Introduction
Breast Cancer is the most common type of cancer in women and the 2nd leading cause of death. The treatment of breast cancer includes surgery, chemotherapy, radiation therapy, hormone therapy or combination of these treatments. One of the most important complications which occurs in one out of four women is lymphoedema. Physiotherapy plays an important role in creating awareness, prevention, early diagnosis and treatment of secondary lymphoedema. The systematic reviews which were already done focused on only one intervention or combination of two or more interventions for lymphoedema with or without other complication related to breast cancer.
Aim
To systematically review the randomised controlled trials to evaluate the effect of various physiotherapy interventions that are used in the prevention and relief of secondary lymphoedema in postoperative breast cancer patients.
Materials and Methods
Relevant studies were retrieved through PubMed, Cochrane, EMBASE and Google Scholar databases ranging from the year 2004 (January) to 2020 (March). The language of search was English. The keywords used for the search were breast cancer, interventions, physiotherapy, postoperative, secondary lymphoedema, treatment, prevention. Total 14 randomised controlled trials were included in this study according to the inclusion criteria. The trials included interventions like Manual Lymphatic Drainage (MLD), compression therapy, Range of Motion (ROM) exercises and massage.
Results
A total of 244 relevant articles were found out of which 14 Randomised Controlled Trials (RCTs) were included in this study. MLD showed positive effects on lymphoedema prevention and treatment as an individual intervention or in combination with other interventions. Compression sleeves/corsets also showed positive effect on lymphoedema. Resistance exercises showed no risk of precipitating or increasing lymphoedema. Shoulder programs showed that delayed mobilisation of shoulder after one week is beneficial for reduction of lymphoedema. Physiotherapeutic stimulation showed positive effects on lymphoedema by increasing the lymphatic flow and velocity.
Conclusion
Physiotherapy interventions like MLD, compression garments, stretching and strengthening, resistance exercises and ROM exercises have a potential effect in the treatment and prevention of secondary lymphoedema.
Interventions, Management, Meta-regression model, Prevalence of premenstrual syndrome, Risk reduction, Symptom
Introduction
Breast cancer is the most common type of cancer in women [1]. It is the 2nd leading cause of death in women [2]. Breast cancer treatments include individual or combination treatments like surgery, chemotherapy, radiation therapy, hormone therapy [3]. There are postoperative complications which include pain, reduced shoulder ROM, lymphoedema or lymphatic cording, wound complications reduces muscle force, postural changes and lack of sensibility [4]. One of the most important complications which occur, in one out of four women, is lymphoedema [5].
Physiotherapy plays an important role in creating awareness, prevention, early diagnosis and treatment of secondary lymphoedema [6]. There were several systematic reviews which studied the effect of only exercise programs on shoulder mobility, lymphoedema, strength and pain [7-11]. Some studies investigated the effect of MLD and compression therapy on breast cancer related lymphoedema [12-14]. Studies also investigated the effect of exercise on health-related outcomes and pre-operative exercises on upper extremity recovery in Breast cancer patients [15,16]. Postoperative physiotherapy interventions which include general exercises, stretching, joint and tissue mobilisations for shoulder pain and ROM were studied [17,18]. Effect of physiotherapy interventions like combined physiotherapy, intermittent pneumatic compression, arm elevation, Manual Lymphatic Drainage (MLD) was also studied [19-21].
The previous systematic reviews focused on a single intervention or combination of two or more interventions for lymphoedema with or without other complications related to breast cancer [7-21]. Thus, the aim of this study was to evaluate the overall effect of various interventions used in physiotherapy for the prevention and treatment of secondary lymphoedema.
Materials and Methods
Search Strategy
Total 244 studies which included systematic reviews with or without meta-analysis, literature reviews, randomised controlled trials were retrieved by means of computerised comprehensive search in the following databases from the year 2004 (January) to 2020 (March): PubMed, Cochrane, EMBASE and Google scholar. Key words used were physiotherapy, prevention, treatment, intervention relief and breast cancer, postoperative, secondary lymphoedema.
Study Selection and Data Extraction
Studies included in the review were based on the following-
Inclusion criteria: Randomised controlled trials, published in English language, study population must be postoperative breast cancer patients with secondary lymphoedema or those undergoing physiotherapy treatment for prevention of secondary lymphoedema with or without other complications were included.
