The sound of rain hitting the street may not be a transcendental event for most of us, but for four-year-old cochlear implant user Laxmi, it makes her shout at the top of her voice, “pa-ani” (water!) eliciting a resounding cheer from all present. Unfortunately, this scene of aural awakening is out of reach for many hearing-impaired children, particularly in developing countries [1]. Hearing is essential to learn language and speech and to develop cognitive skills. According to WHO, world wide approximately 350 million people have hearing disorder.
The performance of some moderately severe hearing-impaired adults and children using hearing aids is poorer than that of even profoundly hearing-impaired individuals using cochlear implants with advanced speech processing strategies. Individuals receiving marginal benefit from hearing aids were previously not considered to be candidates for implantation. Recent reports indicate that most marginally successful hearing aid users will have improved speech understanding with a cochlear implant [2]. The purpose of the present study on hearing-impaired children and adults was to identify appropriate candidates who are in need of cochlear implantation in Prayagraj and its surrounding areas.
Materials and Methods
This cross-sectional study was conducted on 95 hearing-impaired patients at tertiary health care centre in Prayagraj, Uttar Pradesh from August 2011 to July 2012. This study was approved by Institutional Ethical Committee and informed consent was signed by all patients or their legally acceptable relatives prior to the study.
Inclusion criteria: Patients from all age groups, with those below 17 years of age categorised as children and those above 17 years categorised as adult who had hearing impairement were included in the study.
Exclusion criteria: Patients who had mild to moderate hearing loss, unilateral hearing loss, any chronic pathology in middle or inner ear were excluded from the study.
The patients were further categorised into four groups; pre-lingual hearing-impaired children (30 cases), pre-lingual hearing-impaired adults (30 cases), post-lingual hearing-impaired children (15 cases) and post-lingual hearing-impaired adults (20 cases). A detailed history of all patients was taken, with particular reference to history of ear disease, ototoxic drug intake, history of diseases like meningitis, rubella, syphilis, any chronic illnesses like tuberculosis, diabetes, hypertension and any surgery. In case of children, detailed antenatal, natal and postnatal history was taken. Patients selected for study were given hearing aid trial for six months and were on regular follow-up. During these follow-up visits, patients were under auditory training and articulation therapy. After 6 months of hearing aid trial, patients were again assessed for hearing and speech development.
Free Field Audiometry (FFA)/Pure Tone Audiometry (PTA)
PTA/FFA was carried out by audiometer ELKON EDA 3N3 plus model with headphones both for air and bone conduction. This apparatus delivers pure tones at 125 Hz, 250 Hz, 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz 8000 Hz and 12000 Hz. This audiometer can deliver tones ranging from -20 dB to 120 dB.
Brainstem Evoked Response Audiometry (BERA)
The electric response audiometer model AMPLAID MK-10 with headphones having circumaural cushion and silver-silver chloride disc electrodes along with a conducting paste, was used for BERA. It was preferred that in assessment of young children, the patient was not hungry and the feed was given about 10-15 minutes before performing the procedure. Syrup trichlorphos (25 mg/kg body weight) was given half an hour before the procedure. BERA was performed using standard technique [3]. Stimulus was set at 2KHz frequency and rate of presentation was 11 clicks/sec. Intensity was adjusted at maximum and gradually dropped by 10 dB steps. 2000 samples were averaged at 0.2 micro volt/division sensitivity. For measurement of auditory threshold, the Vth wave’s latency and amplitude were measured. Both ears of the child were tested independently.
Speech Audiometry
Children aged 2 years and below lacks auditory skill development and were assessed by the Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS). This parent report scale is administered in an interview format. The parents were instructed that they will be asked a number of questions regarding their child’s responses to sound. The assessment is based on the parents’ response to 10 probes. The score is on a scale of 0 to 4 (0=never, 1=rarely, 2=occasionally, 3=frequently, and 4=always), resulting in a total possible point of 40 (10 questions, maximum score of 4 for each question). The IT-MAIS score at each assessing interval for every child is transformed into a percentage (total score/40x100) [4]. In children above 2 years, speech discrimination scoring was done by Lexical Neighbourhood test. The Lexical Neighbourhood/Multisyllabic Lexical Neighbourhood Tests (LNT-MLNT) were developed primarily for use with cochlear implant children. The LNT-MLNT was developed along theoretically motivated current models of spoken word recognition in listeners with hearing impairment. The development of the LNT-MLNT was based on the assumptions of the Neighbourhood Activation Model (NAM), which proposes that words are organised into similarity neighbourhoods based on their frequency of occurrence in the language and the number of phonemically similar words, or neighbours, within the lexical neighbourhood.
