Introduction
Chronic pain is one of the most neglected health problems throughout the world. A close association of depression with chronic pain adds to the burden. There is severe dearth of epidemiological studies regarding depression in chronic pain among general population in India.
Aim
To evaluate the prevalence of chronic pain among the selected rural population and to find out association between chronic pain and depression, if any.
Materials and Methods
This cross-sectional study was done with the objective of studying the relationships between socio-demographic factors, depression with characteristics of chronic pain among adult population in a community setting. Data was collected from 697 adult (>18 years) chronic pain (>12 weeks duration) sufferers chosen randomly with proportionate representation from all 81 villages of Amdanga block, West Bengal, through a household-based survey in cross-sectional design. A pre-designed, pre-tested structured questionnaire containing socio-demographic information where Brief Pain Inventory (BPI), Patient Health Questionnaire-9 (PHQ-9) and Physical Functional Ability Questionnaire (FAQ-5) were used. During analysis, indices representing perceived pain, impairment and functional ability were generated from the questionnaire by principal component analysis.
Results
Low Back Pain (LBP) was found to be significantly higher among females that is 57.7% (p-value=0.022), followed by knee pain (54.8%). Age (p<0.001), Educational level (p<0.001), Income (p<0.001) were found to be significantly associated with perceived pain, impairment, and functional ability, which again show significant monotonic relationship with severity of depression. Major Depressive Disorder (MDD) is found in 9.04% (95% CI: 7.95%-10.13%) of chronic pain sufferers.
Conclusion
Frequency of knee pain increases with aging, this points towards its degenerative nature. Perceived pain and impairment get higher while functional ability gets lower as the severity of depression increases.
Brief pain inventory, Major depressive disorder, Perceived pain, Suffering
Introduction
About one in five adults European [1], 17.1% of adult males and 20.0% of adult females in Australia [2] and 30.7% adults in United States of America [3] suffer from chronic pain. A pilot study of Vanderbilt Global Pain Survey, reported the point prevalence of chronic pain in India to be approximately 24% to 41% [4] while another telephonic survey estimated the prevalence to be 13% [5]. Though the duration of pain to be considered as chronic varied across researches, most frequently operationalised minimum duration is three months as recognised by International Association for the Study of Pain (IASP) in International Classification of Diseases (ICD) 11 [6]. Despite the Montreal Declaration stating “access to pain management a fundamental human right” [7], chronic pain remains one of the most underestimated health problems throughout the world [8]. Recognising any form of chronic pain as a symptom, where it needs to be considered as a disease itself and lack of proper epidemiological data regarding chronic pain [6], especially in the context of developing countries like India, adds to the problem.
On the other hand, depression, the single largest contributor to non-fatal health loss, led to a global total of over 50 million Years Lived with Disability (YLD) in 2015, where India alone contributed about 10 million YLD with 4.5 percent of total population suffering from depression [9]. Studies suggest that pain symptoms in depressed patients and depression in patients with pain occur more frequently than in general population [10]. Few studies regarding epidemiology of chronic pain are found from India and very few regarding depression in chronic pain [5,11]. Moreover, nearly all of them were either done in hospital settings or done in occupational cohorts. The researchers, thus, contemplated this study in a community setting, at a block of the most populated district of West Bengal (North 24 Parganas), with the following objectives:
To study the socio-demographic characteristics of adult chronic pain sufferers residing in a rural area of West Bengal; to estimate the prevalence of Major Depressive Syndrome among them and to study its relationship with various characteristics of chronic pain.
Materials and Methods
It was an observational descriptive study with cross-sectional design done at Amdanga Community Developmental Block, North 24 Parganas, West Bengal, chosen purposively, being the rural field practice area of the Department of Community Medicine, RG Kar Medical College, to which the researchers are attached. Study was carried out after Ethics Committee clearance of the institute. Informed consents were obtained from all participants. This is a part of a broad study done on various aspects of Mental Illness in that particular block. The time period was done from December 2016 to December 2017.
Inclusion criteria: Adults (>18 years) whose pains lasts or recurs persistently for more than three months and residing in the block for atleast six months, were included for the study.
Exclusion criteria: Individuals who are unwilling to give consent for the study or too sick to respond, were excluded from the study.