Exclusion criteria: Non-randomised controlled trials, case reviews, systematic reviews, literature reviews, case reports and abstracts of posters, randomised controlled trials not related to lymphoedema as a complication with physiotherapy intervention, studies with lymphoedema as a complication without physiotherapy interventions were excluded.
Primary outcome measures were the effect of physiotherapy in the prevention and treatment of secondary lymphoedema in postoperative breast cancer patients. Secondary outcome measures were other upper extremity impairments related to shoulder ROM, quality of life, strength. The quality of each study was assessed using the PEDRO scale [22].
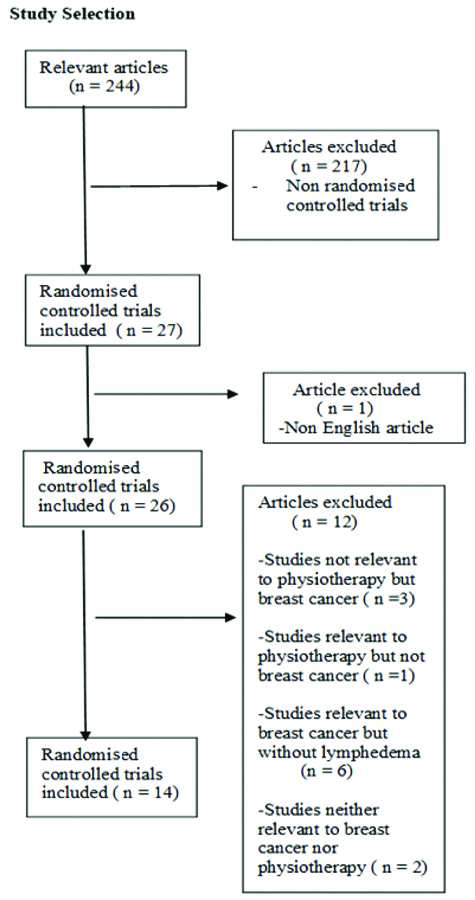
The computerised search found 244 potentially relevant articles out of which 217 non-randomised controlled trials were excluded and 27 randomised controlled trials were included in the study. Out of the 27, 1 non-English study was excluded. From the remaining 26 articles, 3 studies not relevant to physiotherapy but breast cancer, 1 study relevant to physiotherapy but not breast cancer, 6 studies relevant to breast cancer but without lymphedema and 2 studies neither relevant to breast cancer nor physiotherapy were excluded. Finally, 14 studies were included in the systematic review based on the inclusion criteria [5,6,23-34] [Table/Fig-1].
Results
A total of 14 studies (RCTs) were included in this systematic review [5,6,23-34]. The PEDro Scale was used to access the quality of each study which has a total score ranging from 0 to 11 [22]. Twelve studies had a PEDro score in the range of 6-8 and 2 studies with a score in the range of 9-10. Thus, the overall score reflects that the quality of the studies included was good [Table/Fig-2].
| Author | Eligibility criteria | Random allocation | Concealed allocation | Groups similar at baseline | Participant blinding | Therapist blinding | Assessor blinding | <15% dropouts | Intention to treat analysis | Between group difference reported | Point estimate and variability reported | Total (0 to 11) |
|---|
| Devoogdt N et al., [23] (2018) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| Ochalek K et al., [24] (2017) | No | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Dönmez AA and Kapucu S. [5] (2017) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Hansdorfer KR et al., [25] (2016) | No | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Bergmann A et al., [26] (2014) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Kilbreath SL et al., [27] (2012) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Zimmermann A et al., [28] (2012) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Devoogdt N et al., [29] (2011) | No | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Lacomba MT et al., [6] (2010) | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Todd J et al., [30] (2008) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Johansson K et al., [31] (2005) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| Mc Neely ML et al., [32] (2009) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 9 |
| Cho Y et al., [33] (2015) | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Sarri AJ et al., [34] (2010) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
Based on the [Table/Fig-3] it can be inferred that the various physiotherapy interventions including education, MLD, compression bandaging, structural resistance training program, delayed full shoulder mobilisation exercise program, early physiotherapeutic stimulation etc., can be safely used for the patients with secondary lymphoedema. The interventions used have reduced the lymphoedema and improved the lymphatic flow without any aggravation or further complications. Thus, interventions have a potential effect in the prevention and relief of secondary lymphoedema in the postoperative breast cancer patients.