A dense lexical neighbourhood contains many phonemically similar words, whereas a sparse lexical neighbourhood has few phonemically similar words. Words that occur often and come from sparse lexical neighbourhoods are easier for children to identify than words with the opposite lexical characteristics [5]. In adults, open-set sentence tests Hearing in Noise Test (HINT) was done for evaluating speech discrimination scores. The HINT was developed to provide a reliable and efficient measure of speech recognition thresholds for sentences in quiet and in noise. The HINT stimuli consist of 250 digitally recorded sentences organised into 25 phonemically balanced lists of 10 sentences. The HINT is an adaptive speech test. That is, the difficulty of the test is adjusted to the ability of the subject by varying the presentation level in quiet or the signal-to-noise ratio in noise. This means that as cochlear implant technology improves, with even greater levels of speech recognition performance, the implant patient can always be tested with the HINT [6]. All tests were performed in the auditory-only listening condition using live voice presentation and were administered by a speech therapist experienced in controlling the intensity of his voice at 70-75 dB. The tests were administered live-spoken without lip-reading at a presentation level of 70 dB Sound Pressure Level (SPL). Live-voice instead of recorded speech was used to ensure flexibility so that the child’s attention could be kept as sharp as possible.
After six months of hearing aid use, hearing threshold and speech discrimination scores were estimated. Patients who did not benefit significantly from hearing aid were considered as candidates for cochlear implantation.
Statistical Analysis
Data management and statistical analysis were carried out using SPSS for Windows (version 17.0; SPSS, Chicago, IL, USA). For comparison of categorical variables, the Chi-square test or the Fisher’s-exact test was used, as appropriate. A p-value <0.05 was considered statistically significant.
Results
The age and sex distribution of pre-lingual children and adults in the present study shows maximum number of cases in age group ≤10 years, 35.5% were males and 55.1% were females were part of this age group [Table/Fig-1]. Male to female ratio of pre-lingual group was 1.1:1. And in case of post-lingual hearing-impaired children and adults’ maximum number (13) were in age group >50 years, 69.2% males and 30.8% females [Table/Fig-2]. Male and female ratio of post-lingual group was 1.9:1.
Age and sex distribution of pre-lingual children and adults.
| Age (in years) | No. of cases | Total (%) |
|---|
| Males | Females |
|---|
| ≤10 | 11 (35.5%) | 16 (55.1%) | 27 |
| 11-20 | 4 (13%) | 5 (17.2%) | 9 |
| 21-30 | 8 (25.8%) | 3 (10.3%) | 11 |
| 31-40 | 2 (6.5%) | 4 (13.8%) | 6 |
| 41-50 | 3 (9.7%) | 0 | 3 |
| >50 | 3 (9.7%) | 1 (3.4%) | 4 |
| Total | 31 | 29 | 60 |
| Mean Age | 21.72±17.95 | 15.22±14.67 | |
Age and sex distribution of post-lingual children and adults.