Sample size calculation: Considering the prevalence of MDD among patients with chronic pain, as estimated by Dutta D et al., as 30.67% [11], and taking level of alpha error to be 0.05, absolute error as 3.5%, the sample size came out to be 667. For better representation, all the villages (n=81) in the study area were included. Number of individuals to be selected from each village were decided by the formula of Probability Proportional to Size method i.e., {(sample size/total population of the block)} *population of the village as significant variation in village populations was noted. The resultant numbers were rounded up to the nearest whole numbers that gave the number of persons selected from each village. As a result, the final sample size of 697 was obtained.
Individuals were selected from the villages by “left hand thumb rule”. Consecutive houses were approached and one person from one household was interviewed until the required number from that village was met. This was done according to inclusion and exclusion criteria.
Study Tool
A pre-designed, pre-tested, structured schedule was used containing four sections.
Questions regarding socio-demographic characteristics of participants like age, sex, per capita income, occupation, etc.,
Brief Pain Inventory Questionnaire (BPI): for rapid assessment of intensity of pain and its impact on functioning, developed by Cleeland CS [12]. BPI has been previously validated in Indian context [13]. Sites affected by pain were noted in a human figure and other items were recorded in a10-point scale where 0 represented least and 10 highest.
Patient Health Questionnaire-9 (PHQ-9) was an inventory used as screening tool for depression. It is part of PHQ which is the self-administered version of the Primary Care Evaluation of Mental Disorders (PRIME-MD) developed by Kroenke K et al., [14]
Physical Functional Ability Questionnaire (FAQ-5): developed as a clinical assessment tool for patients with chronic pain and disability issues. It can provide a “snapshot” of the patient’s self-perception of his or her physical functional ability at one point in time without reference to pain perception [15].
Scores assigned against each response in BPI, PHQ-9 and FAQ-5 was added unweighted and final scores were interpreted as per the instructions in original questionnaire.
The schedule was translated into Bengali and again retranslated and checked for consistency. A group of experts of Community Medicine gave their inputs on these questions and ascertaining face validity. The conceptual, cultural, and semantic equivalence were well judged. Cronbach’s alpha was done to ascertain the convergent validity and was found to be 0.73. There were four properly trained interviewers, supervised regularly by faculties from the Department of Community Medicine to assure quality.
Statistical Analysis
Data was assembled in Microsoft Excel 2010 software and R software was used for statistical analysis. Continuous data were checked for normality and as they were found to be not following a normal distribution, they were represented by median and Inter Quartile Range (IQR). Chi-square test was done for seeing association in contingency tables. Kruskal Wallis test and Mann Whitney-U test were done for continuous data spread over more than two categories and two categories, respectively. Age was divided roughly on quartiles. Studies using confirmatory factor analysis to evaluate construct validity of the BPI suggested a better fit for a two-factor model than one factor model [16,17]. So, principal component analysis was done for parts of BPI questionnaire to derive “Perceived Pain Index (PPI)” for pain severity and “impairment index” for interference (With Eigen value as 1). Similarly, Functional ability index was also created from FAQ-5. A p-value less than 0.05 considered as significant.
Results
Out of the 697 respondents, 488 of the respondents, i.e., 70% were female. The median age of study population was 45 years with 25th percentile at 35 years and 75th percentile at 56 years. Most of the individuals completed primary education (42.6%) whereas 200 (28.7%) persons were illiterate. The median family income of the studied population was Rs. 5000 per month (IQR- Rs. 3000) [Table/Fig-1].
Distribution of study population according to their socio-demographic characteristics: (n=697).
