Isolated Fracture of the Corpus Spongiosum- A Rare Case with Atypical Presentation and Diagnostic Role of MRI
Selvin Theodore Jayanth1, Vivek Venkatramani2, Rajiv Paul Mukha3
1 Assistant Professor, Department of Urology, Christian Medical College, Vellore, Tamil Nadu, India.
2 Senior Consultant, Department of Urology, Nanavathi Hospital, Mumbai, Maharastra, India.
3 Professor, Department of Urology, Christian Medical College, Vellore, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Rajiv Paul Mukha, Professor, Department of Urology, Christian Medical College, Vellore, Tamil Nadu, India.
E-mail: mukhas@gmail.com
Penile fractures occur due to rupture of the corpora cavernosum or tunica albuginea secondary to blunt or sexual trauma to the erect penis. They typically present with rapid detumescence of the penis, with pain, swelling and ecchymosis. Approximately 10-20% of penile fractures involve the urethra. The report presents a 28-years-old male patient that complained of per-urethral bleeding, following an injury to an erect penis. With the help of MRI and intra-operative cystoscopy, found that the injury exclusively involved corpus spongiosum. He subsequently underwent a penile exploration and repair of the spongiosal defect. At one year follow up, he had normal erections with no per-urethral bleed. This is a rare form of presentation of penile fractures with only a few cases reported in literature. Surgical exploration remains the gold standard and early exploration is recommended to avoid erectile dysfunction, corporal fibrosis and urethral strictures and MRI is an useful adjunct.
Cystoscopy, Penile fracture, Spongiosal injury
Case Report
A 28-year-old male patient from southern India sustained an injury to his erect penis during sexual intercourse. He presented to the department the following week with complaint of per-urethral bleeding, especially notable following erections. He had no difficulty in passing urine. Patient was in good health with no significant medical or surgical history.
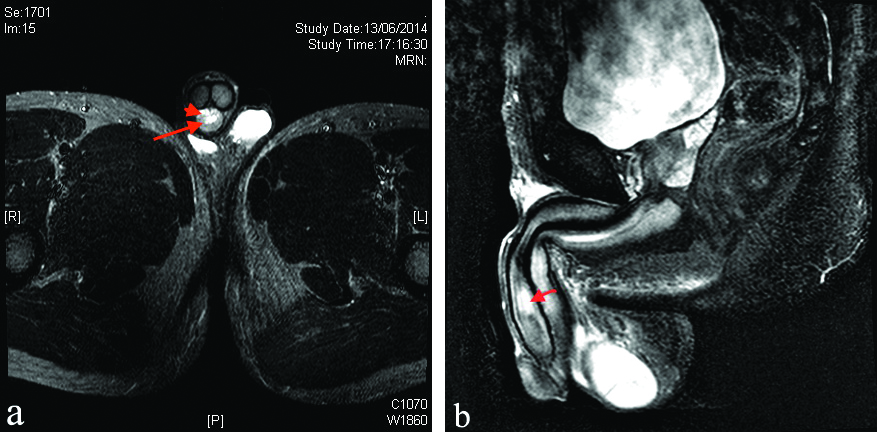
Clinical examination revealed a normal penis with no ecchymosis, palpable haematoma or blood at the meatus. The patient was noted to have tenderness on palpation of the ventral aspect of the distal penile shaft. Laboratory evaluation was unremarkable. Outpatient cystoscopy showed bullous oedema at the mid-penile urethra. An MRI of the erect penis revealed multiple hyperintense foci in the mid-portion of the corpus spongiosum on T2-weighted imaging suggestive of haemorrhage, with normal corpora cavernosa [Table/Fig-1].
(a) Transverse section of T2-weighted MRI showing central urethra (arrow) and surrounding hyperintense haemorrhage (arrowhead); (b) Sagittal section of T2-weighted MRI showing peri-urethral haemorrhage in the region of penile shaft.
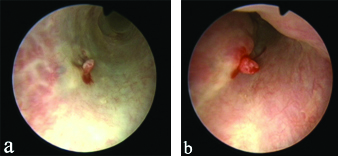
He was taken to the operating room for exploration and repair of a presumptive penile fracture. Urethroscopy revealed an area of haemorrhage and bullous oedema at the mid-penile urethra [Table/Fig-2a]. On injecting normal saline into the glans penis, there was a progressive bulge noted at the same site with some bleeding [Table/Fig-2b].
