Playing online games has become a most popular leisure activity in many parts of the world, which has harmful effect on health, especially students. The World Health Organisation (WHO) has enlisted it as a mental health condition. Some computer-related and vision-related researches have measured the physical and ocular effects and binocular vision separately [1]. India has second largest number of users of cell phones. In India, few studies conducted to assess its impact on health [2]. Presently, the incidence of internet gaming disorder among the adolescent group was between 1.3% to 19.9% [3]. Video games addiction is a condition in which the person is desire to play video games. It may influence day to day life activities of the person, as well as low performance in school, being unable to fulfill the job demands and interrupted in family relationship. According to WHO, gaming disorder is diagnosed after period of at least twelve months, but early in case of severity in signs and symptoms. In 2018, WHO identified that video games addiction as a big problem and has been placed under International classification of diseases 11 (ICD 11) disorders due to substance use addictive behaviour with a code 6C51 [4]. Gaming disorder may develop physical problems such as severe headache, tiredness, cervical spondylosis induced by poor neck control, blurry vision, dry eyes, early diagnosed as a cataract, discomfortness in wrist joint and interphalangeal joints linked to gaming addiction, neurological dysfunction, mental disorders such as bipolar disturbance, psychiatric illnesses like mood disorder, anxiety, cravings for gaming, pilferer and lack of interest for doing other activity [5]. Researchers found that over use of playing computer games alters eye function and causes ocular and physical problems. They found that further understanding of the adverse effects of over use of computer on physical and ocular health hence adequate breaks are important to prevent physical and visual problems while playing computer games [1].
Computer vision disorders are the main health problem because of excessive use of computer. Headache or eye strains, double vision, blurry vision, eye redness are triggered after long hour’s use of the computer. A 70% of excessive computer users may develop computer vision problems [6]. Adolescent’s attraction to the net games cause many mental, physical, and social problems for them. These can cause unit stimulating anger and violence, obesity, epilepsy, social isolation and different physical and mental damages. Many psychologists and condition professionals have paid attention to the results of these games [7]. A case report showed that PlayStation thumb is also health problem due excessive playing of video games. PlayStation thumb is, characterised by numbness and a blister is caused by friction between the thumb and the controller from fast and continuous playing games [8]. Hence, present study was conducted with an aim to determine the effectiveness of self-instructional module on knowledge regarding vision hazards while playing online games among junior college students.
Materials and Methods
A pre-experimental pre-test, post-test research design was used to conduct this study. The data gathering method began from 23rd December to 28th December 2019 and the setting was selected in the New English Junior College, Wardha, Maharashtra, after getting Ethical permission (Ref. No.: DMIMS(DU)/IEC/Sept-2019/8494). By using a purposive sampling technique, 100 junior college students were selected based on the calculation:
Where, n=sample size, Zα is the level of significance at 5% i.e., 95% Confidence Interval (CI)=1.96, p=prevalence=desired error=7%
Standard normal variate, which is 1.96 at 5% type 1 error, SD=standard deviation of knowledge score, d=desired error. P=prevalence, p-values are considered significant below 5%, hence, 1.96 is used in formula. Considering, 95% CI and 20% allowable error, the sample size was calculated to include 123 respondents. However, due to logistic reasons the researchers restricted to include 100 junior college students (11th standard students because during data collection 12th standard junior college students were on preparatory leave and they were not present in the class so that researcher selected 11th standard students only).
The junior college students (11th standard students) were informed and explained the objective of the study. The written informed consent duly signed individually by them was obtained.
Inclusion criteria: Junior college students who can read and understand English, and who gave consent for participation in the study, and who were aged between 17 and 19 years, and included male and female adolescents. (12 standard students also enrolled but not present during data collection).
Exclusion criteria: Those who had participated in similar type of research and who were not available at the time of data collection.
It was assumed that may have some knowledge regarding vision hazards while playing online games.
