faeces. This comprises the chronic phase of the disease.
The life cycle of Fasciola hepatica or liver fluke (adapted from https://www.cdc.gov/parasites/fasciola/biology.html)]
The clinical features of fascioliasis are often nonspecific-patients may present with fever, pain in abdomen, pruritus in the early phase and jaundice and cholangitis in the biliary phase [4]. Hence, imaging findings play an important in suspecting this disease, especially in nonendemic regions. Traditionally, the diagnosis is established by demonstration of parasitic ova in the stool. However, this method of diagnosis is not sensitive especially in the hepatic parenchymal phase of the disease when the parasite has not reached the biliary system. Even in the biliary phase, the parasites may not mature completely to produce eggs, which was the case in our present case scenario [5].
Typical CECT features of the liver lesions in the hepatic parenchymal phase of human fascioliasis as seen on computed tomography are multiple small confluent subcapsular hypodense nodules with linear and tortuous tunnel-like hypodensities, which show a tendency to converge towards the hepatic hilum. Peripheral contrast enhancement can be seen in these lesions. Subcapsular or perihepatic fluid collections and focal capsular thickening and enhancement can be observed. Clues to the diagnosis are multiplicity, ill-defined margins of the nodules and linear distribution extending to the liver capsule. When lesions are large, they can be confused for necrotic metastases and hepatic abscess of other causes. Enlarged periportal nodes are often present.
The biliary phase shows intrahepatic biliary radicle dilatation, oedema and dilatation of the common bile duct and periportal hypodensities. Thickening of the gall bladder wall, Common Bile Duct (CBD) or intrahepatic biliary radicles can be observed. Chronic infection can show punctate parenchymal liver calcifications and sometimes even calcified parasites in the gall bladder lumen [6].
Magnetic Resonance Imaging (MRI) is a useful modality in establishing the hepatic parenchymal involvement of the disease [7]. T2 Weighted (T2W) images in acute phase show capsular hyperintensity with multiple parenchymal hyperintense lines indicating the migration routes of the larvae. T2W images in chronic phase show hyperintense biliary dilatation with filling defects within, which represent the adult worms.
The differential diagnoses in acute phase include other causes of liver abscess such as amoebic and pyogenic liver abscesses. Visceral larva migrans, another parasitic infection, can also present with clustered hypodense hepatic lesions. The differential diagnoses in chronic phase include visceral larva migrans and other causes of cholangitis like sclerosing cholangitis, intraductal cholangiocarinoma, etc., [8].
The complications of fascioliasis include subcapsular liver hematoma, ectopic localisation affecting spleen, pancreas, kidney, bowel and anterior abdominal wall, cholangitis and cholecystitis [9].
A definitive diagnosis of this disease requires a demonstration of ova in stools (occurs late in disease course). ELISA based serology tests have greater sensitivity and specificity and become positive earlier in course the disease [10]. However, these tests remain positive long after disease is treated thus giving false positives. Corproantigen tests show promise in early detection of disease but are not widely available [11]. Centers for Disease Control and Prevention (CDC) have recommended following additional types of testing to support the evidence of fascioliasis:
Complete blood count to look for eosinophilia.
Abdominal cross-sectional imaging or Endoscopic Retrograde Cholangiopancreatography (ERCP).
Histopathological examination of a biopsy specimen of liver or other involved tissue.
In the present case, patient did not consent for serology; however, peripheral eosinophilia was taken into account and typical imaging features of acute parenchymal phase of fascioliasis in the liver and their spread to the basal segments of lower lobes of both the lungs, and arrived at a diagnosis of acute fascioliasis. We treated the patient with the standard 2-dose regimen of oral Triclabendazole (10 mg/kg given 12 hours apart) [12]. The patient was discharged on day 3 and was treated on out-patient basis, with complete symptomatic recovery on day 6. Follow-up blood chemistry on the first month showed a significantly declining trend of eosinophil count. However, follow-up imaging was not done.
