Preservation of health and integrity of tooth structure is of primary importance in paediatric dentistry [1]. However, complicated occlusal morphology of permanent molars makes them highly susceptible to dental caries [2,3]. Caries preventive effect of fluoride is primarily on smooth surfaces and proximal areas [4]. Nevertheless, the occlusal pits and fissures most susceptible to dental caries are least affected by fluoride [4]. As a result, PFS have become the most effective non invasive strategy to prevent and/or arrest occlusal caries in children with high caries risk and teeth with deep, retentive pits and fissures [5]. They relish wide acceptance as a preventive strategy in paediatric dentistry. PFS is a chemically-active liquid material, which is introduced into the occlusal pits and fissures of the caries-susceptible tooth, which forms a protective layer with micro-mechanical bond, thus preventing access to cariogenic bacteria, from the oral environment [6,7]. However, their effectiveness may be precluded by technical problems during the application, such as salivary contamination and improper adhesion of the sealant to the tooth structure [8].
Other factors that mainly influence the retention of PFS are the stage of the tooth’s eruption, the behaviour of the patient, and the technique used for sealant application [9]. Furthermore, the success of sealant depends on the optimal conditions under which it is applied [10]. Therefore, isolation is a prime factor involved in sealant success. However, limited number of previously published studies have reported the influence of isolation method on sealant retention [9-11]. Therefore, the present study was planned to evaluate and compare the retention of PFS with either rubber dam or cotton roll in the FPM for a period of 12 months.
Materials and Methods
This prospective clinical trial was carried out in the Department of Paediatric and Preventive Dentistry at Narayana Dental College and Hospital, Nellore, Andhra Pradesh, India. Before the study was commenced, consent was obtained from the concerned school authorities and parents. The ethical clearance from Institutional Ethical Committee (Institutional Review Board) to conduct the clinical trial (D148407049) was obtained. Healthy, co-operative children in the age group of 6-9 years were included.
Inclusion and Exclusion criteria: One hundred PFMs from 25 children were chosen for the sealant application based on the predefined inclusion and exclusion criteria. Children who required sealants in all four PFM, with fully erupted PFMs that allow retention of clamp during rubber dam placement, with no clinical or radiographic evidence of proximal caries, with adequate oral hygiene {simplified Oral Hygiene Index (OHI-S)} score of 0 to 1.2 [12], and Frankl behaviour rating of 3 and 4 (co-operative children) [Table/Fig-1] [13] were included in the study. Exclusion criteria were molars with developmental anomalies (hypoplasia, fluorosis), stained fissures, frank carious (cavitated) lesions, or previously restored teeth and molars where isolation was not possible.
Frankl behaviour rating scale [13].
| Rating | Behaviour |
|---|
| 1 | Definitely negative. Refusal of treatment, forceful crying, fearfulness, or any other overt evidence of extreme negativism. |
| 2 | Negative. Reluctance to accept treatment, uncooperative, some evidence of negative attitude but not pronounced (sullen, withdrawn). |
| 3 | Positive. Acceptance of treatment; cautious behaviour at times; willingness to comply with the dentist, at times with reservation, but patient follows the dentist’s directions cooperatively. |
| 4 | Definitely positive. Good rapport with the dentist, interest in the dental procedures, laughter and enjoyment. |
Sample size: Based on the previous studies [7,14,15], considering the retention rate as the primary outcome; a level of significance was set at 0.05 and power at 80%, a total sample size of 80 teeth was essential. Considering the dropouts, the sample size increased by 20 teeth, and 100 teeth were included in the study.
The four PFMs of recruited children were assigned into two groups under a split-mouth experimental design. Sealants were applied on the upper and lower PFMs of the right side using rubber dam isolation and left side using cotton roll isolation.
Group I (n=50 teeth): The sealant application was made with Helioseal F® (Ivoclar Vivadent Marketing Ltd., India) with rubber dam isolation.
Group II (n=50 teeth): The sealant application was made with Helioseal F® (Ivoclar Vivadent Marketing Ltd., India) with cotton roll isolation.