| Socio-demographic characteristics | Number (Percentage) |
|---|
| Sex | Male | 209 (30) |
| Female | 488 (70) |
| Age (Years) | ≤35 | 189 (27.1) |
| 36-45 | 184 (26.4) |
| 46-55 | 149 (21.4) |
| More than 55 | 175 (25.1) |
| Education | Illiterate | 200 (28.7) |
| Literate | 92 (13.2) |
| Completed Primary Education | 297 (42.6) |
| Completed Secondary Education | 108 (15.5) |
| Occupation | Unskilled | 155 (22.2) |
| Skilled | 25 (3.6) |
| Clerk, Shop-owner, Farm-owner | 53 (7.6) |
| Semi-Professional | 4 (0.6) |
| Homemaker | 452 (64.8) |
| Unemployed | 8 (1.1) |
| Monthly income (Per month, in Rupees) | 3500 and below | 218 (31.3) |
| 3501-5000 | 207 (29.7) |
| 5001-6499 | 122 (17.5) |
| 6500 and above | 150 (21.5) |
The most frequently affected site was lower back (57.7%) followed by knees (54.8%). Frequency of low back pain was found to be significantly higher among females (60.2%) than males (51.7%) (p-value=0.022) but the frequency did not vary significantly across age groups; whereas knee pain showed no significant difference across sex but the percentage of affected individuals increased with advancing age [Table/Fig-2].
Distribution of Low back pain and knee pain across sex and age group; (There were some patients who suffered from both low back pain and knee pain).
| Parameters | Pain affecting lower back n1=402 (%) | p-value | Pain affecting knees n2=382 (%) | p-value |
|---|
| Sex | Male | 108 (51.7) | 0.022 | 113 (54.1) | 0.431 |
| Female | 294 (60.2) | 269 (55.1) |
| Age (Years) | ≤35 | 108 (57.1) | 0.193 | 57 (30.2) | <0.001 |
| 36-45 | 111 (60.3) | 102 (55.4) |
| 46-55 | 93 (62.4) | 87 (58.4) |
| >55 | 90 (51.4) | 136 (77.7) |
p-value less than 0.05 significant
Median PPI was 10.80 (Q1=6.36 and Q3=15.79), Median Impairment Index (II) was 13.99 (Q1=5.92 and Q3=23.44) and Median Functional Ability Index (FAI) was 13.36 (Q1=10.95 and Q3=14.97). An increasing trend in Perceived pain and Impairment and decreasing trend in functional ability was noted with advancing age and the differences across age groups were found to be significant (p-value <0.001). Among groups regarding educational status, illiterates had the maximum perceived pain. Impairment and minimum functional ability, different across the groups are statistically significant. Median perceived pain (9.88 in Non-depressed vs. 15.57 in Depressed) and median impairment (11.23 vs. 26.48) are way higher (p<0.001) in depressed persons while functional ability is significantly low (p<0.001) among them [Table/Fig-3].
Distribution of perceived pain, impairment and functional ability according to socio-demographic characteristics and presence and severity of depression: (n=697).
| Parameters | Perceived pain median (IQR) | p-value | Impairment median (IQR) | p-value | Functional ability median (IQR) | p-value |
|---|
| Sex | Male | 10.82 (9.37) | 0.716 | 13.15 (17.47) | 0.238 | 14.20 (2.70) | <0.001 |
| Female | 10.77 (9.44) | 14.12 (17.42) | 12.68 (3.46) |
| Age (Years) | ≤35 | 8.29 (9.12) | <0.001 | 7.04 (13.18) | <0.001 | 14.92 (2.39) | <0.001 |
| 36 to 45 | 10.47 (9.37) | 14.07 (16.95) | 13.38 (3.16) |
| 46 to 55 | 11.48 (8.30) | 15.89 (19.79) | 13.24 (3.88) |
| >55 | 12.56 (9.14) | 18.66 (16.70) | 10.95 (4.29) |
| Education | Illiterate | 13.13 (7.82) | <0.001 | 20.14 (17.36) | <0.001 | 11.08 (4.80) | <0.001 |