| Age (in years) | No. of cases | Total (%) |
|---|
| Males | Females |
|---|
| ≤10 | 6 (100%) | 0 | 6 |
| 11-20 | 4 (44.4%) | 5 (55.6%) | 9 |
| 21-30 | 1 (33.3%) | 2 (66.7%) | 3 |
| 31-40 | 1 (50%) | 1 (50%) | 2 |
| 41-50 | 2 (100%) | 0 | 2 |
| >50 | 9 (69.2%) | 4 (30.8%) | 13 |
| Total | 23 | 12 | 35 |
| Mean age | 35.03±23.15 | 33.13±22.18 | |
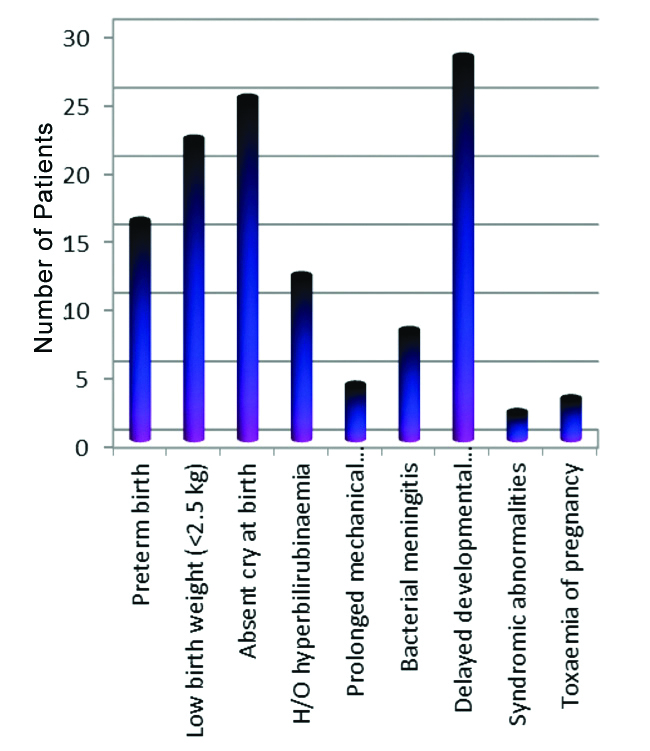
In the present study, 60 pre-lingual hearing-impaired patients were taken and among them 20% had positive family history of deafness. Out of these, two patients had Waardenburg syndrome. Delayed development of milestones was the most common co-morbid condition found along with hearing loss, the occurrence being in 28 (46.7%) cases. The other probable causes of impaired hearing were absence of cry at birth due to perinatal hypoxia in 25 (41.6%) cases, low birth weight in 22 (36.6%) patients, preterm birth in 16 (26.6%) cases, hyperbilirubinemia in 12 (20%) cases, bacterial meningitis in 08 (13.3%) cases, prolonged mechanical ventilation in 04 (6.6%) cases, toxemia of pregnancy in 03 (5%) patients and Waardenburg syndrome in 02 (3.3%) cases [Table/Fig-3]. In post-lingual hearing-impaired, 5.7% had positive family history. The most common cause of post-lingual hearing impairment was ototoxicity seen in 14.3% cases followed by pyogenic meningitis in 11.4% cases.
Distribution of probable causes of hearing impairment in pre-lingual group (N=60)
Among 16 patients with absent response in BERA, 15 (93.75%) were suitable for cochlear implantation and among 79 cases with response present in BERA, 33 (41.8%) were suitable candidates for cochlear implantation. The calculated difference between the two groups was statistically significant [Table/Fig-4]. Among pre-lingual hearing-impaired children, ten children were with absent response in BERA, nine (90%) were suitable for cochlear implantation and in 20 patients who showed response in BERA, five (25%) were eligible for cochlear implantation. Among pre-lingual hearing-impaired adult patients, six patients were with absent response in BERA, all (100%) were suitable for cochlear implantation and among 24 patients who showed response in BERA, 20 (83.3%) fulfilled the criteria for cochlear implantation. All patients in post-lingual groups showed response in BERA.
Absent response in BERA and suitability for cochlear implant (N=95).
| Responses | Suitable for cochlear implant | Not suitable for cochlear implant | Total | p-value |
|---|
| Response absent | 15 (93.75%) | 1 (62.5%) | 16 | <0.05 |
| Response present | 33 (41.8%) | 46 (58.2%) | 79 |
| Total | 48 | 47 | 95 | |
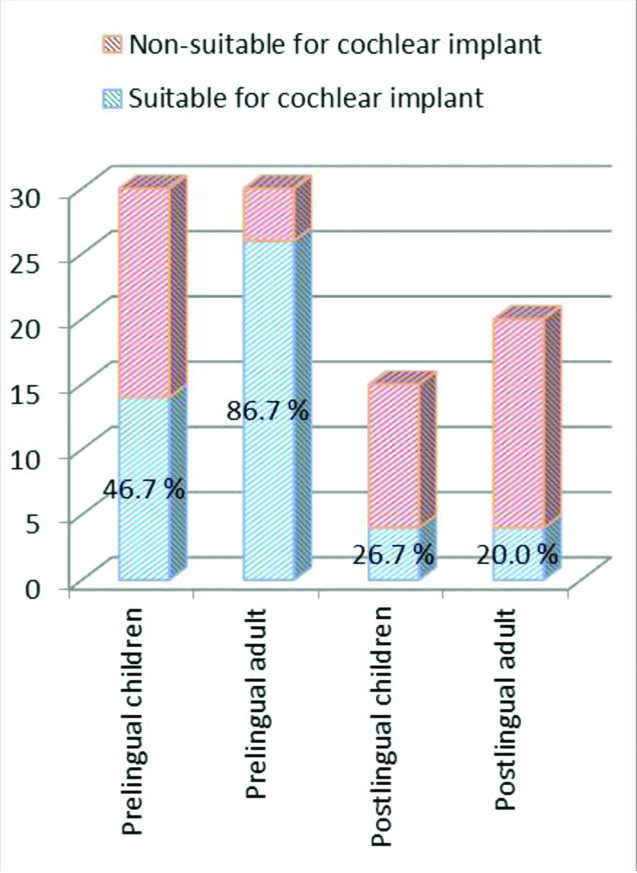
A total of 48 out of the 95 cases were found to be suitable for cochlear implantation, which constituted 50.5%. The highest percentage of cases fulfilling the criteria for cochlear implantation were in the pre-lingual hearing-impaired adults’ group, followed by pre-lingual children and post-lingual children whereas, only 20% of post-lingual adults were found suitable for cochlear implantation [Table/Fig-5].