Summary of RCTs of physiotherapy interventions in the prevention and relief of secondary lymphoedema.
| Author | Country | Participants | Experimental group intervention | Control group intervention | Outcome measures | Results |
|---|
| Devoogdt N et al., [23] | Belgium | Adults undergoing unilateral dissection for Breast Cancer | Guidelines on prevention of lymphoedema, exercise therapy and manual lymphatic drainage (n=79) | Guidelines on prevention of lymphoedema and exercise therapy(n=81) | - Cumulative incidence of arm lymphoedema- Point prevalence of lymphoedema- Arm volumeShoulder range of motion- Quality of life and function | 60 months after surgery, cumulative incidence rate was less in the experimental group compared to control group. Other outcomes were comparable between the groups |
| Ochalek Ket al., [24] | Poland | Pre-operative patients of Breast Cancer | Compression with circular knit sleeves (n=22) | No compression with circular knit sleeves (n=23) | - Limb and oedema volumes- Interface pressure under the sleeves- Compliance and quality of life | Less oedema in the control group after 3, 6, 9 and 12 months.No difference between groups in health related quality of life. |
| Dönmez AA and Kapucu S [5] | Turkey | Breast cancer patients with training for lymphoedema | Physical activity program and simple lymphatic drainage(n=25) | No intervention (n=27) | - Lymphoedema Visual Analog Scale (VAS)- Physical activity- Upper extremity problems | Upper of upper extremity increased by 2 times in the control group at 6th week (p<0.05). Lymphoedema symptoms severity scores reduced in the intervention group compared to baseline (p<0.01) |
| Hansdorfer KR et al., [25] | Poland | 37 patients who had undergone mastectomy and lymphadenectomy. | - Compression corset for 1 month after surgery.- After 7 months follow-up randomly assigned again with properly fitted compression corsets. | - No physiotherapy- No physiotherapy | - Size of truncal lymphoedema- Pain | Pain reduced in both experimental and control groups. Compression corsets could treat and prevent and lymphoedema and reduce pain associated with surgery. |
| Bergmann A et al., [26] | Brazil | Breast Cancer patients with secondary lymphoedema | Manual lymphatic drainage, skin care, bandaging, remedial exercises(n=28) | Skin care, bandaging, remedial exercises(n=29) | - Swelling- Pain- Shoulder function | Both groups showed reduction in excess limb volume and addition of manual lymphatic drainage did not have any effect. |
| Kilbreath SL et al., [27] | Australia | Breast cancer patients (4-6 weeks postoperativel) | - Passive stretching and progressive resistance training for shoulder muscles- Weekly session of exercises and home program. (n=81) | No exercises. Only fortnightly assessments (n=27) | - Self reported arm symptoms- Shoulder range of motion- Strength- Lymphoedema | Self-reported symptoms were similar in both the groups. Range of motion and abductor strength was greater in experimental group. No precipitation of lymphoedema with resistance training. |
| Zimmermann A et al., [28] | Poland | 67 women who underwent breast cancer surgery. | Manal lymphatic drainage (n=33) | No Manual lymphatic drainage | - Arm volume | Arm volume increased in the control group compared to before surgery.Manual lymphatic drainage prevented lymphoedema of the affected side. |
| Devoogdt N et al., [29] | Belgium | Breast cancer patients with unilateral lymph node dissection | Guidelines on lymphoedema prevention, exercise therapy and manual lymphatic drainage (n=79) | Guidelines on lymphoedema prevention and exercise therapy (n=81) | - Cumulative incidence of arm lymphoedema and time to develop it. | At 12 months after surgery cumulative incidence and time to develop lymphoedema was comparable between the groups. |
| Lacomba MT et al., [6] | Spain | Breast cancer patients with axillary lymph node dissection who developed secondary lymphoedema | Manual lymphatic drainage, massage of scar tissue, progressive active assisted and active range of motion shoulder exercises, education strategy (n=4) | Only educational strategy (n=14) | - Incidence of secondary lymphoedema | Incidence was higher in control group. Volume ratio increased in both groups at 12 month follow-up. More survival rate was seen in the experimental group. |