Conclusion(s)
Acute fascioliasis is a highly underrated disease due to the lack of awareness of the typical imaging features. The radiological picture of this condition often confused with that of a pyogenic liver abscess and as the management approach drastically varies in these two entities, early and accurate diagnosis is crucial to avoid the long-term biliary complications of fascioliasis. The detection of the characteristic pattern of capsular enhancement, confluent hypodense nodules in subcapsular location converging towards the liver hilum and linear hypodense tracts should raise suspicion of hepatic fascioliasis and appropriate confirmatory tests should be done to arrive at an early diagnosis.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 10, 2020
Manual Googling: Oct 26, 2020
iThenticate Software: Jan 15, 2021 (5%)
[1]. Mas-Coma S, Human Fascoliasis: Epidemiological patterns in human endemic areas of South America, Africa and AsiaSoutheast Asian Journal of Tropical Medicine and Public Health 2004 35(1):01-11. [Google Scholar]
[2]. Garg R, Yadav CL, Kumar RR, Banerjee PS, Vatsya S, Godara R, The epidemiology of fasciolosis in ruminants in different geo-climatic regions of north IndiaTrop Anim Health Prod 2009 41(8):1695-700.10.1007/s11250-009-9367-y19455400 [Google Scholar] [CrossRef] [PubMed]
[3]. Mas-Coma S, Bargues MD, Valero MA, Fascioliasis and other plant-borne trematode zoonosesInt J Parasitol 2005 35(11-12):1255-78.10.1016/j.ijpara.2005.07.01016150452 [Google Scholar] [CrossRef] [PubMed]
[4]. Kaya M, Beştaş R, Çetin S, Clinical presentation and management of Fasciola hepatica infection: Single-center experienceWorld J Gastroenterol WJG 2011 17(44):4899-904.10.3748/wjg.v17.i44.489922171131 [Google Scholar] [CrossRef] [PubMed]
[5]. Mas-Coma S, Bargues MD, Valero MA, Diagnosis of human fascioliasis by stool and blood techniques: Update for the present global scenarioParasitology 2014 141(14):1918-46.10.1017/S003118201400086925077569 [Google Scholar] [CrossRef] [PubMed]
[6]. Kabaalioglu A, Ceken K, Alimoglu E, Saba R, Cubuk M, Arslan G, Hepatobiliary fascioliasis: Sonographic and CT findings in 87 patients during the initial phase and long-term follow-upAm J Roentgenol 2007 189(4):824-28.10.2214/AJR.07.212717885052 [Google Scholar] [CrossRef] [PubMed]
[7]. Dusak A, Onur MR, Cicek M, Firat U, Ren T, Dogra VS, Radiological imaging features of fasciola hepatica infection-A pictorial reviewJ Clin Imaging Sci 2012 2:210.4103/2156-7514.9237222347685 [Google Scholar] [CrossRef] [PubMed]
[8]. Preza O, Klapa I, Tsiakalos A, Cokkinos DD, Chatziioannou A, Fascioliasis: A challenging differential diagnosis for radiologistsJ Radiol Case Rep 2019 13(1):11-16.10.3941/jrcr.v13i1.345131565163 [Google Scholar] [CrossRef] [PubMed]
[9]. Bächler P, Baladron MJ, Menias C, Beddings I, Loch R, Zalaquett E, Multimodality Imaging of Liver Infections: Differential Diagnosis and Potential PitfallsRadio Graphics 2016 36(4):1001-23.10.1148/rg.201615019627232504 [Google Scholar] [CrossRef] [PubMed]
[10]. Sarkari B, Khabisi SA, Immunodiagnosis of human fascioliasis: An update of concepts and performances of the serological assaysJ Clin Diagn Res 2017 11(6):OE05-10.10.7860/JCDR/2017/26066.1008628764235 [Google Scholar] [CrossRef] [PubMed]
[11]. Valero MA, Periago MV, Pérez-Crespo I, Angles R, Villegas F, Field evaluation of a coproantigen detection test for fascioliasis diagnosis and surveillance in human hyperendemic areas of Andean countriesPLOS Neglected Tropical Diseases 2012 6(9):e181210.1371/journal.pntd.000181223029575 [Google Scholar] [CrossRef] [PubMed]
[12]. Fica A, Dabanch J, Farias C, Castro M, Jercic MI, Weitzel T, Acute fascioliasis-clinical and epidemiological features of four patients in ChileClinical Microbiology and Infection 2012 18(1):91-96.10.1111/j.1469-0691.2011.03575.x21668579 [Google Scholar] [CrossRef] [PubMed]