| Literate | 9.62 (10.99) | 16.90 (19.27) | 13.02 (3.33) |
| Completed Primary Education | 9.74 (8.76) | 11.13 (16.02) | 14.08 (3.15) |
| Completed Secondary Education | 9.58 (9.56) | 8.43 (15.52) | 14.25 (3.54) |
| Income (Per month, in Rupees) | <3500 | 11.73 (10.10) | <0.001 | 16.07 (18.18) | <0.001 | 12.64 (4.21) | <0.001 |
| 3501 to 5000 | 11.32 (9.85) | 15.57 (16.30) | 13.24 (4.02) |
| 5001 to 6499 | 10.81 (8.09) | 14.97 (18.96) | 13.50 (3.30) |
| >6500 | 9.00 (7.89) | 8.00 (16.02) | 14.24 (3.00) |
| Presence of depression | Not depressed | 9.88 (8.91) | <0.001 | 11.23 (16.25) | <0.001 | 13.52 (3.29) | <0.001 |
| Depressed | 15.57 (8.61) | 26.48 (15.28) | 10.35 (4.80) |
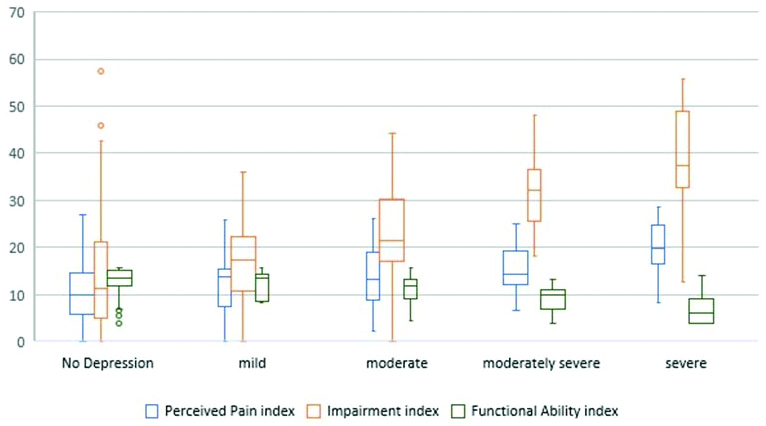
| Severity of depression (n=114) | Mild | 13.93 (8.10) | 0.003 | 17.31 (11.48) | <0.001 | 13.50 (5.72) | <0.001 |
| Moderate | 13.27 (10.22) | 21.51 (13.17) | 11.80 (4.10) |
| Moderately severe | 14.48 (7.26) | 32.28 (11.01) | 10.07 (4.05) |
| Severe | 19.87 (8.06) | 37.50 (16.23) | 6.12 (5.28) |
p-value less than 0.05 considered significant
Out of total 697 respondents, 583(83.6%) individuals had ‘no depression’, 14 (2.1%) had mild, 52(7.5%) had moderate, 31 (4.4%) had moderately severe and 17(2.4%) had severe depression. So, a total of 114 (16.36%) individuals were found to be depressed among whom 63 (55.26%) can be classified as with MDD, according to the prescribed criteria of PHQ-9. Thus, the prevalence of MDD is found to be 9.04 percent (95% CI: 7.95% to 10.13%). In present study, severity of pain increased with increasing severity of depression [Table/Fig-4].
Perceived pain, impairment and functional ability across severity of depression (n=697).
Discussion
Females were responding more in present study primarily because at the time of the household-based survey most of the men were in the workplace. That is why the prevalence of chronic pain is more in females, as suggested in a literature review by Fillingim RB et al., may also contribute [18]. The present study have compared the findings with some other studies to see the proportion of LBP [Table/Fig-5] [19-22]. Finding in this study is near to the study by Kar SK and Dhara PC, the difference may be explained by varying study population. LBP was found to be more common among females in present study, like studies by Banerjee A et al., Bihari V et al., Mohapatra A et al., [22-24]. In present study, LBP is not found to be associated with age, in contrast to studies by Tiwari RR et al., Koley S et al., Goon M et al., [25-27], where most of the study population were young. In present study, individuals more than 55 years of age showed less LBP, possibly because at this age, most of them had stopped heavy work and are not exposed to the occupational risk factors for LBP. Knee pain, the second most frequent, which 54.8% of the respondents were suffering, showed steady increase in presence with advancing age. This may indicate the degenerative nature of background knee pain pathology which has a strong association with age [28]. The Odds Ratio for knee pain in females, when adjusted for age rose from crude 1.04 (±0.17) to1.37(±0.18), which is in concordance with studies by Chia YC et al., Kim IJ et al., Pal CP et al., [29-31], (knee Osteoarthritis more common in females), but sex, in present study, did not predict presence of knee pain significantly (p=0.431).