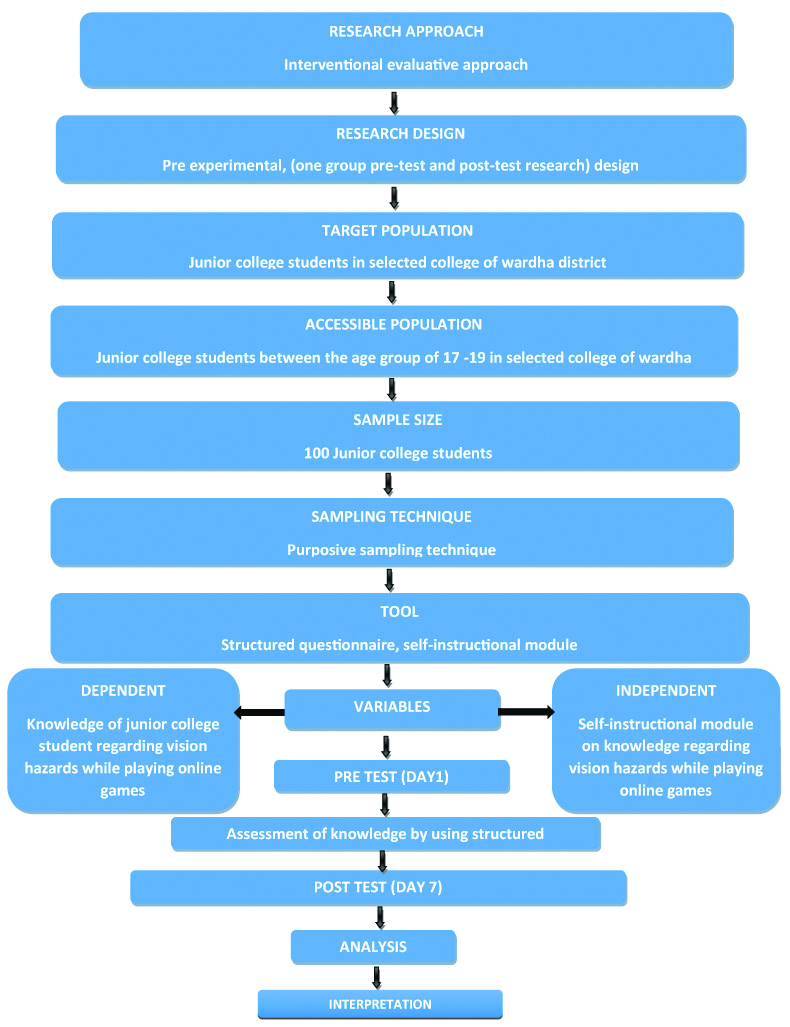
Demographic variables were collected in terms of gender, location of residence, family income, type of device, type of game, time spend on social media, online games affecting them, restless or trouble and parents are aware about activity. A structured questionnaire which is attached in [Annexure1], has16 multiple choice questions were used. The sections were: (i) meaning and causes of online gaming disorder; (ii) disadvantages and health risk problems of online gaming disorder; and (iii) and prevention of gaming disorder. Each correct answer carried one mark and the total score was 16. The prepared tool was validated by 10 experts who included two from departments of statistics, one each from department of English, department of general medicine, department of respiratory medicine and five from department of medical surgical nursing. Parallel form method was adopted for reliability test and it was found as r=0.8962. And hence, tool was reliable and valid. The data collection process was planned to gather demographic information and the knowledge regarding vision hazards while playing online games. The self-instructional module as organised on: (i) meaning and causes of online gaming disorder with image; (ii) disadvantages and health risk problems of online gaming disorder with image; and (iii) and prevention of gaming disorder. There were two sessions conducted for education in two groups, each session had 50 students in each group in 45 minutes. Each sample required mean time of 30 minutes to complete the pre-test structured questionnaire. Then the self-instructional module was intervened to the sample. The post-test structured questionnaire was administered after seven days. Based on the 16 questions, each study participant was asked individually for his/her answers with the same questionnaire. As collected, the responses were arranged in tabular form to conduct statistical analyses which are mentioned in the following sections [Table/Fig-1].
Schematic representation of research design for the study.+
Statistical Analysis
The collected data were coded, tabulated, and analysed by using descriptive statistics (mean percentage, standard deviation) and inferential statistics. Significance difference between pre and post-test readings was tested by using t-test; association of knowledge with demographic variables was done by one-way ANOVA test and independent t-test. For statistical analysis Statistical Package for the Social Sciences (SPSS) version 16.0 was used. The p-value less than 0.05 considered as significant.