| Todd Jet al., [30] | UK | Postoperative Breast Cancer patients | Arm exercises and shoulder movements below shoulder level only for first 7 days after surgery.(n=58) | Exercises above shoulder level within 48 hours(n=58) | - Incidence of lymphoedema - Volume different between 2 limbs- Wound drainage volume- Shoulder range of motion- Grip strength- Health related quality of life | More women with lymphoedema and increased limb volume difference in early full shoulder mobilisation compared to delayed mobilisation group. No difference in shoulder range, grip strength and self evaluated outcomes. |
| Johansson Ket al., [31] | Australia | Breast cancer patients with unilateral arm lymphoedema following treatment older than 70 years | Compression sleeves with low intensity resistance exercises(n=16) | Without compression sleeves with low intensity resistance exercises. | - Arm volume- Subjective sensations- Perceived exertion- Physical activity- Arm volume | Increase in arm volume of lymphoedema immediately after exercise in both the groups. At 2 weeks no volume increase and reduced lymphoedema volume. Perceived exertion was low with or without sleeves but higher with sleeves during exercise. |
| Mc Neeley ML et al., [32] | Canada | 50 breast cancer patients with lymphoedema | 4 weeks of combined manual lymphatic drainage and compression bandaging (n=25) | 4 weeks of compression bandaging (n=25) | Arm volume | Experimental group showed large % reduction in volume compared to control group and also compared to individuals with moderate or severe lymphoedema with either treatment. |
| Cho Yet al., [33] | Berlin | 41 Breast Cancer patients with visible and palpable cords on the arm and axilla | Physiotherapy, manual lymphatic drainage: 5 times/week for 4 weeks.(n=21) | Physiotherapy only: 3 times/week for 4 weeks(n=20) | - Arm volume- Shoulder function- Quality of life- Pain | Arm volume and NRS scores were lower in experimental group than the control group. Lymphoedema was seen in control group and not experimental group. Quality of life, shoulder flexor strength, DASH, NRS improved in both the groups after 4 weeks interval. |
| Sarri AJ et al., [34] | Brazil | 22 patients who underwent lymphoscintigraphy firstly without physiotherapy stimulation and second after randomisation into 2 groups. | Physiotherapeutic stimulation using Foldi’s technique. (n=12) | Without Physiotherapeutic stimulation (n=10) | - Lymphatic flow progression | There was increase in progression of lymphatic flow along with increase in number of lymph nodes and lymphatic velocity. |
Discussion
Breast cancer is the most frequent type of cancer among all the other types in females [5,23-25]. The survival rate is increasing due to the evolution in the treatment and diagnostic procedures [23]. The most common complication of breast cancer is lymphoedema [5,23,24]. After axillary dissection, immediate application of MLD may prevent the development of lymphoedema as it eliminates accumulated water and proteins out of the interstitial tissue and stimulates rerouting of the lymphatic system after axillary dissection [23]. Lymphoedema manifestation at any stage can be managed by complete decongestive therapy or compression therapy as shown by many reports [5,24]. It is the most efficient treatment which can be applied in different conditions from cardiovascular diseases, kidney diseases, deep vein thrombosis, or lymphangitis [25].
The aim of this study was to systematically review the randomised controlled trials to evaluate the effect of various physiotherapy interventions that are used in the prevention and relief of secondary lymphoedema in postoperative breast cancer patients. The overall finding suggests that physiotherapy interventions have a good potential to prevent secondary lymphoedema and provide relief to the patients [5,6,23-34]. Physiotherapy interventions including education, MLD, compression bandaging and exercises is included in a combined treatment program for lymphoedema which is called as Complex Physical Therapy (CPT) [32].
Case reports have been published that found reduction of lymphoedema with return of the affected limb to the normal state following CPT [6,32]. Early stage Physical activity and Simple Lymphatic Drainage (SLD) in clinical and home settings can be effective in prevention of secondary lymphoedema along with reduction in the prevalence of lymphoedema related symptoms [5].