Number of cases suitable for cochlear implant.
 |
|---|
| Study group | No. of cases suitable for cochlear implantation | Percentage (%) |
|---|
| Pre-lingual children (n=30) | 14 | 46.7 |
| Pre-lingual adults (n=30) | 26 | 86.7 |
| Post-lingual children (n=15) | 04 | 26.7 |
| Post-lingual adults (n=20) | 04 | 20.0 |
| Total (n=95) | 48 | 50.5 |
Discussion
Development of cognitive skills, speech and language needs reasonable hearing. Approximately, 350 million people are suffering from hearing disability worldwide. Hearing impairment accounts for 4.7 percent of total Years Lived with Disability (YLD), making it second most common cause of YLD. Deafness cases are disproportionately high in the South-east Asia region with a prevalence ranging from 4.6% to 8.8% [4].
The sex wise distribution of cases in both the pre-lingual and post-lingual groups was almost uniform. The sample taken in the study did not have a statistically significant gender bias. In present study, number of males (56.8%) outnumbered females (43.2%). Bubbico L et al., found 78 cases per 1000 males and 69 cases per 1000 females (p<0.001) in their study [7]. A study done by Agrawal Y et al., shows 5.5-fold higher hearing loss in men as compared to women and similarly, Ries PW found that the overall prevalence for males is 10.5 percent while 6.8 percent for females [8,9]. In the present study, 60 pre-lingual hearing-impaired patients were evaluated and among them 20% had positive family history of deafness. Out of this, two patients had Waardenburg syndrome. In post-lingual hearing-impaired, 5.7% had positive family history. Dereköy FS, in their study found that 28.3% patients had positive family history amongst 130 pre-lingual hearing-impaired patients they included in their research. According to a study conducted by da Silva LP et al., out of 53 pre-lingual hearing-impaired cases, 9% had positive family history. Calhau CM et al., states that 10% cases of pre-lingual hearing-impaired had hereditary deafness out of 200 [10-12]. A 23% cases of deafness were due to hereditary cause in a study conducted by Das VK [13]. Fortnum H and Davis A, showed 41% of cases had genetic aetiology [14]. Ozturk O et al., studied 840 pre-lingually deaf children and found 429 (51.1%) cases had genetic association for deafness [15]. A study conducted by Rajput HB et al., had 8 (32%) out of 25 patients with positive family history of hearing loss [16]. Ito T et al., found that more than 50% of pre-lingual hearing loss cases are found to be hereditary [17]. Thus, it can be concluded that pre-lingual hearing-impaired patients have more chances of positive family history of deafness.
In present study, patients after initial evaluation were put on hearing aid use for 6 months. Pre-lingual children had more improvement in speech discrimination score after hearing aid use than pre-lingual adults. According to Fukuda S et al., pre-lingually hearing-impaired pediatric hearing aid users with average pure-tone thresholds less than 90 dB Hearing Loss (HL) demonstrated generally better monosyllable speech perception test in more than 70% patients [18]. In present study, widely dispersed speech perception was observed within the 90-99 dB HL hearing-aid user group with most subjects demonstrating less than 50% speech perception. In the cluster of >100 dB HL, few cases demonstrated more than 50% of speech perception. This improvement in speech is not so in cases of pre-lingual adults as they have passed sensitive period of early childhood when central auditory system matures. Post-lingual children and adults have better outcome with hearing aid than the pre-lingual children and adults as post-lingual developed their speech and language skills earlier in life.