Results
Association of knowledge with their demographic variables are depicted in [Table/Fig-2]. It showed that majority of the 66 (66%) junior college students were females. The majority of the 50 (50%) junior college students belonged to an urban area. Majority of the 34 (34%) junior college students had monthly family income of 40001-50000 Rs. Majority of the 79 (79%) junior college students were using mobile. Majority of the 21 (21%) junior college students were playing PUBG and 66 (66%) junior college students of them were playing other game. Majority of the 68 (68%) junior college students were spending less than one hour on social media. Majority of the 37 (37%) junior college students replied that online game does not affect me too much. Majority of the 36 (36%) junior college students never troubles while playing online game and 37 (37%) junior college students sometimes troubles while playing online game. Majority of the parents 41 (41%) of junior college students were completely aware about playing online games.
Association of knowledge with their demographic variables.
| Demographic variable | Frequency (N=100) | Post-test knowledge Mean±SD | F-value/t-value | p-value |
|---|
| Gender |
| Male | 34 | 15.61±0.69 | 0.02 | 0.97 p>0.05 |
| Female | 66 | 15.62±0.51 |
| Area of residence |
| Urban | 50 | 15.62±0.63 | 0.52 | 0.66 p>0.05 |
| Rural | 34 | 15.55±0.56 |
| Semi Urban | 14 | 15.71±0.46 |
| Slum | 2 | 16±0 |
| Monthly family Income (Rs) |
| 30000-40000 | 22 | 15.63±0.49 | 0.40 | 0.75 p>0.05 |
| 40001-50000 | 34 | 15.58±0.60 |
| 50001-60000 | 22 | 15.54±0.73 |
| 60001 and above | 22 | 15.72±0.45 |
| Device using while playing online game |
| Mobile | 79 | 15.60±0.60 | 0.05 | 0.98 p>0.05 |
| TV | 6 | 15.66±0.51 |
| Laptop | 12 | 15.66±0.49 |
| Computer | 3 | 15.66±0.59 |
| Type of game playing |
| PUBG | 21 | 15.71±0.46 | 0.04 | 0.98 p>0.05 |
| Call of duty | 8 | 15.25±1.03 |
| Rummy | 5 | 16±0 |
| Other | 66 | 15.60±0.55 |
| Number of hours |
| <1 h | 68 | 15.63±0.51 | 0.04 | 0.98 p>0.05 |
| 1-3 h | 19 | 15.57±0.83 |
| 3-6 h | 8 | 15.62±0.51 |
| >6 h | 5 | 15.60±0.54 |
| Does online game affects you |
| Does not affect me too much | 37 | 15.54±0.69 | 1.25 | 0.29 p>0.05 |
| Partially affect | 8 | 15.37±0.74 |
| Affects a lot | 25 | 15.76±0.43 |
| Disturb my daily routine | 30 | 15.66±0.47 |
| Restless or trouble |
| Never | 36 | 15.41±0.73 | 2.71 | 0.049 p<0.05 |
| Very rarely | 20 | 15.70±0.47 |
| Sometimes | 37 | 15.78±0.41 |
| Always | 7 | 15.57±0.53 |
| Awareness of parents |
| Completely aware | 41 | 15.63±0.48 | 0.24 | 0.86 p>0.05 |
| Partially aware | 24 | 15.63±0.71 |
| Not aware | 27 | 15.55±0.64 |
| Allow to play | 8 | 15.75±0.46 |
p-value less than 0.05 considered as significant
There was only one significant association between knowledge scores of junior college students with their demographic variable i.e., restless or trouble (p=0.049, p<0.05) and rest of all other demographic variables were not associated with (p>0.05) knowledge score of junior college students i.e., gender, location of residence, monthly family income, type of device, type of game, time spend on social media, online games affects you, parents are aware about activity.
The above [Table/Fig-3] showed that in post-test all knowledge structured questionnaires score improved than the pre-test after giving intervention.