After breast cancer surgery, the muscles on the affected side are weak and it leads to reduced elevation of the arm. The healing of the lymphatics of the operated side and the soft tissues is impeded by reduced strength of the muscles. It is hypothesised that a structural resistance training program enhances lymph flow, protein resorption and improves flexibility of soft tissues [27]. Studies have shown that resistance training does not precipitate lymphoedema in the postoperative period [27,31]. Delayed full shoulder mobilisation exercise program for 1 week after axillary node dissection was recommended by one study which showed more women who developed lymphoedema in the early full mobilisation group compared to the delayed full shoulder mobilisation group [30]. Early physiotherapeutic stimulation has proved to be effective in patients undergoing radical axillary dissection in prevention of lymphoedema [34].
Based on this study, it can be inferred that physiotherapy interventions have a positive effect in the prevention and relief of secondary lymphoedema.
Limitation(s)
Although, this systematic review included only the RCTs, the physiotherapy interventions used for the prevention and relief of secondary lymphoedema were not homogenous. The interventions used varied from one study to the other except for few similarities. Another limitation is that, the review has not focused on particular symptoms related to lymphoedema and the symptom-based prevention and relief for the same. The prevalence of lymphoedema as a secondary complication in postoperative breast cancer patients has also not been mentioned.
Conclusion(s)
The study concluded that the physiotherapy interventions have a potential effect in the treatment and prevention of secondary lymphoedema.
[1]. Sharma GN, Dave R, Sanadya J, Sharma P, Sharma KK, Various types and management of breast cancer: An overviewJournal of Advanced Pharmaceutical Technology & Research 2010 1(2):109-26. [Google Scholar]
[2]. Sun YS, Zhao Z, Yang ZN, Xu F, Lu HJ, Zhu ZY, Risk factors and preventions of breast cancerInternational Journal of Biological Sciences 2017 13(11):1387-97.10.7150/ijbs.2163529209143 [Google Scholar] [CrossRef] [PubMed]
[3]. Nounou MI, El Amrawy F, Ahmed N, Abdelraouf K, Goda S, Syed Sha Qhattal H, Breast cancer conventional diagnosis and treatment modalities and recent patents and technologiesBreast Cancer Basic and Clinical Research 2015 9(2):17-34.10.4137/BCBCR.S2942026462242 [Google Scholar] [CrossRef] [PubMed]
[4]. Da Luz SC, da Silva Honório GJ, The role of physiotherapy in female breast cancerWomen’s Health and Biomechanics: Where Medicine and Engineering Meet 2018 9(29):71-82.10.1007/978-3-319-71574-2_6 [Google Scholar] [CrossRef]
[5]. Dönmez AA, Kapucu S, The effectiveness of a clinical and home-based physical activity program and simple lymphatic drainage in the prevention of breast cancer-related lymphedema A prospective randomised controlled studyEuropean Journal of Oncology Nursing 2017 31:12-21.10.1016/j.ejon.2017.09.00429173822 [Google Scholar] [CrossRef] [PubMed]
[6]. Lacomba MT, Sánchez MJY, Goñi ÁZ, Merino DP, del Moral OM, Téllez EC, Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer randomised, single blinded, clinical trialBMJ 2010 340:b539610.1136/bmj.b539620068255 [Google Scholar] [CrossRef] [PubMed]
[7]. Chan DN, Lui LY, So WK, Effectiveness of exercise programmes on shoulder mobility and lymphoedema after axillary lymph node dissection for breast cancer systematic reviewJournal of Advanced Nursing 2010 66(9):1902-14.10.1111/j.1365-2648.2010.05374.x20626480 [Google Scholar] [CrossRef] [PubMed]
[8]. Mc Neely ML, Campbell K, Ospina M, Rowe BH, Dabbs K, Klassen TP, Exercise interventions for upper-limb dysfunction due to breast cancer treatmentCochrane Database of Systematic Reviews 2010 (6):CD00521110.1002/14651858.CD005211.pub220556760 [Google Scholar] [CrossRef] [PubMed]