Wiley S and Meinzen-derr J, studied on children who were five years of age and younger having moderately-severe or worse sensorineural hearing loss. Out of 105 cases, 69% were referred for a cochlear implant [19]. A study done on 147 children by Edwards LC with mean age of 5.25 years and the mean duration of profound deafness of 4.38 years. A 48% were males and 52% were females and the mean hearing threshold over the frequencies 500-4000 Hz was 78.8 dB. Every child was made to use hearing aid consistently for a month prior to decision regarding implantation. Thirteen percent of the children were found to have acquired deafness through meningitis while 58% were congenitally deaf with unknown aetiology. A 93 (63%) children were found to be eligible for cochlear implantation [20].
Lazaridis E et al., assessed 121 children with 63 (52%) males and 58 (48%) females for the assessment of cochlear implantation [21]. Several aetiologies were identified as the probable cause of the sensorineural hearing loss. A 62% children were congenitally deaf, 17% had structural inner ear anomalies, 8% had genetic factors, 5% congenital infections and rest 2% had history of meningitis as probable causes of hearing loss. An 87 (71.9%) cases were considered suitable for cochlear implantation. Similarly, Edwards LC et al., found (82.6%) children suitable for cochlear implantation in their study [22].
Chute PM concluded that the speech perception ability of candidate when using appropriate amplification is most important factor during the evaluation for a cochlear implant. Cochlear implant guidelines suggest there be a “lack of benefit from hearing aid” to qualify as a candidate [23]. From the above study, it is clear that prior to cochlear implantation hearing aid trial for six months is important. Patients having little or no benefit are good candidates for cochlear implantation. In present study, only 26.7% post-lingual children and 20% of post-lingual adults were found fit for cochlear implantation most probable reason being that post-lingual patients have good speech discrimination with hearing aid.
A comparison of mean speech discrimination score was done before and after hearing aid use for six months in post-lingual children and adults in present study and it was observed that the mean speech discrimination score before hearing aid use was 33.8 and 42.7, respectively and that of after six month of hearing aid use was 57.53 and 68.75, respectively. Criteria for candidacy of cochlear implantation given by Wackym PA and Runge Samuelson CL, states that aided scores on open-set sentence tests of less than 50% suggest need of cochlear implantation [24]. This score was not attained by 26.7% post-lingual children and 20% post-lingual adults; hence they were suitable for cochlear implantation.
In present study, the pre-lingual hearing-impaired adults had the largest number of cases (86.7%) followed by pre-lingual hearing-impaired children (46.7%), suitable for cochlear implantation. Mean speech discrimination score before hearing aid use in pre-lingual children and adults was 7.38 and 7.26, respectively. The mean speech discrimination score after hearing aid use was 18.98 and 10.63 in pre-lingual children and adults respectively. According to criteria for candidacy of cochlear implantation given by Wackym PA and Runge Samuelson CL, minimal benefit from hearing aids, defined as less than 20% to 30% on single syllable word test, or in case of younger children, lack of developmentally appropriate auditory milestones measured using parent report scale [24]. A 46.7% pre-lingual children and 86.7% adults meet the above-mentioned criteria for cochlear implant candidacy; hence these patients were suitable for cochlear implantation.
According to a study conducted by Garg S et al., 6.3% of Indian population suffers from significant auditory loss, among which 32% have profound hearing loss and 39% have severe hearing disability [25]. Thus, the number of cases with hearing impairment is expected to be 375,126 of which 266,339 were estimated to have severe to profound hearing loss in Prayagraj district which has a population of 5,954,391 [26]. According to the present study, this amounts to 134,501 cases which are in-need of cochlear implantation in Prayagraj district.
Limitation(s)
As it is a single centered study and sample size is also very small so, the results of this study may not exactly represent the need of cochlear implants in the given population.
Conclusion(s)
A 50.5% of severe to profoundly hearing-impaired patients were found to be suitable for cochlear implantation. The pre-lingual hearing-impaired children and adults are more suitable for cochlear implantation than the post-lingual hearing-impaired children and adults. Approximately, 134,501 cases were estimated to be, in need of cochlear implantation in Prayagraj district (estimated using census 2011). These figures call for further studies in other centers so that input is provided to public health policy makers in order to establish facilities for cochlear implantation in the region. Further, multicentric studies with larger sample size are needed to accurately access the need of population.