The table shows the comparison of the findings of the present study with respect to previous studies with respect to proportion of Low Back Pain (LBP) [19-22].
| Authors | Study population | Sample size | Prevalence of LBP |
|---|
| Kar SK and Dhara PC (2007) [19] | Farmers in West Bengal | 400 | 48.8% |
| Sharma SC et al., (2003) [20] | Work-age adults of rural North India | 11234 | 23.09% |
| Haldiya KR et al., (2010) [21] | General population in Jodhpur district | 10015 | 6.2% |
| Banerjee A et al., (2012) [22] | General population in Pimpri, Pune | 2633 | 34.21% |
| Present study | General population in Amdanga | 697 | 57.7% |
Severity of chronic pain, as represented by Perceived Pain Index (PPI), impairment index and functional ability index, has associations with age, level of education and monthly family income. Urwin M et al., found a strong association of pain with social deprivation [28]. Study conducted in Southern Iran by Zarei S et al., showed significant association of pain with educational level and income [32]. Major depressive syndrome, as indicated by PHQ-9 [14], was found in 9.04%, the combined proportion of major and other depressive syndrome (taken as Depressed) is 16.36%. Studies suggesting prevalence of major depression are summarised in [Table/Fig-6] [11,33,34]. Variation from the study done in India by Dutta D et al., may be due the difference in study population, while it was a clinic-based survey, present study was household based. In present study, severity of pain increased with increasing severity of depression. This denotes a strong association of chronic pain and depression as found in other studies [10,11].
The table shows the comparison of the findings of the present study with respect to previous studies with respect to proportion of major depression [11,33,34].
| Authors | Sample size | Setting | Patients with depression |
|---|
| Magni G et al., [33] | 2341 | Population households | 16.4% |
| Von Korff M et al., [34] | 1500 | Health maintenance organisation enrolees | 5.9% to 10.7% |
| Dutta D et al., [11] | 476 | Pain clinic attendees | 30.7% |
| Present study | 697 | Population households | 16.36% |
Limitation(s)
Precise diagnosis of the respondents could not be made in absence of a clinical setting. Occupation could have played a role in explaining chronic pain, but it was found extremely difficult to categorise the study population in existing occupational categories.
Conclusion(s)
Low Back Pain (LBP) was most frequent followed by knee pain. LBP was more common in females and knee pain was increasingly common with aging. Severity of pain and interference with work increased with age and decreased with increasing level of education and income. Functional ability was higher among males, young adults and in persons with higher level of education and income. About 16.36% were found depressed and the severity of pain, its interference with work showed monotonic increase with advancing severity of depression. Functional ability declined with depression severity, as measured with PHQ-9.
p-value less than 0.05 significant
p-value less than 0.05 considered significant
Author Declaration:
Financial or Other Competing Interests: None
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Oct 31, 2020
Manual Googling: Feb 10, 2021
iThenticate Software: Feb 22, 2021 (17%)
[1]. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D, Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatmentEuropean Journal of Pain 2006 10(4):287-33.10.1016/j.ejpain.2005.06.00916095934 [Google Scholar] [CrossRef] [PubMed]
[2]. Blyth FM, March LM, Brnabic AJ, Jorm LR, Williamson M, Cousins MJ, Chronic pain in Australia: A prevalence studyPain 2001 89(2):127-34.10.1016/S0304-3959(00)00355-9 [Google Scholar] [CrossRef]