Procedure: After obtaining parental consent, fissure sealants were placed on the occlusal surfaces of PFMs. After oral prophylaxis, isolation was performed either using a rubber dam (Hygenic Coltene/Whaledent Inc., USA) in Group I or with cotton rolls (custom-made) in Group II. Each tooth was etched with 37% phosphoric acid (Prime Dental Products Pvt., Ltd., India) for 15 seconds, followed by rinsing thoroughly with air-water spray for 15 seconds as well as drying for 30 seconds [6] and change of cotton rolls after rinsing off the etchant in Group II. A dull frosty-white appearance confirmed the etching of the enamel surface. If salivary contamination had occurred, the surface was further re-etched for 5 seconds [15], rinsed, and dried. The bonding agent was applied using disposable micro-applicator tips and cured for 15 seconds [9]. This was followed by the application of sealants on the allocated PFMs. A probe was used to remove the air bubbles and ensure the sealant flow into all pits and fissures. All the sealants were photo-polymerised for 20 seconds according to the manufacturer’s instructions. The complete application of the sealant was confirmed by passing an explorer along the margins. All the sealants were applied during the same visit by a single operator. The patients were advised to refrain from eating or drinking for 30 minutes. Oral hygiene instructions [16] such as toothbrushing twice daily in the morning and after the last meal in the night, tongue cleaning and mouth rinsing were given.
Follow-up examination and evaluation of the sealants was performed by a second examiner who was blinded to the study groups. Intra-examiner reliability was assessed by the re-evaluation of 10% of the teeth after a one-week interval. All the children were evaluated for sealant retention at regular intervals of 3, 6, and 12 months using Simonsen’s criteria [Table/Fig-2] [8].
Simonsen’s criteria for evaluation of occlusal sealants [8].
| Rating | Evaluation criteria |
|---|
| Marginal integrity |
| 0 | Restorative material adjacent to the tooth and not detectable with an explorer |
| 1 | Margin detectable with the explorer |
| 2 | Crevice along the margin of visible width and depth |
| 3 | Crevice formation with exposure of central fissure |
| Marginal discolouration |
| 0 | No color change at the tooth-sealant interface |
| 1 | Discoloration noted along the margin in one area |
| 2 | Discoloration noted along the margin in multiple areas |
| 3 | Severe discoloration with evidence of penetration and leakage |
| Anatomic form |
| 0 | Harmonious and continuous with occlusal form and structure |
| 1 | Change in anatomic form but all pits and fissures covered |
| 2a | Loss of sealant from one or two pits or accessory grooves (partial loss), but no need to repair or replace sealant |
| 2b | Loss of sealants from pits or accessory grooves (partial loss), with a need for replacement or repair of the sealant |
| 3 | Loss of sealant from all pits (total loss) |
| 7 | Partial loss due to the occlusion |
| 9 | Bubble (not connected with the margins) |
Oral hygiene instructions were reinforced in each follow-up visit. However, the sealants were not reapplied if they had been lost between the examinations since teeth with partial or complete loss of sealant are not at high risk compared to unsealed teeth [17].
Statistical Analysis
The data collected were tabulated and subjected to statistical analysis using the SPSS statistical package (Version.17.0) with the level of significance set at 0.05. Any significant difference in the retention rates by using two different isolation techniques was analysed using the Chi-square test. The null hypothesis stated that there was no difference in the retention of sealants isolated with either rubber dam or cotton rolls in PFMs.
Results
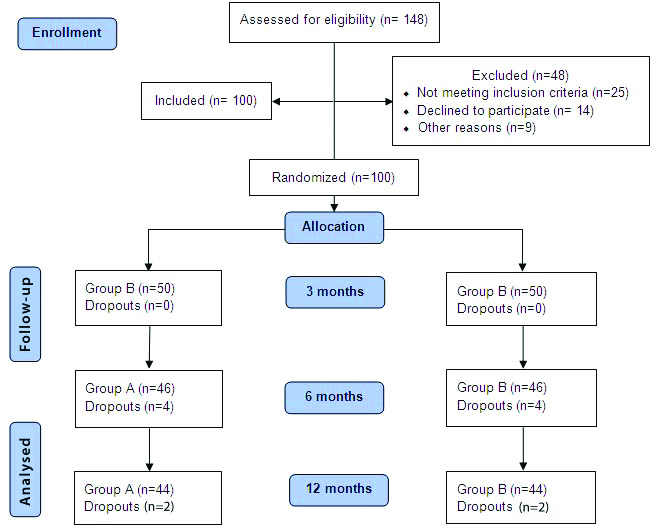
The total number of teeth assessed for eligibility, recruitment, randomisation, allocation, and numbers analysed were illustrated in the CONSORT flow diagram [Table/Fig-3]. A total of 100 PFMs (occlusal surfaces) from 25 children irrespective of gender were included in the study. In both the rubber dam and cotton roll isolation groups, 50 teeth were available for examination at 3 months, 46 teeth at 6 months, and 44 teeth at 12 months, respectively. The loss of the sample was due to migration to other places and change of the location leading to inaccessibility during follow-up.