[9]. Cavanaugh KM, Effects of early exercise on the development of lymphedema in patients with breast cancer treated with axillary lymph node dissectionJournal of Oncology Practice 2011 7(2):89-93.10.1200/JOP.2010.00013621731515 [Google Scholar] [CrossRef] [PubMed]
[10]. Kwan ML, Cohn JC, Armer JM, Stewart BR, Cormier JN, Exercise in patients with lymphedema A systematic review of the contemporary literatureJournal of Cancer Survivorship 2011 5(4):320-36.10.1007/s11764-011-0203-922002586 [Google Scholar] [CrossRef] [PubMed]
[11]. Ribeiro IL, Moreira RFC, Ferrari AV, Alburquerque Sendín F, Camargo PR, Salvini TF, Effectiveness of early rehabilitation on range of motion, muscle strength and arm function after breast cancer surgery A systematic review of randomised controlled trialsClinical Rehabilitation 2019 33(12):1876-86.10.1177/026921551987302631480855 [Google Scholar] [CrossRef] [PubMed]
[12]. Kligman L, Wong RK, Johnston M, Laetsch NS, Supportive Care Guidelines Group of Cancer Care OntarioThe treatment of lymphedema related to breast cancer A systematic review and evidence summarySupportive Care in Cancer 2004 12(6):421-31.10.1007/s00520-004-0627-015095073 [Google Scholar] [CrossRef] [PubMed]
[13]. Huang TW, Tseng SH, Lin CC, Bai CH, Chen CS, Hung CS, Effects of manual lymphatic drainage on breast cancer-related lymphedema A systematic review and meta-analysis of randomised controlled trialsWorld Journal of Surgical Oncology 2013 11(1):1510.1186/1477-7819-11-1523347817 [Google Scholar] [CrossRef] [PubMed]
[14]. Jeffs E, Ream E, Taylor C, Bick D, Clinical effectiveness of decongestive treatments on excess arm volume and patient-centered outcomes in women with early breast cancer-related arm lymphedema: A systematic reviewJBI Database of Systematic Reviews and Implementation Reports 2018 16(2):45310.11124/JBISRIR-2016-00318529419623 [Google Scholar] [CrossRef] [PubMed]
[15]. Chung C, Lee S, Hwang Park E, Systematic review of exercise effects on health outcomes in women with breast cancerAsian Nursing Research 2013 7(3):149-59.10.1016/j.anr.2013.07.00525030253 [Google Scholar] [CrossRef] [PubMed]
[16]. Yang A, Sokolof J, Gulati A, The effect of preoperative exercise on upper extremity recovery following breast cancer surgery A systematic reviewInternational Journal of Rehabilitation Research 2018 41(3):189-96.10.1097/MRR.000000000000028829683834 [Google Scholar] [CrossRef] [PubMed]
[17]. De Groef A, Van Kampen M, Dieltjens E, Christiaens MR, Neven P, Geraerts I, Effectiveness of postoperative physical therapy for upper-limb impairments after breast cancer treatment A systematic reviewArchives of Physical Medicine and Rehabilitation 2015 96(6):1140-53.10.1016/j.apmr.2015.01.00625595999 [Google Scholar] [CrossRef] [PubMed]
[18]. Giacalone A, Alessandria P, Ruberti E, The physiotherapy intervention for shoulder pain in patients treated for breast cancer: Systematic reviewCureus 2019 11(12)10.7759/cureus.641631988817 [Google Scholar] [CrossRef] [PubMed]
[19]. Devoogdt N, Kampen MV, Geraerts I, Coremans T, Christiaens MR, Different physical treatment modalities for lymphoedema developing after axillary lymph node dissection for breast cancer: A reviewEuropean Journal of Obstetrics & Gynecology and Reproductive Biology 2010 149(1):03-09.10.1016/j.ejogrb.2009.11.01620018422 [Google Scholar] [CrossRef] [PubMed]
[20]. Kärki A, Anttila H, Tasmuth T, Rautakorpi UM, Lymphoedema therapy in breast cancer patients A systematic review on effectiveness and a survey of current practices and costs in FinlandActaoncologica 2009 48(6):850-59.10.1080/0284186090275525119235573 [Google Scholar] [CrossRef] [PubMed]
[21]. Baumann FT, Reike A, Hallek M, Wiskemann J, Reimer V, Does exercise have a preventive effect on secondary lymphedema in breast cancer patients following local treatment A systematic reviewBreast Care 2018 13(5):380-85.10.1159/00048742830498426 [Google Scholar] [CrossRef] [PubMed]