[3]. Johannes CB, Le TK, Zhou X, Johnston JA, Dworkin RH, The prevalence of chronic pain in United States adults: Results of an Internet-based surveyThe Journal of Pain 2010 11(11):1230-39.10.1016/j.jpain.2010.07.00220797916 [Google Scholar] [CrossRef] [PubMed]
[4]. Walters JL, Baxter K, Chapman H, Jackson T, Sethuramachandran A, Couldridge M, Chronic pain and associated factors in India and Nepal: A pilot study of the vanderbilt global pain surveyAnesthesia & Analgesia 2017 125(5):1616-26.10.1213/ANE.000000000000236028806206 [Google Scholar] [CrossRef] [PubMed]
[5]. Dureja GP, Jain PN, Shetty N, Mandal SP, Prabhoo R, Joshi M, Prevalence of chronic pain, impact on daily life, and treatment practices in IndiaPain Practice 2014 14(2):E51-62.10.1111/papr.1213224304963 [Google Scholar] [CrossRef] [PubMed]
[6]. Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, A classification of chronic pain for ICD-11Pain 2015 156(6):100310.1097/j.pain.000000000000016025844555 [Google Scholar] [CrossRef] [PubMed]
[7]. International Pain Summit of the International Association for the Study of PainDeclaration of Montreal: Declaration that access to pain management is a fundamental human rightJournal of Pain & Palliative Care Pharmacotherapy 2011 25(1):29-31.10.3109/15360288.2010.54756021426215 [Google Scholar] [CrossRef] [PubMed]
[8]. World Health Organisation supports global effort to relieve chronic pain. World Health Organisation 2017. [Internet]. [cited 11 December 2017]. Available from: http://www.who.int/mediacentre/news/releases/2004/pr70/en/ [Google Scholar]
[9]. Depression and other common mental disorders: Global health estimates. [Internet]World Health Organization 2017. [cited December 2017] [Google Scholar]
[10]. Bair MJ, Robinson RL, Katon W, Kroenke K, Depression and pain comorbidity: A literature reviewArchives of Internal Medicine 2003 163(20):2433-45.10.1001/archinte.163.20.243314609780 [Google Scholar] [CrossRef] [PubMed]
[11]. Dutta D, Bharati S, Roy C, Das G, Measurement of prevalence of ‘major depressive syndrome’ among Indian patients attending pain clinic with chronic pain using PHQ-9 scaleJournal of Anaesthesiology, Clinical Pharmacology 2013 29(1):7610.4103/0970-9185.10580823493638 [Google Scholar] [CrossRef] [PubMed]
[12]. Cleeland CS, Pain assessment in cancer. In: Osoba D, edEffect of cancer on quality of life 1991 Boca RatonCRC Press [Google Scholar]
[13]. Tan G, Jensen MP, Thornby JI, Shanti BF, Validation of the Brief Pain Inventory for chronic nonmalignant painThe Journal of Pain 2004 5(2):133-37.10.1016/j.jpain.2003.12.00515042521 [Google Scholar] [CrossRef] [PubMed]
[14]. Kroenke K, Spitzer RL, Williams JB, The PHQ-9: Validity of a brief depression severity measureGen Intern Med 2001 16:606-13.10.1046/j.1525-1497.2001.016009606.x11556941 [Google Scholar] [CrossRef] [PubMed]
[15]. Hooten WM, Timming R, Belgrade M, Gaul J, Goertz M, Haake B, Institute for Clinical Systems ImprovementAssessment and Management of Chronic PainUpdated November 2013. Available as: https://www.mnmed.org/getattachment/about-us/committees-task-forces/Prescription-OpioidTask-Force/Resources-for-physicians/ChronicPain.pdf.aspx?lang=en-US [Google Scholar]
[16]. Atkinson TM, Rosenfeld BD, Sit L, Mendoza TR, Fruscione M, Lavene D, Using confirmatory factor analysis to evaluate construct validity of the Brief Pain Inventory (BPI)Journal of Pain and Symptom Management 2011 41(3):558-65.10.1016/j.jpainsymman.2010.05.00821131166 [Google Scholar] [CrossRef] [PubMed]
[17]. Kumar SP, Utilization of brief pain inventory as an assessment tool for pain in patients with cancer: A focused reviewIndian Journal of Palliative Care 2011 17(2):10810.4103/0973-1075.8453121976850 [Google Scholar] [CrossRef] [PubMed]
[18]. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL, Sex, gender, and pain: A review of recent clinical and experimental findingsThe Journal of Pain 2009 10(5):447-85.10.1016/j.jpain.2008.12.00119411059 [Google Scholar] [CrossRef] [PubMed]