CONSORT flow diagram of the study.
The marginal integrity rates for sealants with rubber dam isolation at 3, 6, and 12 months were 88%, 78%, and 75%, respectively. For sealants with cotton roll isolation, the marginal integrity rates at 3, 6, and 12 months were 76%, 70%, and 64%, respectively [Table/Fig-4].
Marginal integrity of the occlusal sealants in Group I and Group II on follow-up intervals.
| Follow-up | Teeth | Group I (Marginal integrity) | Group II (Marginal integrity) | p-value* |
|---|
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 |
|---|
| N | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
|---|
| 3 m | 50 | 44 (88) | 6 (12) | --- | --- | 38 (76) | 10 (20) | 2 (4) | --- | 0.11 (NS) |
| 6 m | 46 | 36 (78) | 10 (22) | --- | --- | 32 (70) | 10 (21) | 4 (9) | --- | 0.39 (NS) |
| 12 m | 44 | 33 (75) | 7 (16) | 4 (9) | --- | 28 (64) | 8 (18) | 6 (14) | 2 (4) | 0.30 (NS) |
*Chi-square test; NS: Not significant
The difference in marginal discolouration of the sealants in Group I and Group II were not statistically (NS) significant. In Group I, the percentage for no color change in sealants in with rubber dam isolation at 3, 6, and 12 months were 96%, 89%, and 75%, respectively, whereas, in Group II with cotton roll isolation, the percentage for no color change were 90%, 85%, and 68%, respectively [Table/Fig-5].
Discolouration of the occlusal sealants in Group I and Group II on follow-up visits.
| Follow-up | Teeth | Group I (Marginal discolouration) | Group II (Marginal discolouration) | p-value* |
|---|
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 |
|---|
| N | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
|---|
| 3 m | 50 | 48 (96) | 2 (4) | --- | --- | 45 (90) | 5 (10) | --- | --- | 0.23 (NS) |
| 6 m | 46 | 41 (89) | 5 (11) | --- | --- | 39 (85) | 7 (15) | --- | --- | 0.61 (NS) |
| 12 m | 44 | 33 (75) | 11 (25) | | --- | 30 (68) | 14 (32) | --- | --- | 0.53 (NS) |
*Chi-square test; NS: Not significant
The retention of the sealant’s anatomic form with rubber dam isolation after 3, 6, and 12 months was 90%, 78%, and 71%, respectively. For the sealants with cotton roll isolation (group I and II), retention of anatomic form at 3, 6, and 12 months was 78%, 70%, and 64%, respectively [Table/Fig-6]. There was no statistically significant difference among the sealants in Group I and II evaluated concerning marginal integrity (p>0.05), marginal discoloration (p>0.05), and anatomic form (p>0.05) at all time intervals.
Anatomic form of the occlusal sealants changes in Group I and Group II on follow-up intervals.
| Follow-up | Group I (Anatomic form) | Group II (Anatomic form) | p-value* |
|---|
| Teeth | 0 | 1 | 2a | 2b | 3 | 7 | 0 | 1 | 2a | 2b | 3 | 7 |
|---|
| N | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
|---|
| 3 m | 50 | 45 (90) | 5 (10) | --- | --- | --- | --- | 39 (78) | 7 (14) | 4 (8) | --- | --- | --- | 0.10 (NS) |
| 6 m | 46 | 36 (78) | 8 (18) | 2 (4) | --- | --- | --- | 32 (70) | 9 (19) | 4 (9) | 1 (2) | --- | --- | 0.39 (NS) |
| 12 m | 44 | 31 (71) | 8 (18) | 3 (7) | 2 (4) | --- | --- | 28 (64) | 8 (18) | 2 (4) | 3 (7) | 3 (7) | --- | 0.54 (NS) |
*Chi-square test; NS: Not significant
Discussion
The diagnostic accuracy and digital radiographs for caries diagnosis play a significant role in treatment plan that whether to restore or seal the tooth [18,19]. Apart from the detection of carious lesions and to determine the extension in dentine is essential for the selection of restorative material [19]. Sealing the pits and fissures would prevent the occurrence of dental caries [20]. However, according to Buonocore MG, the sealants’ effectiveness is directly related to its micro-mechanical retention [21] and is primarily reliant on the method of application [22]. The traditional method of isolation is by using cotton rolls. Poor control of saliva, contamination during swallowing, and tongue movements are the disadvantages of cotton roll isolation [23,24]. Alternatively, isolation with rubber dam provides adequate moisture control necessary for the sealant placement; however, its application and effectiveness are influenced by the child’s co-operation level [14,25,26].