[22]. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M, Reliability of the PEDro scale for rating quality of randomised controlled trialsPhys Ther 2003 83(8):713-21.10.1093/ptj/83.8.71312882612 [Google Scholar] [CrossRef] [PubMed]
[23]. Devoogdt N, Geraerts I, Van Kampen M, De Vrieze T, Vos L, Neven P, Manual lymph drainage may not have a preventive effect on the development of breast cancer-related lymphoedema in the long term A randomised trialJournal of Physiotherapy 2018 64(4):245-54.10.1016/j.jphys.2018.08.00730241913 [Google Scholar] [CrossRef] [PubMed]
[24]. Ochalek K, Gradalski T, Partsch H, Preventing early postoperative arm swelling and lymphedema manifestation by compression sleeves after axillary lymph node interventions in breast cancer patients A randomised controlled trialJournal of Pain and Symptom Management 2017 54(3):346-54.10.1016/j.jpainsymman.2017.04.01428797867 [Google Scholar] [CrossRef] [PubMed]
[25]. Hansdorfer KR, Teodorczyk J, Gruszecka A, Wydra J, Lass P, Relevance of low-pressure compression corsets in physiotherapeutic treatment of patients after mastectomy and lymphadenectomyPatient Preference and Adherence 2016 10:117710.2147/PPA.S10832627445465 [Google Scholar] [CrossRef] [PubMed]
[26]. Bergmann A, Ferreira MDCL, De Aguiar SS, De Almeida Dias R, De Souza Abrahao K, Paltrinieri EM, Physiotherapy in upper limb lymphedema after breast cancer treatment A randomised studyLymphology 2014 47(2):82-91. [Google Scholar]
[27]. Kilbreath SL, Refshauge KM, Beith JM, Ward LC, Lee M, Simpson JM, Upper limb progressive resistance training and stretching exercises following surgery for early breast cancer: A randomised controlled trialBreast Cancer Research and Treatment 2012 133(2):667-76.10.1007/s10549-012-1964-122286332 [Google Scholar] [CrossRef] [PubMed]
[28]. Zimmermann A, Wozniewski M, Szklarska A, Lipowicz A, Szuba A, Efficacy of manual lymphatic drainage in preventing secondary lymphedema after breast cancer surgeryLymphology 2012 45(3):103-12. [Google Scholar]
[29]. Devoogdt N, Christiaens MR, Geraerts I, Truijen S, Smeets A, Leunen K, Effect of manual lymph drainage in addition to guidelines and exercise therapy on arm lymphoedema related to breast cancer: Randomised controlled trialBMJ 2011 343:d532610.1136/bmj.d532621885537 [Google Scholar] [CrossRef] [PubMed]
[30]. Todd J, Scally A, Dodwell D, Horgan K, Topping A, A randomised controlled trial of two programmes of shoulder exercise following axillary node dissection for invasive breast cancerPhysiotherapy 2008 94(4):265-73.10.1016/j.physio.2008.09.005 [Google Scholar] [CrossRef]
[31]. Johansson K, Tibe K, Weibull A, Newton RU, Low intensity resistance exercise for breast cancer patients with arm lymphedema with or without compression sleeveLymphology 2005 38(4):167-80. [Google Scholar]
[32]. Mc Neely ML, Magee DJ, Lees AW, Bagnall KM, Haykowsky M, Hanson J, The addition of manual lymph drainage to compression therapy for breast cancer related lymphedema: A randomised controlled trialBreast Cancer Research and Treatment 2004 86(2):95-106.10.1023/B:BREA.0000032978.67677.9f15319562 [Google Scholar] [CrossRef] [PubMed]
[33]. Cho Y, Do J, Jung S, Kwon O, Jeon JY, Effects of a physical therapy program combined with manual lymphatic drainage on shoulder function, quality of life, lymphedema incidence, and pain in breast cancer patients with axillary web syndrome following axillary dissectionSupportive Care in Cancer 2016 24(5):2047-57.10.1007/s00520-015-3005-126542271 [Google Scholar] [CrossRef] [PubMed]
[34]. Sarri AJ, Moriguchi SM, Dias R, Peres SV, Da Silva ET, Koga KH, Physiotherapeutic stimulation, Early prevention of lymphedema following axillary lymph node dissection for breast cancer treatmentExperimental and Therapeutic Medicine 2010 1(1):147-52.10.3892/etm_0000002423136607 [Google Scholar] [CrossRef] [PubMed]