Analysis of knowledge structured questionnaires.
| Questions | Pre-test | Post-test | p-value |
|---|
| What is meaning of online game? | 76% | 100% | <0.001 |
| What is meaning of addiction? | 56% | 100% | <0.001 |
| Which one of the following cause for attracting adolescence towards online game? | 54% | 98% | <0.001 |
| Which one of the communication may reduce while playing online game? | 37% | 98% | <0.001,S |
| Which one of the bad affect occurs due to online games? | 47% | 98% | <0.001 |
| Which one of the factors responsible for increase addiction towards online games among adolescence? | 42% | 97% | <0.001 |
| Which one of the following Health risk occurs while playing online games? | 36% | 96% | <0.001 |
| Which effect occurs on family because of frequently playing online games? | 46% | 93% | <0.001 |
| Which organ of the body affected directly while playing online game? | 52% | 96% | <0.001 |
| Why vision problem occur while playing online games? | 39% | 94% | <0.001 |
| Which part of the body absorbs the radiation emitted while playing online games? | 40% | 99% | <0.001 |
| What are the one of the most physical illnesses existing while playing online games? | 51% | 97% | <0.001 |
| Which symptom seen while extensive viewing of the screen? | 62% | 100% | <0.001 |
| Which month Gaming disorder should be diagnosed? | 41% | 99% | <0.001 |
| While playing online game screen brightness should be | 45% | 97% | <0.001 |
| How to protect yourself while playing online games? | 58% | 100% | <0.001 |
p-value less than 0.05 considered as significant
The above [Table/Fig-4] showed that 1% of junior college students had poor knowledge scores, 67% had average knowledge scores, and 32% had good knowledge scores in the pre-test. Minimum knowledge score in pre-test was two and maximum knowledge score in pre-test was 12. Mean knowledge score in pre-test was 7.82±1.88 and mean percentage of knowledge score in pretest was 48.87±11.79.
Analysis of knowledge structured questionnaires; N=100.
| Level of pre-test knowledge | Score range | Pre-test level knowledge score |
|---|
| No of junior college students |
|---|
| Poor | 1-4 | 1 |
| Average | 5-8 | 67 |
| Good | 9-12 | 32 |
| Excellent | 13-16 | 0 |
| Minimum score | 2 |
| Maximum score | 12 |
| Mean knowledge score | 7.82±1.88 |
| Mean percentage knowledge score | 48.87±11.79 |
The above [Table/Fig-5] showed that 100% of the college students were having excellent level of data score in post-test. Minimum knowledge score in post-test was 13 and maximum knowledge score in post-test was 16. Mean knowledge score in post-test was 15.62±0.58 and the mean percentage of post-test knowledge was 97.62±3.63.
Assessment with level of post-test knowledge (N=100).
| Level of post-test knowledge | Score range | Level of post-test knowledge score |
|---|
| No of junior college students |
|---|
| Poor | 1-4 | 0 |
| Average | 5-8 | 0 |
| Good | 9-12 | 0 |
| Excellent | 13-16 | 100 |
| Minimum score | 13 |
| Maximum score | 16 |
| Mean knowledge score | 15.62±0.58 |
| Mean percentage knowledge score | 97.62±3.63 |
The effectiveness of self-instructional module was analysed as follows:
The mean value of the pre-test is 7.82 and the post-test is 15.62 and the standard deviation values of pre-test are ±1.88 and post-test is ±0.58. The calculated t-value is 39 and the p-value is <0.001 [Table/Fig-6]. Hence, it was statistically interpreted that the self-instructional module on knowledge regarding vision hazards while playing online games among junior college students was helpful. Thus, the H 1 is accepted and H 0 is rejected in this research.