[19]. Kar SK, Dhara PC, An evaluation of musculoskeletal disorder and socioeconomic status of farmers in West Bangal, IndiaNepal Medical College Journal 2007 9(4):245-49. [Google Scholar]
[20]. Sharma SC, Singh R, Sharma AK, Mittal R, Incidence of low back pain in work age adults in rural North IndiaIndian Journal of Medical Sciences 2003 57:145-47. [Google Scholar]
[21]. Haldiya KR, Mathur ML, Mathur NC, Mathur A, Epidemiology of musculoskeletal conditions in IndiaAnnual Report 2009-2010, Dr. S.N. Medical College, Jodhpur 2010 Available from http://dmrcjodhpur.nic.in/AR09-10/P2-1.pdf [Google Scholar]
[22]. Banerjee A, Jadhav SL, Bhawalkar JS, Limitations of activities in patients with musculoskeletal disordersAnnals of Medical and Health Sciences Research 2012 2(1):05-09.10.4103/2141-9248.9692823209982 [Google Scholar] [CrossRef] [PubMed]
[23]. Bihari V, Keasavachandran C, Pangtey BS, Srivastva AK, Mathur N, Musculoskeletal pain and its associated risk factors in residents of National Capital RegionIndian Journal of Occupational and Environmental Medicine 2011 15(2):59-63.10.4103/0019-5278.9037522223951 [Google Scholar] [CrossRef] [PubMed]
[24]. Mohapatra A, Handoo SK, Gambhir IS, Mohapatra SC, Mohapatra SC, A study of non-communicable morbidity pattern in geriatric patients attending a referral railway hospital in Allahabad, Uttar PradeshNat J Commun Med 2011 2(2):191-95. [Google Scholar]
[25]. Tiwari RR, Mrinalini CP, Sanjay PZ, Low back pain among textile workersIndian Journal of Occupational and Environmental Medicine 2003 7(1):27-29. [Google Scholar]
[26]. Koley S, Kaur J, Sandhu JS, Biological risk indicators for non specific low back pain in young adults of Amritsar, Punjab, IndiaJournal of Life Sciences 2010 2(1):43-48.10.1080/09751270.2010.11885152 [Google Scholar] [CrossRef]
[27]. Goon M, Ghoshal S, Chandrasekaran B, Sharma BC, Prevalence of low back pain in long distance truck drivers of mountainous terrainAdvances in Occupational, Social and Organisational Ergonomics 2010 :516-22.10.1201/EBK1439835074-56 [Google Scholar] [CrossRef]
[28]. Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, Estimating the burden of musculoskeletal disorders in the community: The comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivationAnnals of the Rheumatic Diseases 1998 57(11):649-55.10.1136/ard.57.11.6499924205 [Google Scholar] [CrossRef] [PubMed]
[29]. Chia YC, Beh HC, Ng CJ, Teng CL, Hanafi NS, Choo WY, Ethnic differences in the prevalence of knee pain among adults of a community in a cross-sectional studyBMJ Open 2016 6(12):e01192510.1136/bmjopen-2016-01192527909033 [Google Scholar] [CrossRef] [PubMed]
[30]. Kim IJ, Kim HA, Seo YI, Jung YO, Song YW, Jeong JY, Prevalence of knee pain and its influence on quality of life and physical function in the Korean elderly population: A community based cross-sectional studyJournal of Korean Medical Science 2011 26(9):1140-46.10.3346/jkms.2011.26.9.114021935267 [Google Scholar] [CrossRef] [PubMed]
[31]. Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A, Epidemiology of knee osteoarthritis in India and related factorsIndian Journal of Orthopaedics 2016 50(5):51810.4103/0019-5413.18960827746495 [Google Scholar] [CrossRef] [PubMed]
[32]. Zarei S, Bigizadeh S, Pourahmadi M, Ghobadifar MA, Chronic pain and its determinants: A population-based study in Southern IranThe Korean Journal of Pain 2012 25(4):245-53.10.3344/kjp.2012.25.4.24523091685 [Google Scholar] [CrossRef] [PubMed]
[33]. Magni G, Marchetti M, Moreschi C, Merskey H, Luchini SR, Chronic musculoskeletal pain and depressive symptoms in the National Health and Nutrition Examination I. Epidemiologic follow-up studyPain 1993 53(2):163-68.10.1016/0304-3959(93)90076-2 [Google Scholar] [CrossRef]
[34]. Von Korff M, Dworkin SF, Le Resche L, Kruger A, An epidemiologic comparison of pain complaintsPain 1988 32(2):173-83.10.1016/0304-3959(88)90066-8 [Google Scholar] [CrossRef]