(a) Urethroscopy showing area of haemorrhage and oedema in the mid-penile urethra; (b) Urethroscopy after injection of normal saline into the glans revealing progressive bulge and bleeding from the same site.
Penile exploration was then undertaken, using a degloving incision. A defect was noted in the spongiosum which was closed primarily with 4-0 polyglactin over a Foley catheter. The catheter was removed after two weeks. At one year follow-up, the gentleman had no per-urethral bleeding and had normal erections.
Discussion
Penile fractures occur due to rupture of the corpora cavernosum or tunica albuginea secondary to blunt or sexual trauma to the erect penis [1]. Penile fractures typically present with rapid detumescence of the penis, with pain, swelling and ecchymosis. Approximately, 10-20% of penile fractures involve the urethra [2]. These fractures present similarity with associated urinary symptoms such as blood at the meatus, a positive urinalysis for blood and/or urinary retention [3]. The index patient complained of per-urethral bleeding following an injury to an erect penis. He was detected to have an injury that exclusively involved the corpus spongiosum [4].
Cerone JS et al., reported a patient with isolated corpora spongiosal injury following sexual trauma, but the patient presented with classical features of fracture penis (flaccid, detumescent penis) [5]. The present case may be just the second such report in the literature, and the first with this atypical clinical presentation. He had no clinically palpable penile fracture and an MRI raised the suspicion of spongiosal injury.
Magnetic Resonance Imaging (MRI) has been used to evaluate penile fractures; however its utility is questionable when the diagnosis is clear [6]. It can clearly demonstrate a tear in the tunica albuginea, which is noted as a discontinuity in the relatively hypointense tunica on T1-weighted imaging [7]. The extent and orientation of the tear can also be identified. High signal intensity on T2-weighted images is highly suggestive of intra-corporeal haemorrhage. Urethral and spongiosal involvement have also been identified using MRI [7]. A retrograde urethrogram has also been used to detect urethral involvement in cases of penile fracture and is usually recommended in patients who present with blood at the meatus, hematuria or voiding difficulty [6]. However, false negatives can occur and cystoscopy is a surer method of detection.
Conclusion(s)
Surgical exploration remains the gold standard for penile fracture and early exploration is recommended in clear cases to avoid erectile dysfunction, corporal fibrosis and urethral strictures. MRI is an useful adjunct.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 11, 2020
Manual Googling: Nov 29, 2020
iThenticate Software: Jan 27, 2021 (5%)
[1]. Jack GS, Garraway I, Reznichek R, Rajfer J, Current treatment options for penile fracturesRev Urol 2004 6(3):114-20. [Google Scholar]
[2]. Nymark J, Kristensen JK, Fracture of the penis with urethral ruptureJ Urol 1983 129(1):147-48.10.1016/S0022-5347(17)51967-9 [Google Scholar] [CrossRef]
[3]. Tsang T, Demby AM, Penile fracture with urethral injuryJ Urol 1992 147(2):466-68.10.1016/S0022-5347(17)37276-2 [Google Scholar] [CrossRef]
[4]. Eke N, Fracture of the penisBr J Surg 2002 89(5):555-65.10.1046/j.1365-2168.2002.02075.x11972544 [Google Scholar] [CrossRef] [PubMed]
[5]. Cerone JS, Agarwal P, McAchran S, Seftel A, Penile fracture with isolated corpus spongiosum injuryInt J Impot Res 2006 18:218-20.10.1038/sj.ijir.390138916151474 [Google Scholar] [CrossRef] [PubMed]
[6]. Kamdar C, Mooppan UMM, Kim H, Gulmi FA, Penile fracture: Preoperative evaluation and surgical technique for optimal patient outcomeBJU Int 2008 102(11):1640-44.10.1111/j.1464-410X.2008.07902.x18710448 [Google Scholar] [CrossRef] [PubMed]
[7]. Choi MH, Kim B, Ryu JA, Lee SW, Lee KS, MR imaging of acute penile fractureRadiographics 2000 20(5):1397-405.10.1148/radiographics.20.5.g00se05139710992029 [Google Scholar] [CrossRef] [PubMed]