The significant difference between the pre-test and post-test knowledge of junior college students (N=100).
| Overall | Mean | SD | Mean difference | t-value | p-value |
|---|
| Pre-test | 7.82 | 1.88 | 7.80±2.00 | 39 | <0.001p<0.05 |
| Post-test | 15.62 | 0.58 |
SD: Standard deviation; p-value less than 0.05 considered as significant
Discussion
Present study was conducted to evaluate the effectiveness of self-instructional module on knowledge regarding vision hazards while playing online games among junior college students. It intends to promote junior college students knowledge regarding vision hazards while playing online games. The mean value of the pre-test is 7.82 and the post-test is 15.62 and the standard deviation values of pre-test are ±1.88 and post-test is ±0.58. The calculated t-value is 39 and the p-value is <0.001. Hence, it is statistically interpreted that the self-instructional module on knowledge regarding vision hazards while playing online games among junior college students was helpful. Similarly, a pre-experimental study conducted on to assess the effectiveness of video teaching on knowledge regarding health hazards of electronic devices among adolescence. The statistical analysis revealed that, the ‘t’ value for knowledge was (t=9.304), this indicates the significant difference between the pre and post-test levels of knowledge at 0.05 level of significance, the video teaching on knowledge regarding health hazards of electronic devices among adolescence was effective [9].
Present study found that playing online games are associated with restlessness and trouble=2.71, p=0.049 (S, p<0.05) and Similarly, one cross-sectional study conducted in Kottakuppam, a town panchayat in Villupuram district of Coastal Tamil Nadu, Southern India found that usage of mobile phones are associated with health problems. There was association between mobile phone usage and selected health problems. The prevalence of health problems was significantly higher in the mobile phone users when compared to non-users. After adjusting the confounding factors using multivariate logistic regression, it was found that all the health problems had positive association with mobile phone usage except hypertension [2]. The present study illustrated one group pre-test and post-test research design among 100 junior college students in which majority of the students were from urban i.e., 50%, from rural 34%, from semi urban 14%, and from slum area 2%. In another cross-sectional study on prevalence of internet gaming disorder, in India, a technological hazard among adolescents in which residence of majority of the study participants with Internet Gaming Disorder (IGD) was from urban area i.e., 86% whereas the rest 14% were from rural area [3].
A similar study conducted by faculty of medicine on the topic “awareness of cell phone hazards among university students in a Malaysian medical school” and this paper seeks to examine the awareness of potential health hazards by using mobile phone among AIMST (Asian Institute of Medical Sciences and Technology) university students. A cross-sectional study conducted by circulating questionnaire on ‘perception. Researcher compared perceptions of dangers to well-being and outcomes by gender, age, study course, chosen year, number of regular calls and daily massages, cell phone brand and mobile phone accessory usage (bluetooth and band-free). In AIMST university, student’s overall perception of cell phone dangers was 62%. Most respondents accepted that use of cell phones can cause headache, mental loss of concentration, and sleep disturbances, although most disagree that use of mobile phones can cause constipation although diarrhoea. Out of the 124 subjects who were knew about the side effects of cell phone, 5% males and 10% females felt that there was no need to mitigate any undesirable effects. This study is useful for the general public, especially for the students as the perceived health risk did not detect students using cell phones significantly. In spite of their awareness of the associative hazards, the reasons given by students for continued use of mobile phone were discussed. This research provides new insight into the level of understanding and interpretation among university students of cell phone hazards [10].
A research study concluded that cell phones are used by every person at their work places. This study specialises in the health effects of telephone usage amongst students following skilled courses in schools in an urban setting, school students of each sexes in the age group of 17-19 years from urban and rural backgrounds. They got self-administrated, pre-tested form including aspects associated with few common adverse mental and physical health symptoms attributed to mobile phone usage [11].
Limitation(s)
The study was limited to sample size i.e., 100, which might be inadequate to generalise the study findings. More time duration would give more relevant results with variations of any research, but the investigator planned to complete the research work within one week to get more feasibility of getting sample. Therefore, sufficient number of sample and time duration was required to establish the effect of structure instructional module, in general.
Conclusion(s)
Study concluded that knowledge regarding vision hazards while playing online games has been improved after administering Self Instruction Module (SIM) among junior college students. There was a significant association of knowledge score in relation to restless or troubles while playing online game. There was no significant association of knowledge score in relation to gender, location of residence, family income, type of device, type of game, time spend on social media, online games affecting them and parents are aware about activity.
p-value less than 0.05 considered as significant
p-value less than 0.05 considered as significant
SD: Standard deviation; p-value less than 0.05 considered as significant