In the present study, two different isolation techniques were used in Group I and Group II. In the group with rubber dam isolation, the marginal integrity was higher (75%) compared to the group with cotton roll isolation (64%) at the end of 12 months. The results were better in Group I than in Group II, although there were no statistically significant differences with respect to the marginal integrity, discolouration, anatomical failure between the two groups. These findings are in agreement with the earlier studies reported by Eidelman E et al., and Albani F et al., [14,27]. Albani F et al., reported similar results with a rubber dam or cotton rolls, however, the retention rate was higher with rubber dam isolation [27]. The possible reasons for loss of marginal integrity could be patient behaviour, saliva control, operator skills, enamel alterations, patient age, time of placement, and maxillary or mandibular arch [9]. However, behaviour and moisture control were considered essential factors that influence sealant effectiveness [6,8]. Indeed, patients with poor behaviour cannot be well managed, and it is difficult to achieve proper moisture control in such patients [10,14]. Hence, we included only co-operative children with Frankl behaviour ratings of 3 and 4 in the current study [13]. Another study reported that the child’s preference on choosing the isolation method for dental treatment should also be given priority [28]. The authors concluded that the children preferred rubber dam over the saliva ejector and cotton rolls.
Salivary contamination during the application of sealant (both after etching and bonding procedures) is the main factor responsible for sealant failure [29,30]. According to Silverstone LM et al., contamination of etched enamel by saliva readily absorbs salivary constituents and leads to the formation of surface coatings that could not be removed by simple washing with water [30]. This causes surface changes and reduces surface energy that renders the surface less favourable for bonding, as it interferes with the bonding mechanism [31,32]. Unwashed, saliva contaminated etched enamel surface showed significantly reduced bond strength [25]. Furthermore, re-etching is needed for an extended time (5 and 15s) to achieve adequate bond strength [15]. Hence, proper isolation is an essential element in sealant retention and success. Eidelman E et al., considered a short etching time of 20 seconds [33]. Furthermore, Duggal MS et al., reported that different periods of etching time 15, 30, 45, and 60 seconds did not influence the retention rate of sealants used on the PFMs [34]. Hence, 37% phosphoric acid with an etching time of 15 seconds was used in the present study. The etched enamel surface was not completely air dried as it hampers the resin tag formation due to the collapse and denaturation of collagen fibrils forming amorphous material. To avoid the reduction in bond strength of the sealants due to saliva contamination, the use of a bonding agent before sealant application is recommended to improve retention and reduce microleakage [22,35-37]. Bonding agents are also sensitive to salivary contamination. Adsorption of salivary glycoproteins to the poorly polymerised adhesive layer prevents complete wetting of resin-based sealant and prevents adequate copolymerisation [15]. Patil SB et al., reported that a cured adhesive layer is contaminated with saliva, rinsing of the surface with water did not improve the detrimental effects of saliva contamination [26]. The long-term effects of saliva contamination are not specific. However, it was believed that contamination might cause nano-leakage within the hybrid layer.
There was some loss of marginal integrity of sealants in both groups. Furthermore, saliva contamination of the etched enamel surface before sealant placement is the most common reason for sealant failure [10,38,39], either in the rubber dam or cotton roll groups. Saliva contamination generally causes adhesive bond failures, fracturing at the enamel-resin interface [40], whereas, uncontaminated teeth most frequently show cohesive bond failures, occurring within the resin itself, leaving the bond intact [5,6]. Hence, fissure sealant’s long-term clinical success is closely related to effective moisture control at each stage of the application [41].
Limitation(s)
As the procedure is technique sensitive, inadvertent salivary contamination even after careful isolation, the experience of the operator and co-operation of the children during the procedure were considered as possible limitations of the present study.
Conclusion(s)
Retention of PFS in young permanent teeth was better when applied using rubber dam than cotton rolls for isolation, however, there was no statistical significance. Hence, proper isolation is considered as the key factor for the clinical success of PFS.
*Chi-square test; NS: Not significant
*Chi-square test; NS: Not significant
*Chi-square test; NS: Not significant